Maximal opening of mouth is described as the greatest distance between incisal edge of maxillary central incisor to the incisal edge of mandibular central incisor, when the mouth is opened as wide as possible painlessly or as the inter incisal distance plus the overbite [1].
Dental infections, craniofacial malignancies, fractures and myopathies in the head and neck region and many other reasons may contribute to the cause of reduced mouth opening [2]. All clinicians dealing with the oral cavity face various problems when there is a limited mouth opening [3].
Any restriction in mandibular mobility is commonly accepted as one of the main signs of mandibular dysfunction, and so it is an important criterion for the evaluation of functional state of the masticatory system. Clinical measurement of normal range of Maximum Mouth Opening (MMO) is an important diagnostic tool for evaluation of stomatognathic system, especially in those who have suspected temporomandibular dysfunctions and neurogenic dysfunctions. MMO can also be helpful in providing necessary information for designing of dental instruments/prosthesis [4].
In order to make a diagnosis of decreased mouth opening, it is essential that we know the range of normal mouth opening for that particular population. Previous investigations have shown that the range of mandibular movement varies considerably among individuals on the basis of age, sex, weight and height [4]. Helkimo’s Clinical Dysfunction Indices are based on the limit of 40mm for maximum mouth opening and 7mm for other horizontal mandibular movements [5]. His system does not allow any differentiation in mobility values between the two sexes, among people of different ages and different statures. Yao et al., and Hirsch et al., came to a conclusion that MMO reduces with age and females have lower MMO when compared to males of same age [6,7]. On the contrary, Landtwing has stated that mouth opening correlates significantly less with age than with stature [8]. Gallagher found no link between mouth opening and stature in his study conducted on Irish adult population [9].
The rationale behind finding a relation between MMO and facial type was that, several studies have found a relation between facial musculature and its effect on arch width and also on facial type [10,11]. It is seen in general that individuals with strong and thick elevator muscles have a euryproscopic face type [10]. Satiro Glu et al., found that individuals with vertically short facial pattern had thick masseter and those with long face had thin masseter [11]. Since, MMO is the combined result of movement of temporo-mandibular joint (TMJ) and action of mandibular musculature, this study was carried out to see whether facial type; which is indirectly influenced by musculature has got any correlation with mouth opening or not [12].
Keeping the aforesaid studies in mind, the present study was done to obtain the normal range of maximal mouth opening in children without any functional disturbances of the masticatory system and to examine the possible relationship of maximal mouth opening with age, gender, height, body weight and different facial types.
Materials and Methods
The present cross-sectional study was undertaken in the Department of Pedodontics and Preventive Dentistry, Dr. R Ahmed Dental College and Hospital over a period of three months after obtaining Ethical Clearance. It was carried out over a sample of 434 children, after obtaining informed consent from their parents/guardians, to determine if any correlation exists with age, sex, height, body weight and different facial types. The sample size was determined on the basis of previous studies [2,3].
Inclusion Criterion: Children with no history of jaw, head, or facial trauma having fully erupted maxillary and mandibular central incisors. Children with no history of pain in the jaw, face, or neck, either at rest or during function. Children with no history of bruxism. Children with no facial or dental abnormalities. Children with no history of temporomandibular joint sounds. Children with no dental prosthesis on anterior teeth.
Exclusion Criterion: Children with missing maxillary or mandibular incisors. Children with broken maxillary or mandibular incisors due to any reason. Children with severe orthodontic problems (anterior cross bite, proclination/retroclination of incisors etc.) Children with muscular, neurological disorders and craniofacial deformities. Children with neck pain and systemic diseases (juvenile rheumatoid arthritis), which have been reported to create limited mouth opening.
