Morphometric Study on Bicipital Groove among South Indian Population
Yamini Soundara Rajan1, Senthil Kumar Sampath Kumar2
1 Post Graduate, Department of Anatomy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, India.
2 Professor, Department of Anatomy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Senthil Kumar Sampath Kumar, Professor, Department of Anatomy, Sri Ramachandra Medical College and Research Institute, Porur-600116, Chennai, India.
E-mail: ssksrmc@gmail.com
Introduction
The Bicipital Groove (BG) is an indentation between the lesser and greater tubercles of the proximal part of the humerus. It conveys biceps tendon, its synovial sheath and ascending branch of anterior circumflex humeral artery. The knowledge of the morphometry is important for the understanding of the functional aspect of the shoulder region.
Aim
To study the morphometry of bicipital groove of humerus in south Indian population.
Materials and Methods
In the present study, 100 adult humeri (50 right and 50 left) were examined. The length of the medial wall, lateral wall, width and depth were measured by using vernier calliper. The humeri were examined for the presence of supratubercular ridge. All the parameters were accurately measured and the data were analysed.
Results
The mean length of BG on right side was 84.79±5.84 mm and 87.33±6.40mm on the left side. The mean width of BG on right side was 6.84±1.01mm and 7.74±1.96mm on the left side. The mean depth of BG on right side was 4.21±0.58 mm and 5.01±1.05mm on the left side. The mean length of the medial and lateral walls on the right side was 24.22±1.02mm and 32.05±2.21mm respectively and that on the left side was 23.31±2.21mm and 31.12±0.24mm respectively. 17% of humeri on the right side and 14% on the left side showed the presence of supratubercular ridge of Meyer in the present study.
Conclusion
Bicipital groove is present in the shoulder region where wide range of movements occurs. Osseous spurs and supratubercular ridge may predispose dislocation of tendon of biceps brachii. Hence morphometric knowledge is obligatory and is significant functionally and clinically for better understanding of this region.
Biceps tendonitis, Osseous spurs, Supratubercular ridge of Meyer
Introduction
The Bicipital Groove (BG) in the proximal part of humerus is an indentation formed between the lesser and greater tubercles. The lateral edge of lesser tubercle forms the medial border of BG. The proximal third of the anterior border of the greater tubercle forms the lateral lip of BG [1]. The BG or intertubercular sulcus lodges the long head of biceps, its synovial sheath and the ascending branch of anterior circumflex humeral artery. The BG is converted into a canal by the fibrous band called transverse humeral ligament which extends from the lesser tubercle to the greater tubercle of the humerus. The transverse humeral ligament provides stability and effective functioning of long head of biceps muscle and prevents subluxation of the tendon during multi-directional biomechanical movements of the arm [2]. Coracohumeral ligament overlies the transverse humeral ligament and continues with rotator cuff [3]. The supratubercular ridge is a bony prominence that is continuous with the lesser tubercle. It was originally described by Meyer in 1928 [4] and later by Hitchcock and Bechtol [5] and it allows gradual change in the direction of tendon of long head of biceps by elevating and forcing it laterally. Owing to the functional significance of structures related to BG, it is an important landmark for replacement of prosthesis of shoulder and the knowledge of its morphometry is essential for the selection of prosthetic design, size and position [6]. Apart from this, morphometry of bicipital groove may influence the function of surrounding structures leading to various pathologic conditions [7,8]. In the present study, the morphometry of BG was examined in relation to its length, width, depth, length of the medial and lateral walls of the BG and the presence of supratubercular ridge of Meyer in south Indian population.
