Introduction
Aloe vera is well known for its medicinal properties which lead to its application in treating various diseases. Its use in treating oral lesions has not been much documented in literature.
Aim
Although, systematic reviews on aloe vera and its extracts have been done earlier, but in relation to oral diseases this is the first systematic review. The aim of the present systematic review was to compile evidence based studies on the effectiveness of Aloe vera in treatment of various oral diseases.
Materials and Methods
Computerized literature searches were performed to identify all published articles in the subject. The following databases were used: PUBMED [MEDLINE], SCOPUS, COCHRANE DATABASE, EMBASE and SCIENCE DIRECT using specific keywords. The search was limited to articles published in English or with an English Abstract. All articles (or abstracts if available as abstracts) were read in full. Data were extracted in a predefined fashion. Assessment was done using Jadad score.
Results
Fifteen studies satisfied the inclusion criteria. Population of sample study ranged from 20 patients to 110 patients with clinically diagnosed oral mucosal lesions. Out of 15 studies, five were on patients with oral lichen planus, two on patients with oral submucous fibrosis, other studies were carried on patients with burning mouth syndrome, radiation induced mucositis, candida associated denture stomatitis, xerostomic patients and four were on minor recurrent apthous stomatitis. Most studies showed statistically significant result demonstrating the effectiveness of Aloe vera in treatment of oral diseases.
Conclusion
Although there are promising results but in future, more controlled clinical trials are required to prove the effectiveness of Aloe vera for management of oral diseases.
Introduction
Oral mucosa is the lining of the oral cavity which has a variety of functions, such as protection, sensation and secretion and histologically adapted to the unique environment inside the mouth. Oral health is important to the quality of life of individuals of all the age groups [1]. Oral lesions can lead to discomfort or pain that may hamper individual’s daily activities like mastication, swallowing, and speech which later may produce symptoms such as halitosis, xerostomia, or oral dysesthesia [2].
Espinoza et al., defined oral mucosal lesion as any change in oral mucosal surface that may present as red, white, ulcerative and pigmented lesions, any swelling or as variants of developmental defects [3]. There are various causes for oral mucosal lesions such as infection (bacteria, viruses, fungi, parasites), physical, chemical and thermal causes; immunological causes; systemic diseases; trauma; neoplasia; chronic habits such as the use of betel nut, tobacco and alcohol [4].
Ayurveda is India’s traditional natural system of medicine which today, has become one of the emerging treatment modality worldwide, for treating and preventing various oral and other diseases. Various ayurvedic gels, mouth washes etc. are used, since many years to treat oral health problems [5].
In today’s scenario when steroids and other drugs, having various adverse effects, are being commonly used for treating various oral diseases, scientist are searching for other modalities with equivalent potency and lesser or no ill-effects. Ayurvedic medications holds good result in this perspective, and among them aloe vera is one of the best choice which has multiple pharmacological effect with least adverse effect. This property of aloe vera has attracted attention of researchers as an alternative treatment modality in treating various oral diseases.
Aloe Vera (AV) is a cactus-like plant that grows readily in hot, dry climates. It belongs to the Liliacea family, of which there are about 360 species. Only two species are grown commercially: Aloe barbadensis Miller and Aloe aborescens. The parenchymatous cells in the fresh leaves of aloe vera secrete colorless mucilaginous gel (i.e., Aloe vera gel) that contains 98-99% water and 1-2% active compounds [Table/Fig-1] [6–9].
Constituents of aloe vera.
| Anthraquinones | Inorganic compounds |
|---|
| Aloin | Calcium |
| Barbloin | Sodium |
| Isobarbaloin | Chlorine |
| Anthranol | Manganese |
| Aloetic Acid | Zinc |
| Ester of cinnamic acid | Chromium |
| Aloe-emodin | Potassium sorbate |
| Emodin | Copper |
| Chrysophanic acid | Magnesium |
| Resistannol | Iron |
| Vitamins | Essential Amino acids |
| B1 | Lysine |
| B2 | Threonine |
| B6 | Valine |
| Choline | Leucine |
| Folic acid | Isoleucine |
| C | Phenylalanine |
| Alpha-tocopherol | Methionine |
| Beta -carotene | |
| Nonessential amino acids | Miscellaneous |
| Histidine | Cholesterol |
| Arginine | Triglycerides |
| Hydroxyproline | Steroids |
| Aspartic acid | Beta-sitosterol |
| Glutamic acid | Lignins |
| Proline | Uric acid |
| Glycine | Gibberellin |
| Alanine | Lectin-like-substance |
| Tyrosine | Salicylic acid |
| Arachidonic acid |
Aloe vera gel has various pharmacological actions like antibacterial, antifungal, anti-inflammatory, antioxidant, antitumour, hypoglycaemic properties and immune boosting. Therefore it is used traditionally as nutritional drinks, moisturizer, healing agent in cosmetics, diabetic patients, sun burn, wounds and digestive tract disorders, there is no adverse effect [10–15].
Aloe vera gel had also been used in dentistry and showed good results. It had been used for treatment of over extraction socket and endodontic medicament. Various dentifrices also contains Aloe vera gel as its constituent because of its medicinal property [16–18]. Studies have demonstrated that aloe vera has an important therapeutic uses in the management of oral lesions such as oral lichen planus, oral submucous fibrosis, radiation induced mucositis, burning mouth syndrome, xerostomia, recurrent apthous ulcers.