Depending on age, participants were divided into 3 groups:
Group 1: Age Group 6-8 years
Group 2: Age Group 8.1-10 years
Group 3: Age Group 10.1-12 years
Patient history was taken. A questionnaire was given to parent or guardian of the patient at the time of clinical oral examination. The pre tested, structured questionnaire consisted of demographic information of each child. Information collected included age, gender, any previous history of trauma, tenderness or clicking sound at rest or during jaw movements and any head and neck disorders. In addition to these, a proper history of conditions that could affect the child’s ability to open his/her mouth such as systemic diseases, neurological disorders, or craniofacial deformities was also collected from the child’s parents.
Clinical examination consisted of general dental examination, inspection of the pre-auricular area to look for any swelling, erythema, or tenderness. This was followed by palpation directly over the TMJ when the child opened and closed his mouth. The assessment of the extent of the mandibular condylar movement and auscultation of TMJ were also done at the same time. This was followed by auscultation and palpation of masticatory and cervical muscles.
The amount of mandibular opening was measured using the distance between the incisal edges of upper and lower anterior teeth. Any deviation of mandible during opening and closing was also observed. MMO was recorded using a modified Vernier Caliper [Table/Fig-1], with children resting their heads against a firm wall/surface in an upright position [Table/Fig-2]. Children were asked to open their mouth as wide as possible, while the examiner measured the maximum distance from the incisal edge of the maxillary central incisor to incisal edge of mandibular central incisor at the midline.
Modified vernier caliper.

Measurement of maximum mouth opening using modified vernier caliper.

For each child, the examiner took three readings of MMO in millimeters (mm) and the mean of the three readings was considered so as to reduce intra-examiner error. In order to increase the reliability and reproducibility of MMO measurement, a notch was made on the outer border of both the jaws of digital vernier caliper so as to make the incisors rest on the notch at the same point on different attempts. While modifying the vernier caliper, a new formula was derived in which the final reading was obtained after adding the actual reading with the total distance between two notches (i.e., 12mm).
Final Reading = Original Reading + 12mm
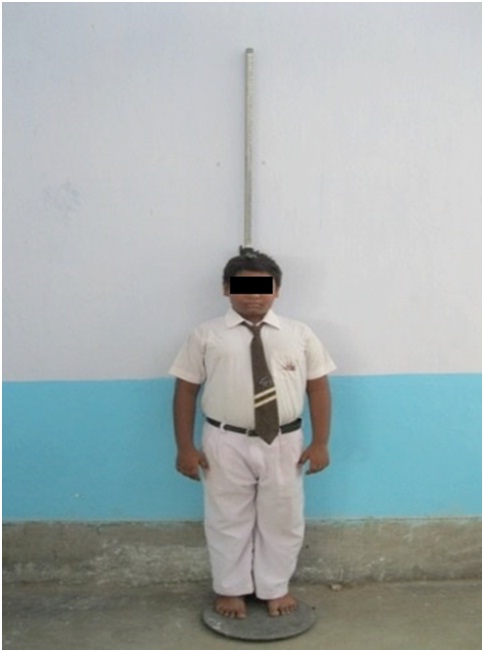
The height and weight of participating children was determined, with children being dressed in light clothing without shoes. Standing height (in centimeters) was measured using a wall mounted stadiometer [Table/Fig-3]. Weight was determined in kilograms using digital weighing machine [Table/Fig-4].
Measurement of height using stadiometer.
Measurement of weight using digital weighing machine.