Materials and Methods
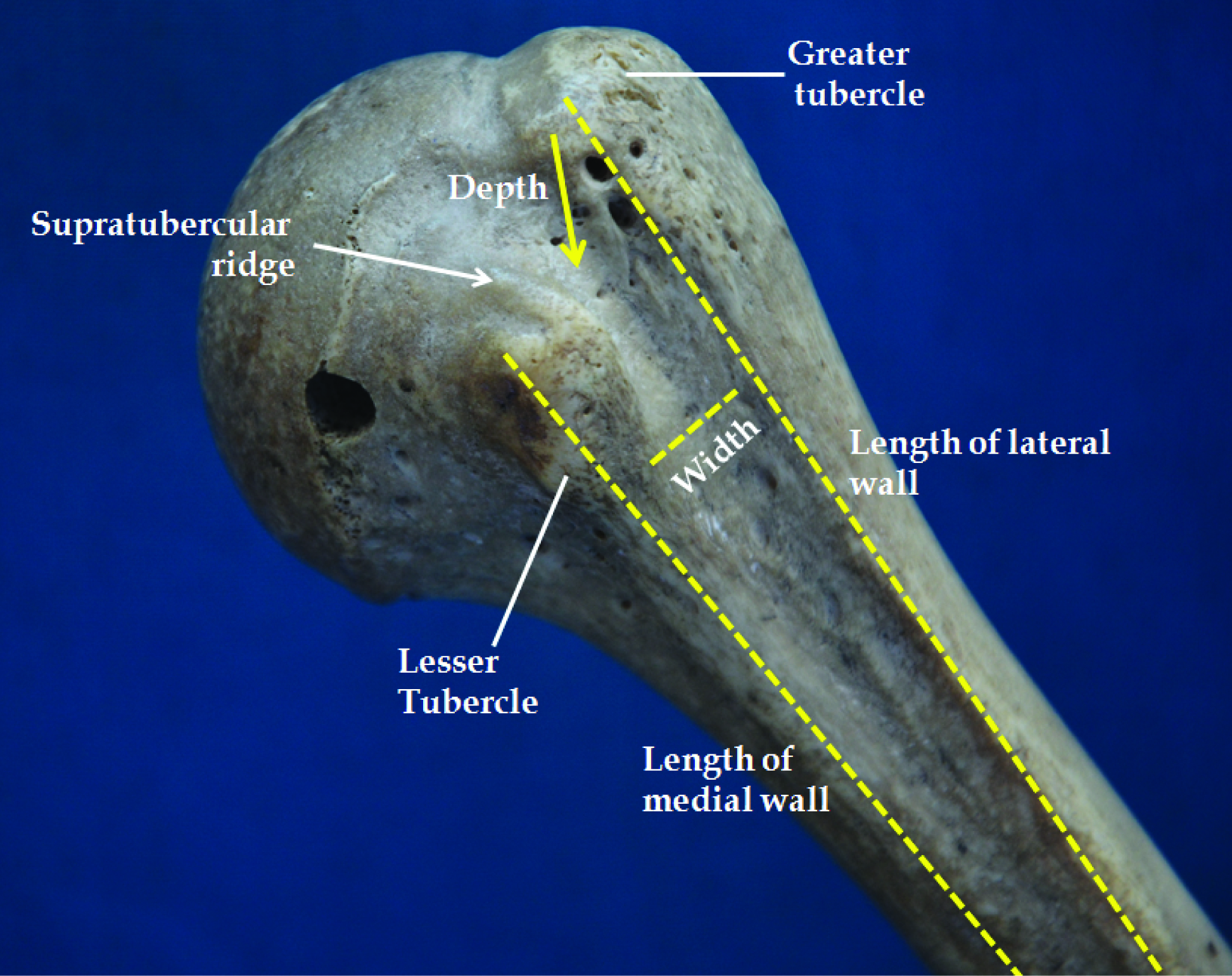
The study was carried out in 100 adult humeri (50 right and 50 left) from the Department of Anatomy, Sri Ramachandra Medical College and Research Institute, Sri Ramachandra University, Chennai between July 2014 and September 2015. Bones with external deformities were excluded from the study. The length, width, depth were accurately measured by using vernier calliper. All the parameters were measured by single observer twice to ensure accuracy and the average was taken. The parameters were tabulated and statistically analysed. The length of the BG was measured from the point between the tubercles to the end of the medial lip of the BG. The depth of the BG was measured between the greater and lesser tubercles. The width of the BG was measured between the midpoint of the medial and lateral lips. The length of the medial and lateral walls was measured from the tubercles to the respective lips of the BG. Supratubercular ridge is a bony prominence extending from the lesser tubercle [9] and is found in few humeri in the present study [Table/Fig-1]. Data were presented in Mean±SD. Statistical significance is performed using independent t-test. Data were analysed using SPSS 15.0 Programme (SPSS Inc, Chicago, Illinos, USA).
Measurements of the bicipital groove.
Results
The mean length, width, depth of the BG and the mean length of the medial and lateral walls of BG are given in [Table/Fig-2]. The mean length of BG on right side was 84.79±5.84mm and 87.33±6.40mm on the left side. The mean width of BG on right side was 6.84±1.01mm and 7.74±1.96 mm on the left side. The mean depth of BG on right side was 4.21±0.58mm and 5.01±1.05mm. The mean length of the medial and lateral walls on the right side was 24.22±1.02mm and 32.05±2.21mm respectively and that on the left side was 23.31±2.21mm and 31.12±0.24mm respectively. 17% humeri on the right side and 14% on the left side showed the presence of supratubercular ridge of Meyer in the present study.