The clinical use of aloe vera is supported mostly by personal observations rather than scientific research data. Those reports are relevant for formulating hypotheses, but for defining its effectiveness more conclusively, controlled trials of aloe vera are essential. Therefore, the aim of this systematic review was to accumulate evidence based studies on aloe vera preparation and to evaluate its clinical effectiveness in treating various oral diseases.
Materials and Methods
Protocol: This review was planned and conducted in accordance with PRISMA guidelines.
Eligibility Criteria: Studies on aloe vera that is randomized control trials, single and double blind trials, cross-sectional and case control studies were included in this review. Studies were eligible only if they were published as full papers in English language. Animal studies were excluded in this review.
Literature Search: A systematic review of scientific literature concerning effectiveness of aloe vera on oral diseases was done in the manuscript. The electronic retrieval systems and data bases searched for relevant articles were PUBMED [MEDLINE], SCOPUS, COCHRANE DATABASE, EMBASE and SCIENCE DIRECT. The MEDLINE, science direct and SCOPUS search was performed from July 1998 till December 2015, and it was based on Mesh Terms. Database of indexed journals were searched for keywords such as Herbs, Ayurveda, Oral mucosa.
Study Selection: Authors searched for articles that met the before mentioned eligibility criteria. Later they reviewed the full title and abstract of the articles retrieved in the initial literature research. Differences among the reviewers, in the eligible studies were reviewed and resolved by mutual agreement.
The articles that were not matching eligibility criteria and duplicate articles were removed from the study. The abstracts of the remaining articles were screened individually. The authors tried to obtain the full papers for all the potentially eligible studies. The studies that met the eligibility criteria (when checked using the standard abstraction forms) were included in the systematic review.
Data Collection: On the basis of studies characteristics (title of the paper, author’s information, country in which the study was conducted, condition treated, study design, follow-up results, time to outcome measure) the author’s independently extracted data using the standard data extraction form. Differences were reviewed and resolved by mutual agreement between the authors. Data was extracted in predefined fashion and assessment of data was done using Jadad score [19].
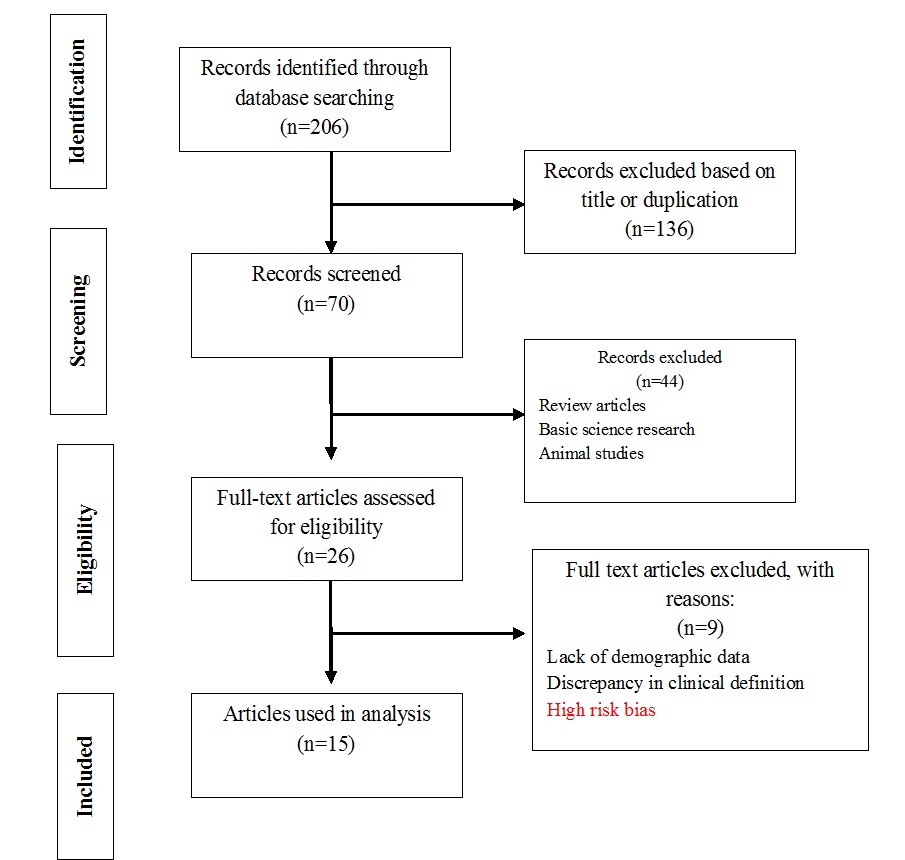
The initial computerized search strategy and associated hand search yielded 206 titles [Table/Fig-2]. In the first case selection observer screened the articles by reading titles and abstracts of the retrieved publications and 136 were discarded because those articles did not meet the inclusion criteria. Out of those 70 articles, 44 were excluded as they were animal studies, basic science research or review articles. Remaining 26 articles that fulfilled the eligibility criteria were read in full. Among these 26 articles, only 15 clinical trials met our inclusion criteria. Most of the studies included were carried out in hospital clinics of countries such as Iran, Spain, India, USA, and Saudi Arabia. Population of sample study ranged from 20 patients to 110 patients with clinically diagnosed oral mucosal lesions. Out of 15 studies five were on patients with oral lichen planus (OLP), two on oral submucous fibrosis, other studies were carried on patients with burning mouth syndrome, radiation induced mucositis, candida associated denture stomatitis, xerostomic patients and four minor recurrent apthous/stomatitis [Table/Fig-3]. Most studies showed statistically significant result demonstrating the efficacy of Aloe vera in treatment of oral lesions. Key data from these studies are summarized in [Table/Fig-3] [20–34].