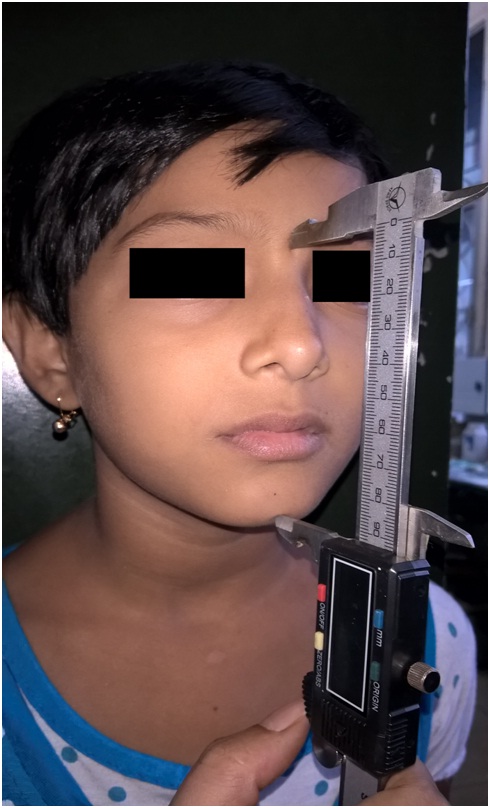
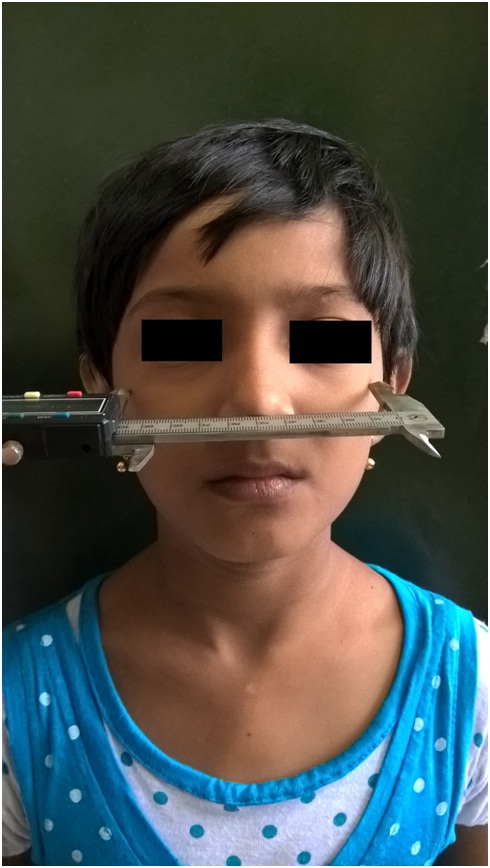
Morphological facial length (nasion – gnathion) [Table/Fig-5] and morphological facial width (bizygomatic width) were measured using sliding caliper [Table/Fig-6].
Measurement of facial height using a sliding caliper.
Measurement of facial width using sliding caliper.
Facial Index was determined by using formula [13]

Based on the calculated facial index, facial type was determined using Martin & Sallers’ scale [13],
Euryprosopic: 79- 83.9
Mesoprosopic: 84-87.9
Leptoprosopic: 88-92.9
All measurements were performed by a single examiner in order to avoid inter examiner variability. The measurements of MMO were compared among children of different age groups and facial types. Similarly, correlation between the MMO and sex, body weight and height was also calculated. Pearson correlation was used to determine the relationship between the different parameters. p-value <0.05 was the bench mark for statistical significance in the analysis. Descriptive and inferential analysis was done for the data using SPSS version 20.0. (SPSS 20, inc.; Chicago).
Results
MMO was measured in boys and girls in the age range of six to twelve years. Results are shown in [Table/Fig-7,8].
Maximum Mouth Opening (mm), Height (cm) and Body Weight (kg) in boys and girls of age six to twelve years.(Data presented as Mean±SD).