Measurements of the bicipital groove.
| Bicipital groove | Right side | Left side |
|---|
| Length of BG | 84.79±5.84 mm | 87.33±6.40 |
| Width of BG | 6.84±1.01mm* | 7.74±1.96 mm* |
| Depth of BG | 4.21±0.58 mm* | 5.01±1.05 mm* |
| Length of the medial wall | 24.22±1.02 mm | 23.31±2.21mm |
| Length of the lateral wall | 32.05±2.21mm | 31.12±0.24mm* |
* Statistical significance p<0.05
Discussion
The BG in the humerus lodges the tendon of biceps brachi in a tunnel formed by the fibrous band i.e., transverse humeral ligament. The humerus moves with the tendon of biceps in all movements of the shoulder. Rajani S et al., conclusively reported the length of the medial and lateral walls of the BG [2]. In their study, the length of the medial wall was 23±4mm on the right side and 24±5mm on the left side and the length of the lateral wall was 31±6mm on the right side and 31±5 mm on the left side which is similar to the present study [Table/Fig-3].
Comparison of length, width and depth of bicipital groove with other authors [2,9–12].
| Parameter | Wafae etal., [9](mm) | Cone et al.,[10](m) | Abboudet al., [11](mm) | Murlimanju et al., [12] (mm) | Rajani S et al., [2] (mm) | Present study (mm) |
|---|
| Right | Left | Right | Left | Right | Left |
|---|
| Length | 81 | - | | 86±10.1 | 83.3±11.5 | 85±09 | 83±10.1 | 84.79±5.84 | 87.33±6.40 |
| Width | 10.1 | 8.8 | - | 8.3±2.4 | 8.7±2.2 | 9.0±2.1 | 8.9±1.1 | 6.84±1.01 | 7.74±1.96 |
| Depth | 4 | 4.3 | 5.1 | 4.7±2.0 | 4.2±1.6 | 5.0±1.0 | 6.0±1.0 | 4.21±0.58 | 4.21±0.58 |
No other authors have reported the lengths of medial and lateral wall and so comparison could not be made with different population. Rockwood and Masten mentioned that humans are unique among primates in presenting marked variations in the configuration of the BG [13]. The depth and width of the BG are very important in the retention of tendon of biceps. Several authors reported greater incidence of subluxation and dislocation of tendon of biceps when the BG is shallow [3–5,14,15]. The instability of biceps tendon may be attributed to the lengths of medial and lateral walls, medial wall angles depending on width and depth constituting shallowness of BG, presence of supratubercular ridge [16–18]. The length, width and depth of BG of different authors are given in [Table/Fig-3].
The morphometry of BG is likely to be influenced by the nature of manual work a person does. In manual workers the pressure on the biceps tendon will be higher on the right side than left side and vettivel et al., reported such morphometric change in the BG [7]. Murlimanju et al., in the Indian population reported the mean length of the BG on the right and left side which is 86±10.1mm and 83.3±11.5mm respectively [12]. The mean width was 8.3±2.4mm on the right side and 8.7±2.2mm on the left side. The width was found to be lower in the present study than the studies done by other authors. The other parameters are similar to Rajani S and Murlimanju et al., [2,12]. Wafae et al., reported mean width of 10mm which is higher than the other study population [9]. Most of the parameters are found to be similar among different study population and so role of ethnic variation is not reported. Pfahler et al., and Robertson et al., reported sex differences in the morphometry of BG [19,20].
Hitchcock and Bechtol demonstrated definite correlation between the supratubercular ridge and tendonitis [5]. Cone et al., defined the supratubercular ridge as a bony ridge extending proximally from the lesser tubercle more than one-half of the distance to the humeral head [10]. In their study supratubercular ridge was present in 48% of all specimens and 46% of all patients. But the authors through radiographic interpretations in specimens and patients concluded that the supratubercular ridges are not pathologically significant. This is in contravention to the findings of Hitchcock and Bechtol. However cone et al., agreed that bicipital tendonitis does not have radiological manifestations, so the theory of Hitchcock and bechtol cannot be completely discounted. Sangeeta gupta et al., observed 42% incidence of supratubercular ridge in North Indian population but their findings were not statistically significant [21]. Vettivel et al., found this ridge in 88% on the right side and 57% on the left side [7]. The authors in a functional perspective described the higher incidence of supratubercular ridge on the right side will prevent medial displacement of biceps tendon. Murlimanju et al., reported supratubercular ridge in 24 (23.1%) of the humeri of which 16 (15.4%) were on the right side. In the present study we found a lower incidence of 17% supratubercular ridge on the right side and 15% on the left side. This may probably be due to ethnic variation and it needs to be substantiated with comparison with different population.