Preferred reporting items for systematic review (PRISMA) diagram showing article selection for effectiveness of Aloe Vera in various oral disesases.
Clinical trials of Aloe Vera in treating oral mucosal lesions [20–34].
| Author(Year) | JadadScore(Max 5) | Conditiontreated | Design | Sample | Interventions | Primary end point | Main results |
|---|
| Garnick JJ et al., (1998) [20] | 5 | Recurrent apthous stomatitis | Case control study with cross over | -Study I (40 Patients) was performed to indicate the effect of each active substance and each combination-Study II (50 Patients), additional subjects were divided into 2 groups; one used a control gel with silicon dioxide, and the other a gel with all 3 active substances-In Study III (21 Patients), a modified crossover design was used with the subjects of study II | Effectiveness of a gel containing silicon dioxide, aloe vera, and allantoin in the healing of recurrent apthous stomatitis | Number and size of ulcers, length of the interval between ulcers, and pain from ulcers | Study I- statistical differences in the durations of lesions were present when all 3 substances were included in the gel.Study II - no statistical differences in the parameters when the 2 groups were comparedStudy III- a significant difference was found in lesion-free intervals and length of time for the studyAlteration in the occurrence of aphthous ulcers was demonstrated by the reduction in numbers of lesions in study I and by the increase in length of intervals between lesions in study III. |
| Choonhakarn C et al., (2008) [21] | 1 | Oral Lichen Planus | Randomized double blinded placebo controlled study | 54 patients5% aloevera gel for 8 weeks | Efficiency of aloe vera gel in treatment of oral lichen planus | Healing of lesionsBurning pain | Improvement of lesionsBurning improved in 9 patients (33%) |
| Sanchez et al., (2010) [22] | 5 | Oral Lichen Planus | Randomized double blinded placebo controlled study | 64 patients70% aloevera thrice daily for 12 weeks | Efficacy of topical aloe vera in patients in patients with oral lichen planus | Pain (VAS) and psychological assessment (OHIP 49) | Aloe vera group: complete pain remission 31.2 % of cases after 6 week, and 61% after 12 weeksSignificant differences between groups for OHIP49 |
| Amanat D et al., (2011) [23] | 2 | Oral Lichen palnus | Randomized double blinded Trial | 50 patientsGp 1-70% Apevera gelGp2-0.1% TAThrice daily for 8 weeks | Effect of Aloe vera versus local triamcnolone in treatment of oral lichen planus. | Pain,Lesion size | Outcomes were not clear, Pain was reduced with aloe vera, with partial remission of 30% |
| Mansourian A et al., (2011) [24] | 3 | Oral Lichen Planus | Randomized double blinded placebo controlled study | 46 patients | To compare the therapeutic effects of aloe vera mouthwash with triamcinolone acetonide (0.1%) on OLP | VAS for pain and burning sensation-Thong prasom index for clinical improvement and healing-Lesion size | Reduced VAS. Throngpransom score and size of lesions after treatment for both groups and after 2 months of discontinuation of treatment.Aloe vera group: 74 % of patients and triamcinolone acetonide group 78% of patients showed degrees of healing. |
| Reddy RL et al., (2012) [25] | 3 | Oral Lichen Planus | Randomized double blind trial | 40 patientsGp A-AV gelGpB-0.1% TAApply thrice daily for 8 weeks | Aloe vera gel versus triamcinolone acetonide ointment in the treatment of oral lichen planus | Pain, Burning sensation, and clinical appearance or erythema | Pain reduced and Thongprasom index was 0-1 for lesions. AV gel was found more effective than 0.1 % TA. |
| Sudarshan R et al., (2012) [26] | 3 | Oral submucous fibrosis | Randomized controlled trial | 20 subjectsGroup A (10 patients) AV group Apply 5mg thrice daily topically for 3 monthsGroup B (10 Patients) Antioxidant capsules twice daily for 3 months | To compare the efficacy of Aloe vera with antioxidants in the treatment for OSMF | Burning sensation, mouth opening, cheek flexibility | Aloe vera showed a statistically significant reduction in burning sensation, improvement in mouth opening and cheek flexibility as compared to antioxidant group |
| Bhalang et al., (2013) [27] | 5 | Apthous Ulcers | Randomized Trial | 100 subjects0.5% Acemannan thrice daily for 7 days | Effectiveness of Acemannan, in the treatment of oral Apthous Ulceration | Pain reduction, ulcer size, erythema | There was reduction in all the outcome measures but results were inferior to topical steroids |