| Age Group | Facetype | Gender | Weight (mean±SD) | Height (mean±SD) | MMO (mean±SD) |
|---|
| 6-8 years | Euryprosopic | Female (38) | 20.63±3.61 | 113.48±8.15 | 41.14±4.29 |
| Male (17) | 23.59±2.55 | 117.86±6.09 | 42.16±3.98 |
| Leptoproscopic | Female (21) | 21.90±3.80 | 117.42±9.08 | 42.12±4.54 |
| Male(14) | 23.09±4.61 | 117.70±7.48 | 43.76±3.80 |
| Mesoproscopic | Female (26) | 21.89±3.69 | 113.98±7.29 | 41.77±4.09 |
| Male (23) | 22.33±4.38 | 118.29±7.60 | 42.51±3.95 |
| 8.1-10 years | Euryprosopic | Female (31) | 29.45±8.17 | 127.22±7.37 | 44.42±4.69 |
| Male (30) | 30.31±7.68 | 125.82±8.28 | 43.30±4.11 |
| Leptoproscopic | Female (21) | 26.69±6.83 | 125.53±8.03 | 43.02±3.92 |
| Male (27) | 27.13±6.12 | 126.96±7.25 | 46.29±3.09 |
| Mesoproscopic | Female (19) | 25.63±5.01 | 125.14±8.37 | 42.50±4.32 |
| Male (15) | 29.13±6.77 | 125.40±7.34 | 42.80±5.16 |
| 10.1-12 years | Euryprosopic | Female (33) | 35.33±8.56 | 134.28±8.27 | 44.63±5.28 |
| Male (28) | 32.66±6.86 | 134.76±5.86 | 45.80±5.18 |
| Leptoproscopic | Female (22) | 29.73±3.91 | 134.10±6.28 | 45.76±4.98 |
| Male (33) | 31.33±6.01 | 137.04±8.75 | 46.28±4.68 |
| Mesoproscopic | Female (21) | 32.90±7.45 | 136.91±9.26 | 45.32±5.80 |
| Male (15) | 36.03±10.15 | 136.10±10.01 | 46.03±5.86 |
Pearson’s correlation test showing correlation using between MMO (mm), Height (cm), Body Weight (kg) and facial types in boys and girls of all age groups
| Facetype | Parameter | Age | Weight | Height | MMO |
|---|
| Euryprosopic | Age | 1 | 0.613** | 0.774** | 0.310** |
| Weight | 0.613** | 1 | 0.730** | 0.303** |
| Height | 0.774** | 0.730** | 1 | 0.326** |
| MMO | 0.310** | 0.303** | 0.326** | 1 |
| Leptoproscopic | Age | 1 | 0.580** | 0.710** | 0.308** |
| Weight | 0.580** | 1 | 0.710** | 0.152 |
| Height | 0.710** | 0.710** | 1 | 0.156 |
| MMO | 0.308** | 0.152 | 0.156 | 1 |
| Mesoproscopic | Age | 1 | 0.129 | 0.178 | 0.057 |
| Weight | 0.129 | 1 | 0.744** | 0.373** |
| Height | 0.178 | 0.744** | 1 | 0.302** |
| Mmo | 0.057 | 0.373** | 0.302** | 1 |
**. Correlation is significant at the 0.01 level (2-tailed).
Age Group 6-8 years: MMO was weakly directly proportional to age, height & weight in euryproscopic and leptoproscopic face type children (p-value>0.05), whereas in mesoproscopic face type children MMO was weakly directly proportional to age & weight and weakly inversely proportional to height (p-value>0.05).
Age Group 8.1 - 10 years : MMO was weakly indirectly proportional to age, weakly directly proportional to height (p-value>0.05) and weakly directly proportional to weight (p-value <0.05) in euryproscopic face type children, whereas in leptoproscopic and mesoproscopic face type children MMO was weakly indirectly proportional to age and weakly directly proportional to weight & height (p-value>0.05).
Age Group 10.1-12 years: MMO was directly proportional to age & height (p-value<0.05) and directly proportional to weight (p-value>0.05) in euryproscopic face type children. In leptoproscopic face type children MMO was directly proportional to age but inversely proportional to weight and height (p-value>0.05), whereas in mesoproscopic face type children MMO was weakly directly proportional to age, height (p-value>0.05) & weight (p-value <0.05).
