Gas Bubbles in the Bone: A Case Report
Bita Abbasi1, Farrokh Seilanian-Toosi2, Sirous Nekooei3, Behrang Rezvani Kakhki4, Reza Akhavan5
1 Assistant Professor, Department of Radiology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
2 Associate Professor, Department of Radiology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3 Associate Professor, Department of Radiology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
4 Assistant Professor, Department of Emergency Medicine, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
5 Assistant Professor, Department of Emergency Medicine, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Reza Akhavan, MD. Edalatian Emergency Department, Imam Reza Hospital, Razi sq. Mashhad, Iran.
E-mail: akhavanr@mums.ac.ir
Intraosseous pneumatocysts are benign gas-filled cavities within bones which are most commonly found in ilium, sacrum and vertebrae. The lesions are asymptomatic and found incidentally while evaluating for other injuries. Here, we present an intraosseous pneumatocyst of ilium in a 23-year-old male patient. Although once thought to be rare, intraossseous pneumatocyst are now believed to be more common. Thus, familiarity with their appearance is essential to avoid unnecessary workup. Intraosseous pneumatocysts are differentiated from more clinically significant differential diagnoses like osteonecrosis and osteomyelitis by their characteristic appearance of intraosseous air collections with sclerotic rim.
Ilium, Intraosseous, Pneumatocyst, Tomography
Case Report
A 23-year-old male was brought in the emergency department by Emergency Medical Service (EMS) after a motor vehicle collision. He was lying on a backboard but alert and responsive. His vitals on arrival were respiratory rate of 18 breaths per minute, pulse rate of 88 beats per minute, temperature of 37.3°C, blood pressure of 122/85 mmHg and O2 saturation of 95% in room air. We detected no superficial abrasions or bruise. He complained of posterior pelvic pain and had mild localized swelling and tenderness over the symphysis pubis on physical examination. He had normal range of motion of the both hips, without any limb shortening or rotational deformity. Other physical examination findings were unremarkable. A pelvic plain radiograph was obtained and no obvious pathology was detected [Table/Fig-1]. A pelvic Computed Tomography (CT) scan was performed to evaluate for posterior arc injuries. The CT scan revealed no fracture line or pelvic hematoma. Incidentally, a well-defined 207mm lobulated lesion was detected within the right ilium adjacent to the sacroiliac joint. The lesion contained gas densities with a mean Hounsfield number of -666 and had a thin sclerotic rim [Table/Fig-2]. There was no surrounding soft tissue swelling. The lesion was not visible on plain radiograph. The patient had no pain on the right side of pelvis and did not mention any previous history of pain or trauma except that recent one. He was followed on the outpatient service and the pain disappeared after a week. He had no complaints after 3 months of follow-up.
Anteroposterior pelvic radiograph depicts no abnormality.

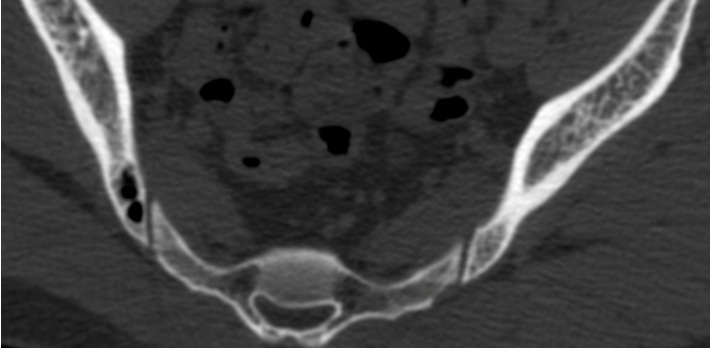
Axial pelvic CT scan in bone window shows a well-defined lobulated gas collection with a thin sclerotic rim within the right ilium. The lesion is located adjacent to the sacroiliac joint. There is no cortical breakthrough or connection to the joint space.