| Alam S et al., (2013) [28] | 3 | Oral Submucous Fibrosis | Double-blind, placebo-controlled, parallel-group randomized controlled trial | 60 subjectsMedicinal treatment (submucosal injection of hyaluronidase and dexamethasone, Grade I & II OSMF n = 30) and surgical treatment (Grade III & IV OSMF n = 30) categories.Each category was randomly divided into groups A (with aloe vera, n = 15 per category, advised to applytopical aloe vera gel twice daily up to 6 month) andGroup B (without aloe vera, n = 15 per category) | Efficacy of aloe vera gel as an adjuvant treatment of Oral Submucous Fibrosis | Symptoms of oral submucous fibrosis such as burning sensation, mouth opening, pain associated with lesion, vesicles/ulcerations/erosion | Patients treated with aloe vera showed significant improvement in symptoms than non aloe vera group with both medicinal and surgical treatment |
| Mansour G et al., (2014) [29] | 3 | Minor recurrent apthous stomatitis | Randomized double blinded placebo controlled study | 99 patientsAloe Vera or Myrrh gelApply 4 times a day for five-seven days | Evaluate the clinical efficacy and safety of newly customized natural mouth oral mucoadhesives gels, containing either aloe vera or myrrh as active ingredients in management of minor recurrent apthous stomatitis | Change in ulcer size, pain, erythema, intensity at day 4 and 6 of study entry | Complete ulcer healing in 76.6% patients (subsidence of erythema 86.7% of them, subsidence of exudation 80% of them) |
| Babee et al., (2012) [30] | 4 | Recurrent apthous stomatitis | Double blinded clinical trial | 40 patients2% aloevera gel thrice daily over lesions for ten days | Evaluation of therapeutic effects of aloe vera gel on minor recurrent apthous stomatitis | Healing time (days after gel application), patient’s pain score; the lesion andits surrounding inflammation diameters | The durationof complete wound healing, pain score, wound size and inflammation zone diameter in the AV treated group were significantly lower than the control group . |
| Su K C et al., (2004) [31] | 1 | Radiation induced mucositis | Randomized double blinded placebo controlled study | 58 patients with head and neck cancer | Phase II double blind randomized study comparing oral aloe vera versus pacebo to prevent radiation related mucositis in patients with head and neck neoplasms | MucositisQulaity of life questionnaires | No statistical differences between two groups, oral aloe vera did not improve tolerance to head nad neck radiotherapy, decrease mucositis and improve patient well being. |
| Jornet PL et al., (2013) [32] | 5 | Burning Mouth Syndrome | Randomized double blinded placebo controlled study | 75 patientsGroup I- Tongue Protector three times a dayGroup II- Tongue protector 0.05 ml Aloe vera at 70% three times a dayGroup III- Tongue protector and 0.5 ml placebo three times a day | Evaluate the efficacy of aloe vera applied in combination with a tongue protector, comparing this with a placebo | VAS for pain and OHIP 49 for psychological assessment | VAS improved for all three groups and statistically significant differences between groups (p=0.210)Regarding OHIP 49 (overall clinical improvement was grater for group II |
| Shetty PJ et al., (2014) [33] | 0 | Candida associated Denture stomatitis | Cross-sectional | 50 patients | Anticandidal efficacy of denture cleansing tablet, triphala, aloe vera and cashew leaf on complete dentures of institutionalized elderly | Candida counts | Reduction in candida count was highest followed by triphala, aloe vera, cashew leaf and water |
| Morales-Bozo I et al., (2012) [34] | 4 | Xerostomia | Randomized control trial | 77 patientsRinse1(xylitol, sodium fluoride, cetylpyridinium chloride, sodium chloride and spearmint flavoring)Rinse 2 (same components as rinse 1, with the addition of propylene glycol, aloe vera, glycerine and citric acid) | Evaluation of the efficacy of two mouthrinses formulated for the relief of xerostomia | Burning tongue sensation, need to drink liquids to swallow and the sensation of swallowing difficulty were recorded | Mouthrinse 1 relieves sensation of dry mouth, need to drink liquids, and swallowing difficulty. In contrast, mouthrinse 2 relieves only latter two symptoms.Both rinses were more effective in relieving xerostomía-associated symptomatology in patients taking 3 or more medicines simultaneously. |
Risk of Bias across individual studies: All the studies demonstrated low risk bias using COCHRANE BIAS TOOL. Blinding Bias was low among all the studies except in one study [33]. Randomization sequence bias was high in seven studies [Table/Fig-4] [20–34].
Risk of Bias across individual studies [20–34].