For whole sample of 434 children, children having euryproscopic face type MMO was directly proportional to age, weight and height (p-value <0.05). In children with leptoproscopic face type MMO was directly proportional to age (p-value < 0.05), height and weight (p-value > 0.05). In mesoproscopic face type children type MMO was directly proportional to age (p-value > 0.05), weight and height (p-value < 0.05).
Discussion
The present study revealed MMO in children of 6-8, 8.1-10 and 10.1-12 years age group. The values obtained go well with the values, 46.0 and 46.2 mm, which were given by Nevakari [5] and Shephard and Shephard [14] respectively, for children in the age group of six to ten years. Contrary to the above results, Vanderas and Ingervall [15] reported higher values of MMO in children between the age of six to ten years which were 54.8 mm and 51.3 mm, respectively.
As already mentioned, MMO is described either as the inter-incisal distance [1,5,16–18] or as the sum of inter-incisal distance and overbite [19]. An advantage of using inter incisal distance for MMO measurement is that the measuring point is more easily determined and is relatively more permanent in terms of reproducibility.
Head position also plays a very important role in determining MMO [20,21]. Values of MMO were seen to vary in forward, natural or retracted head positions in a study conducted by Higbie et al., [22]. Thus, in the present study, MMO was measured with the head of the subjects in an upright position and rested against a firm wall/surface, so as to eliminate the possible influence of different head positions on values of MMO.
Also, Wood and Branco [1] concluded that using a ruler or Vernier caliper for determination of mouth opening gives more precise and accurate results.
It has been seen in several studies that MMO steadily increases after birth until adolescence [5,15,18,23] and then gradually decreases as age progresses [16,19]. The present study reported a gradual increase in MMO with advancing age. These findings were in accordance with results obtained from studies done by Hirsch et al., Cortese et al., and Vanderas, who found MMO to be directly correlated with age [24–26].
Gender differences in MMO were also observed in a few studies [24,27]. In the present study, a statistically significant difference was observed between boys and girls in all the three age groups. The results of our study were in accordance with the results of the study conducted by Pullinger et al., who observed that the maximum passive jaw opening was 2.7% wider in males compared to females [28]. Contrary to this, Abou–Atme et al., in his study reported no gender difference in the measurement of MMO in children between the age of four to fifteen years [29].
The present study revealed an indefinitive correlation of MMO with height and weight. Similar results were obtained by a study conducted by Agerberg who found a weak correlation of MMO with height and weight [19]. On the contrary, Rothenberg [27] observed a positive correlation between MMO values in relation to weight and height in subjects in age group four and fourteen years.
One characteristic finding which was evident in this present study was the higher MMO values in long faced or leptoproscopic individuals among all age groups. This particular feature deduced from this study adds to the novelty of the study. Greater downward and backward growth of mandible can be a significant factor to contribute to the greater MMO values in such facial pattern.
The increased values of MMO with age and leptoproscopic face type could be due to changes in the temporomandibular joint apparatus, facial morphology, muscle development, and growth of cranial base and mandible, particularly in length.
At present, however, it is difficult to propose the exact mechanism responsible for this increase in MMO. This study, in combination with several clinical expertises can serve as an available approach for clinical decision making in diagnosing divergence and diseases related to the function of the masticatory system by knowing the normal range of MMO in individuals of a particular age group.
Clinical Implication of Present Study: After having known the average range of normal maximal mouth opening, it can help the clinician to know if there is any limitation in mouth opening of any individual and can also help in evaluating the improvement during/after treatment. As stated earlier, MMO can also be helpful in providing necessary information for designing of dental instruments/prosthesis.
Limitation
Horizontal movement of mandible wasn’t taken into consideration.
Sample size was small.
Conclusion
There was a significant difference in MMO between males and females; with males having the higher values in all age groups. MMO was seen to increase with age in a statistically significant manner. Significantly increased value of MMO was observed in leptoprosopic facial type in comparison to euryproscopic and mesoprosopic facial type in each age group.
**. Correlation is significant at the 0.01 level (2-tailed).