Discussion
Intraosseous pneumatocyst is an uncommon condition of gas accumulation within a bone that was first described in 1984 by Ramirez et al., [1]. True pneumatization is not expected in any human bone except paranasal sinuses and middle ear, and other gas collections within bone are either a variant of normal or pathologic finding [2]. The most common involved bones are ilium and sacrum near the sacroiliac joint. The lesion is benign and usually discovered while evaluating for other injuries. Although more frequent that was initially thought, the lesion is still unknown to most physicians and might cause clinical confusions [3]. The clinicians should be familiar with this condition in order not to confuse it with other considerable differential diagnoses such as osteonecrosis, osteomyelitis or post-embolization state [4].
The pathogenesis of the lesion is poorly understood [5]. They are believed to be acquired and the nature of the accumulated gas is nitrogen [2]. Some lesions are near degenerative joints and are thought to be produced by a mechanism similar to vacuum phenomenon [6,7]. In other cases, like our patient, the lesions are seen in young people and not near a degenerative joint. These are believed to be primary lesions with unknown pathogenesis [5].
Pneumatocysts are believed to be perceptible on plain radiographs as lucent areas. In our patient there was mild prominency of bowel loops and fecal materials that were proposed to mask the lesion. Intraosseous pneumatocysts are usually single and 2-5 mm [2], while in our case the lesion was solitary but large and lobulated. Their incidence is now believed to be more than estimated, and because of being asymptomatic, they usually remain undetected [2].
It is important to appreciate the benign nature of the process, as intraosseous air might be seen in some severe conditions like osteonecrosis, osteomyelitis, post-embolization, post-operative or post-traumatic states [2,8]. CT scan is the modality of choice and the presence of gas collection within ilium or sacrum near the sacroiliac joint, with no associated soft tissue reaction suffice for diagnosis. However, air collection in uncommon regions like vertebral bodies may warrant further evaluation [2].
The lesion has no clinical significance, but familiarity with the appearance is important for clinicians to prevent unnecessary workup. No further workup, biopsy or surgical resection is required for the lesion.
Conclusion
Intraosseous pneumatocysts are rare gas collections within the bone that most commonly appear in ilium and sacrum near the sacroiliac joint. Although these lesions have no clinical significance, they have important differential diagnoses that should be excluded.
[1]. Ramirez H, Blatt ES, Cable HF, McComb BL, Zornoza J, Hibri NS, Intraosseous pneumatocysts of the ilium. Findings on radiographs and CT scansRadiology 1984 150(2):503-05. [Google Scholar]
[2]. Al-Tarawneh E, Al-Qudah M, Hadidi F, Jubouri S, Hadidy A, Incidental intraosseous pneumatocyst with gas-density-fluid level in an adolescent: a case report and review of the literatureJournal of Radiology Case Reports 2014 8(3):16-22. [Google Scholar]
[3]. Oehler E, Valour F, Pascart T, Intraosseous pneumatocysts: a case based reviewClinical Rheumatology 2013 32(1):129-34. [Google Scholar]
[4]. Haithcock JA, Layton KF, Opatowsky MJ, Vertebral pneumatocysts: uncommon lesions with pathognomonic imaging characteristicsProceedings 2006 19(4):423-24. [Google Scholar]
[5]. Kamba M, Ohuchi Y, Ogawa T, Ohata R, Intraosseous pneumatocyst of the scapulaThe British Journal of Radiology 2000 73(870):658-60. [Google Scholar]
[6]. Nakayama T, Ehara S, Hama H, Spontaneous progression of vertebral intraosseous pneumatocysts to fluid-filled cystsSkeletal Radiology 2001 30(9):523-26. [Google Scholar]
[7]. Steingruber IE, Bach CM, Wimmer C, Nogler M, Buchberger W, Multisegmental pneumatocysts of the lumbar spine mimic osteolytic lesionsEuropean radiology 2001 11(5):845-48. [Google Scholar]
[8]. Cosar M, Eser O, Aslan A, Korkmaz S, Boyaci G, Degirmenci B, Vertebral body pneumatocyst in the cervical spine and review of the literatureTurkish Neurosurgery 2008 18(2):197-99. [Google Scholar]