| Disease | OLP | OLP | OLP | OLP | OLP | OSMF | OSMF | Apthous ulcers | Apthousulcers | ApthousUlcers | Apthous Ulcers | Xerostomia | BMS | Radiation Mucositis | Denture stomatitis |
|---|
| Authors | Garnickat al[20] | Choonhakaran et al., [21] | Salar sanchez et al., [22] | Amanat et al., [23] | Mansourian et al., [24] | Reddy RL et al., [25] | Sudarshanet al., [26] | Bhalang et al., [27] | Alam et al., [28] | Mansouret al., [29] | Babeeet al., [30] | Su et al., [31] | JornetPL[32] | Shetty PJ[33] | Morales-Bozo I et al., [34] |
|---|
| Year | 1998 | 2008 | 2011 | 2011 | 2011 | 2012 | 2012 | 2012 | 2013 | 2014 | 2012 | 2004 | 2023 | 2014 | 2012 |
| Randomization sequence | low Risk | High Risk | low Risk | High Risk | High Risk | High Risk | High Risk | Low Risk | Low Risk | High Risk | High Risk | Low Risk | Low Risk | Low risk | Low Risk |
| Allocation Concealment | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | Low risk | low Risk |
| Blinding of Participants | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | High risk | low Risk |
| Blinding of Patient reported outcome | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | High risk | low Risk |
| Blinding of outcome assessment | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | low Risk | questionable | low Risk | low Risk | Low risk | low Risk | High risk | low Risk |
| Short term attrition (<6 weeks), no of subjects | ------ | 14 | 3 | ----- | 0 | 0 | 0 | 0 | 0 | 0 | 9 | ----- | 0 | 0 | ----- |
| Long term attrition (>6 weeks), no of subjects | ------ | -------- | 9 | --------- | 0 | 0 | 0 | ----- | 0 | ----- | 0 | ------ | 0 | 0 | ------- |
OLP, Oral Lichen Planus; OSMF, Oral Submucous Fibrosis, BMS, Burning Mouth Syndrome
Clinical trials conducted to establish the efficacy of aloe vera in treating oral lesions.
Choonhakarn C et al., found that Apevera gel is more effective than placebo in clinical and symptomatological improvement of OLP [21]. Sanchez et al., also used topical aloe vera gel in OLP patients and found no adverse effects of aloe vera. In relation to quality of life, they found that there was significant difference between the aloevera and placebo groups [22]. Amanat D et al., compared the effectiveness of 70% aloe vera gel with 0.1% triamcinolone acetonide (TA) in the treatment of OLP lesions. Agents were applied topically 3 times daily for 8 weeks. Although pain associated with the lesion reduced with both agents but outcomes such as pain, burning sensation, lesion size were not clearly defined. Even the effectiveness of aloe vera and triamcinolone acetonoide (TA) was debatable [23]. Mansourian et al., in their study found that aloevera mouthwash could be an effective substitute for TA 0.1% in the treatment of OLP [24]. Reddy R et al., also conducted double blind randomized trial to compare the effectiveness of both agents in treatment of atrophic and erosive OLP and results demonstrated reduction of pain scores and burning sensation after 8 weeks of therapy but aloe vera was found to be superior than TA in their study [25].
Sudarshan R et al., found that aloevera when compared with antioxidant, had a better response in oral submucous fibrosis (OSMF) patients in all the parameters assessed and in all the clinicohistopathological stages particularly in those with mild-stage clinically and early-stage histopathologically [26]. Alam S et al., also conducted similar study in which they found that group receiving aloe vera had a significant improvement (during treatment and follow up period) in most symptoms of OSMF like burning sensation, mouth opening, tongue protrusion, cheek flexibility compared with the non–aloe vera group [28].
Some authors have found that it is effective in decreasing pain, size, erythema and exudation of ulcer. Though, some found it to be non effective. Study by Garnick JJ et al., gave contrasting results while testing the effectiveness of a gel containing silicon dioxide, aloe vera, and allantoin in the healing of Recurrent Apthous Stomatitis (RAS) [20]. Because 3 active substances which were present in the gel, a preliminary study (study I) was performed to indicate the effect of each active substance and each combination. The results of this study demonstrated that statistical differences in the durations of lesions (p= .017) were present when all 3 substances were included in the gel. In the next study (study II), which was initiated to test the results of study I, additional subjects were divided into 2 groups; one used a control gel with silicon dioxide and the other a gel with all 3 active substances. Study II found no statistical differences in the parameters when the 2 groups were compared. In study III, a modified cross-over design was used with the subjects of study II and a significant difference was found in lesion-free intervals (p = .0335) and length of time for the study (p = .0001). The differences in lesion intervals may have been caused by the differences in study length. Alteration in the occurrence of aphthous ulcers was demonstrated by the reduction in numbers of lesions in study I and by the increase in length of intervals between lesions in study III. However, a consistent pattern was not present; this indicated a lack of effect of the aloe vera gel on aphthous ulcers which was in contrast with other mentioned studies [20].
Bhalang et al., evaluated the effectiveness of acemannan, a polysaccharide extracted from aloe vera in the treatment of oral apthous ulceration and it was found that after 7 days of topical application there was reduction in ulcer size and associated pain but results were inferior to 0.1 % TA, but could be a effective alternative for patient is allergic to steroid medication [27].
Mansour et al., reported that mucoadhesive gel containing aloe vera as an active ingredient when used over fresh MiRAS, reduced ulcer size, erythema and exudation; whereas mucoadhesive gel containing myrhh as an active ingredient decreased the ulcer associated pain [29]. Babaee N et al., found that aloevera 2% oral gel is effective in decreasing the minor RAS patients’ pain score, wound size and wound healing period [30].
Aloe vera has antioxidant, anti-inflammatory and anti-tumour effects which could heal the lesions in oral mucositis patients. Ahmadi A postulated that Oral aloe vera mouthwash has anti –inflammatory and wound healing properties thus preventing the development of radiation induced mucositis. In addition it has antifungal and immunomodulatory properties, which prevents the establishment of oral candidiasis in the patients undergoing head and neck radiotherapy [35]. But contradicting this, Su et al., in their study concluded that oral aloe vera was not beneficial adjunct to head and neck radiotherapy and didn’t decreased mucositis or improved patients’ well being [31].
Aloe vera gel has been shown to have a significant anticandidal activity. Shetty PJ et al., evaluated the anticandidal efficacy of denture cleansing tablet, triphala, aloe vera and cashew leaf on complete dentures of 50 patients and candida count reduced maximum by use of triphala followed by aloe vera, cashew leaf and water (control) [33].
Jornet P L et al., hypothesized that the control of oral parafunctional habits together with application of topical aloe vera can protect the oral mucosa from repetitive trauma and decrease the discomfort associated with BMS [32].
Aloevera along with other ingredients (like salivary substitute & anticariogenic agents) is effective in relieving xerostomia associated symptoms [36]. Morales-Bozo I et al., formulated two rinses to relieve xerostomia. Rinse 1 was composed of an aqueous solution containing xylitol, sodium fluoride, cetylpyridinium chloride, sodium chloride and spearmint flavoring. Rinse 2 was composed of the same components as rinse 1, with the addition of propylene glycol, aloe vera, glycerine and citric acid. Both rinses were effective in relieving xerostomía-associated symptomatology [34].
Adverse Effects: No withdrawals owing to adverse effects of aloe vera were reported in any of the above clinical trials. Aloe vera was generally well tolerated by all patients.
Discussion
Aloe vera is used widely as a natural treatment and alternative therapy for various types of diseases and several studies have suggested the healing, cosmetic and nutritional benefits of this plant [37,38]. It has also been reported to possess anticancer activities which lead its usage in oral mucositis induced by patients with head and neck cancer undergoing radiotherapy [35]. Though aloe vera in literature has been reported to have significant medicinal value started from 1500 BC, clinical trials of aloe vera on oral diseases were published since 2002 though its effects in extra-oral applications were studied early from 1985. The clinical trial conducted in 2002 for alveolar osteitis was the earliest to be done for the maximum number of patients of about 1,194 in total while the other trials included only a few study groups [39].
Although few systematic reviews have been done on aloe vera and its extracts but we didn’t found any systematic review in relation to ‘use of aloe vera in oral mucosal disease’ in our search. We used Jadad score to assess the methodological quality of the clinical trials and only few studies reviewed were free of methodological flaws. Of all 15 trials included in this review, only six trials achieved the high methodological jaded score (4/5), rest trials achieved the jadad sore (0-3). Lack of randomization, lack of description of withdrawals, dropouts and method to generate the sequence of randomization and lack of double blinding were some prevalent limitations in other studies. Clinical trials demonstrated that aloevera was efficacious in treating oral lesions but it was most beneficial in OLP patients, but is debatable whether aloe vera is more effective than TA 0.1% for which further research is required [23]. All the five studies of OLP demonstrated low risk bias and proved aloe vera is effective therapeutic option for the reduction of lesion associated pain scores, and burning sensation with partial or complete remission of clinical symptoms in these patients [21–25].
In a clinical trial by Su et al., aloevera was found to be less beneficial in radiation induced mucositis patients for which further trials should be conducted. Aloevera was not effective in improving tolerance to head & neck radiotherapy, decreasing mucositis, and soreness. But the quality of life was improved in aloevera patient [31]. Though aloevera has anticandidal effect, it was less than Triphala as demonstrated in study by Shetty PJ et al., [33]. Studies conducted on OSMF patients proved that aloevera is effective in all clinicopathological stages of OSMF particularly in mild stage clinically and early stage histopathologically. The primary outcomes of pain and burning sensation in patients showed significant reduction and the overall quality of studies was considered to be good with low risk bias. The other outcome measures of mouth opening, cheek flexibility and tongue protrusion also appear to be promising in these studies [26,28]. Patil S et al., found aloe vera to be effective in the management of OSMF but the results of aloe vera were inferior to the other antioxidants used in its comparison. Since these studies had high risk bias we did not included it in our study [40–42]. Four trials were conducted on apthous stomatitis patients who evaluated 319 subjects. The overall quality of these studies was considered to be good, with the primary outcomes of pain and erythema, lesion size reduction and lesion healing, showing significant remission. Hence, aloe vera is effective in pain relief and lesion healing in apthous stomatitis [20,27,29,30].
Next question arises whether it could be used in other oral lesions or not and also about its safety. Topical application could lead to allergic reactions (due to anthraquinones, such as aloin and barbalion), episodes of contact dermatitis, burning and erythema. Ingestion of aloevera is sometimes associated with diarrhea, electrolyte imbalance (laxative action sometimes may lead to low potassium levels), worsening of constipation and conventional drug interactions [43,44]. However, these side effects are not seen in all patients. In the reviewed trials, no adverse effects were reported. Hence, it is recommended to choose an AV product, which is pure, stabilized, concentrated and grown organically.
Recommendations
Aloe vera gel has multiple and unique properties with great medicinal value and very less side effects, therefore it is definitely recommended in the treatment of various oral mucosal diseases.
Conclusion
Aloe vera has a wide spectrum of unique properties and uses and it is a promising agent in treating oral lesions yet in future more controlled clinical trials related to its dosage should be carried out to prove its effectiveness in various oral diseases.
OLP, Oral Lichen Planus; OSMF, Oral Submucous Fibrosis, BMS, Burning Mouth Syndrome
[1]. Bairwa R, Gupta p, Gupta VK, Srivastava B, Traditional medicinal plants: use in Oral hygieneIJPCS 2012 1:1529-38. [Google Scholar]
[2]. Patil S, Kaswan S, Rahman F, Dhoni B, Prevalence of tongue lesions in the Indian populationJ Clin Exp Dent 2013 5(3):e128-32. [Google Scholar]
[3]. Espinoza I, Rojas R, Aranda W, Gammol J, Prevalence of Oral mucosal lesions in Santiago, ChileJ Oral Pathol Med 2003 32:571-75. [Google Scholar]
[4]. Reichart PA, Oral mucosal lesions in a representative cross-sectional study of aging GermansCommunity Dent Oral Epidemiol 2000 28:390-98. [Google Scholar]
[5]. Ahuja A, Ahuja V, Yadav S, Garlic: A miraculous herb for oral diseases – a reviewJ Oral Health Community Dent 2014 8:51-54. [Google Scholar]
[6]. Reynolds T, Dweck AC, Aloe vera gel leaf: a review updateJ Ethnopharmacol 1999 68:3e37 [Google Scholar]
[7]. Newall CA, Anderson LA, Phillipson JD, Herbal medicinesA guide for health-care professionals 1996 LondonThe Pharmaceutical Press [Google Scholar]
[8]. Femenia A, Sanchez ES, Simal S, Rossello C, Compositional features of polysaccharides from Aloe vera (Aloe barbadensis Miller) plant tissuesCarbohydr Polym 1999 39:109e117 [Google Scholar]
[9]. Xing JM, Li –FF, Purification of aloe polysaccharides by using aqueous two phase extraction with desalinationNat Prod Res 2009 23:1424-30. [Google Scholar]
[10]. Vazquez B, Avila G, Segura D, Esclanate B, Antiinflammatory effects of extracts from aloe verav gelJ Ethnopharmacol 1995 54:69-75. [Google Scholar]
[11]. Lorenzetti LJ, Salisbury R, Beal JL, Baldwin JN, Bacteriostatic properties of aloe veraJ pharma Sci 1964 53:1287 [Google Scholar]
[12]. Yagi A, Kabash A, Okamura N, Haraguchi H, Moustafa SM, Khalifa TI, Antioxidants, free radical scavenging and anti-inflammatory effects of aloesin derivatives in Aloe VeraPlanta Med 2002 68:957-60. [Google Scholar]
[13]. Im SA, Lee Yr, Lee Yh, Invivo evidence of the immunomodulatory activity of orally administered Aloe vera gelArch Pharm Res 2010 33:451-56. [Google Scholar]
[14]. Kim K, Kim H, Kwon J, Hypoglycaemic nad hypolipidemic effects of processed Aloe Vera gel in a mouse model of non insulin dependent diabetes mellitusPhytomedicine 2009 16:856-83. [Google Scholar]
[15]. Langmead L, Makins RJ, Rampton DS, Antiinflammatory effects of aloe vera gel in human colorectal mucosa in vitroArch Pharm Res 2010 33:451-56. [Google Scholar]
[16]. Poor MR, Hall JE, Poor AS, Reduction in the incidence of alveolar osteitis in patients treated with the salicept patch containing Acemann hygrogelJ Oral Maxillofac Surg 2002 60:374-79. [Google Scholar]
[17]. Wadhawan R, Khan SDDA, Solanki G, Sabir S, Aloe vera: boon in dentistryInt J Pharm Res Rev 2014 4:147-51. [Google Scholar]
[18]. George D, Bhat SS, Antony B, Comparative evaluation of antimicrobial efficacy of aloe vera tooth gel asnd two popular commercial toothpastes. An in vitro studyGen Dent 2009 238-41. [Google Scholar]
[19]. Jadad AR, Moore RA, Carol D, Assessing the quality of randomized controlled trials: Is blinding necessary?Controlled Clin trials 1996 17:1-12. [Google Scholar]
[20]. Garnick JJ, Singh B, Winkley G, Effectiveness of a medicament containing silicon dioxide, aloe, and allantoin on aphthous stomatitisOral Surg Oral Med Oral Pathol Oral Radiol Endod 1998 86:550-56. [Google Scholar]
[21]. Choonhakarn C, Busaracome P, Sripanikulchai B, Sarakarn P, The efficacy of aloe vera gel in the treatment of oral lichen planus: a randomized controlled trialBr J Dermatol 2008 158:573-77. [Google Scholar]
[22]. Salazar-Sánchez N, López-Jornet P, Camacho-Alonso F, Sánchez-Siles M, Efficacy of topical Aloe vera in patients with oral lichen planus: a randomized double-blind studyJ Oral Pathol Med 2010 39:735-40. [Google Scholar]
[23]. Amanat D, Bahri NR, Tazaesh L, Effect of Aloe vera versus local triamcnolone in treatment of oral lichen planusShiraz Univ Dent J 2011 12:206-13. [Google Scholar]
[24]. Mansourian A, Momen-Heravi F, Saheb Jamee M, Esfehani M, Khalilzadeh O, Momen Beitollahi J, Comparison of aloe vera mouthwash with triamcinolone acetonide 0.1% on oral lichen planus: a randomized double blinded clinical trialAm J Med Sci 2011 342:447-50. [Google Scholar]
[25]. Reddy RL, Reddy RS, Ramesh T, Singh TR, Swapna LA, Laxmi NV, Randomized trial of aloe vera gel versus triamcinolone acetonide ointment in the treatment of oral lichen planusQuintessence International 2012 43:793-800. [Google Scholar]
[26]. Sudarshan R, Annigeri RG, Sree Vijayabala G, Aloe vera in the treatment for oral submucous fibrosis - a preliminary studyJ Oral Pathol Med 2012 41:755-61. [Google Scholar]
[27]. Bhalang K, Thunyakitpisal P, Rungsirisatean N, Acemannan, a polysaccharide extracted from aloe vera is effective in the treatment of oral Apthous UlcerationJ Altern Complement Med 2013 19:229-34. [Google Scholar]
[28]. Alam S, Ali I, Giri KY, Gokkulakrishnan S, Natu SSS, Faisal M, Efficacy of aloe vera gel as an adjuvant treatment of oral submucous fibrosisOral Surg Oral Med Oral Pathol Oral Radiol 2013 117:717-24. [Google Scholar]
[29]. Mansour G, Ouda S, Shaker A, Abdallah HM, Clinical efficacy of new aloe vera- and myrrh-based oral mucoadhesive gels in the management of minor recurrent aphthous stomatitis: a randomized, double-blind, vehicle-controlled studyJ Oral Pathol Med 2014 43:405-09. [Google Scholar]
[30]. Babaee N, Zabihi E, Mohseni S, Moghadamnia AA, Evaluation of the therapeutic effects of Aloe vera gel on minor recurrent aphthous stomatitisDent Res J 2012 9:381-85. [Google Scholar]
[31]. Su CK, Mehta V, Ravikumar L, Shah R, Pinto H, Halpern J, Phase II double-blind randomized study comparing oral Aloe vera versus placebo to prevent radiation-related mucositis in patients with head-and-neck neoplasmsInt J Radiat Oncol Biol Phys 2004 60:171-77. [Google Scholar]
[32]. Jornet PL, Camacho–Alonso F, Molino-Pagan D, Prospective, randomized, double blind, clinical evaluation of Aloe Vera Barbadensis, applied in combination with a tongue protector to treat burning mouth syndromeJ Oral Pathol Med 2013 42:295-301. [Google Scholar]
[33]. Shetty PJ, Hegde V, Gomes L, Anticandidal efficacy of denture cleansing tablet, Triphala, Aloe vera, and Cashew leaf on complete dentures of institutionalized elderlyJ Ayurveda Integr Med 2014 5:11-4. [Google Scholar]
[34]. Morales-Bozo I, Rojas G, Ortega-Pinto A, Espinoza I, Soto L, Plaza A, Evaluation of the efficacy of two mouthrinses formulated for the relief of xerostomia of diverse origin in adult subjectsGerodontology 2012 29(2):e1103-12. [Google Scholar]
[35]. Ahmadi A, Potential Prevention: Aloe vera mouthwash may reduce radiation induced oral mucositis in head and neck cancer patientsChin J Integr Med 2012 18:635-80. [Google Scholar]
[36]. Beyari M, Dar–Odeh N, Natural remedies for dry mouth associated with nonfunctioning salivary glandsJ Her Med 2015 5:113-17. [Google Scholar]
[37]. Dal Belo SE, Gasper LR, Campos PMBGM, Moisturizing effect of cosmetic formulations containing Aloe vera extract in different concentrations assessed by skin bioengineering techniquesSkin Res Technol 2006 12:241-46. [Google Scholar]
[38]. Heggers JP, Kucukcelebi A, Listengarten D, Stabenau J, Ko F, Broemeling LD, Beneficial effects of aloe on wound healing in an excisional wound modelJ Altern Complement Med 1996 2:271-77. [Google Scholar]
[39]. Poor MR, Hall JE, Poor AS, Reduction in the incidence of alveolar osteitis in patients treated with SaliCept Patch, containing acemannan hydrogelJ Oral Maxillofac Surgery 2002 60:374-79. [Google Scholar]
[40]. Patil S, Al Zeera BK, Sahu R, Comparative study of natural antioxidants spirulina and aloe vera for the treatment of oral submucous fibrosisJ Oral Biol Craniofac Res 2015 5:11-15. [Google Scholar]
[41]. Patil S, Halgatti V, Maheshwari S, Santosh BS, Comparative study of the efficacy of herbal antioxdants oxitard and aloe vera in the treatment of oral submucous fibrosisJ Clin Exp Dent 2014 6(3):e265-70. [Google Scholar]
[42]. Patil S, Sghaireen MG, Maheshwari S, Kunsi SR, Sahu R, Comparative study of the efficacy of lycopene and aloe vera in the treatment of oral submucous fibrosisInt J Health Allied Sci 2015 4:13-17. [Google Scholar]
[43]. Moore TE, The M and M’s of Aloe vera- Is it for dentistry ?J Okla Dent Assoc 2001 91:30-31. [Google Scholar]
[44]. Mangaiyarkarasi SP, Manigandan T, Elumalai M, Cholan PK, Kaur RP, Benefits of Aloe vera in DentistryJ Pharm Bioallied Sci 2015 7:255-59. [Google Scholar]