Limitation
Though the present study focussed the morphometry of BG, the variation with respect to gender is not examined. Owing to the functional differences of shoulder joint between sexes, gender differences may exist and need to be elucidated.
Conclusion
In the present study, the width of the BG is reduced and the incidence of supratubercular ridge is less when compared to other studies. The findings would pave way for better understanding of the structural and functional aspects of the BG. The data of the present study would also add knowledge to the existing literature.
* Statistical significance p<0.05
[1]. Susan standring, Grays Anatomy: the anatomical basis of clinical practice 2008 40th editionEdinburghElsevier Churchil Livingstone:796-798. [Google Scholar]
[2]. Rajani S, Man S, Review of bicipital groove morphology and its analysis in North Indian PopulationISRN Anatomy 2013 :1-7. [Google Scholar]
[3]. Slatis P, Aalto K, Medial dislocation of the tendon of the long head of the biceps brachiiActa Orthopaedica Scandinavica 1979 50(1):73-77. [Google Scholar]
[4]. Meyer AW, Spontaneous dislocation and destruction of the tendon of the long head of biceps brachii: 59 instancesArch Surg 1928 17:493-506. [Google Scholar]
[5]. Hitchcock HH, Bechtol CO, Painful shoulderJ Bone Joint Surg (Am) 1948 30:262-73. [Google Scholar]
[6]. Robertson DD, Yuan J, Bigliani LU, Flatow EL, Yamaguchi K, Three-dimensional analysis of the proximal part of the humerus: Relevance to arthroplastyJournal of Bone and Joint Surgery 2000 82(11):1594-602. [Google Scholar]
[7]. Vettivel S, Indrasingh I, Chandi G, Chandi SM, Variations in the intertubercular sulcus of the humerus related to handednessJournal of Anatomy 1992 180(2):321-26. [Google Scholar]
[8]. Rasch PJ, Burke RK, Kinesiology and Applied Anatomy 1974 5th editionPhiladelphia USALea & Febiger [Google Scholar]
[9]. Wafae N, Atencio Santamaría LE, Vitor L, Pereira LA, Ruiz CR, Wafae GC, Morphometry of the human bicipital groove (sulcus intertubercularis)Journal of Shoulder and Elbow Surgery 2010 19(1):65-68. [Google Scholar]
[10]. Cone RO, Danzig L, Resnick D, Goldman AB, The bicipital groove: radiographic, anatomic and pathologic studyAJR Am J Roentgenol 1983 141:781-88. [Google Scholar]
[11]. Abboud JA, Bartolozzi AR, Widmer BJ, DeMola PM, Bicipital groove morphology on MRI has no correlation to intra-articular biceps tendon pathologyJournal of Shoulder and Elbow Surgery 2010 19(6):790-94. [Google Scholar]
[12]. Murlimanju BV, Prabhu L.V, Pai MM, Anthropometric study of the bicipital groove in indians and its clinical implicationsChang Gung Medical Journal 2012 35(2):155-59. [Google Scholar]
[13]. Rockwood CA, Masten FA, The Shoulder. Vol 2 1992 PhiladelphiaW. B. Saunders Company [Google Scholar]
[14]. Nevaiser RJ, Nevaiser TJ, Lesions of musculutendinous cuff of the shoulder—diagonosis and management in American Academy of Orthopaedic SurgeonsInstructional Course Lectures 1981 30St. Louis, Mo, USA:238-57. [Google Scholar]
[15]. Neviaser TJ, Neviaser RJ, Neviaser JS, The fourin-one arthroplasty for the painful arc syndromeClinical Orthopaedics and Related Research 1982 163:107-12. [Google Scholar]
[16]. Smith A.L. Morphologic classification of the bicipital groove in Proceedings of the annual meeting of the American Academy of Orthopaedic Surgeons (AAOS ’07), SanDiego, Calif, USA, 2007 [Google Scholar]
[17]. Toshiaki A, Itoi E, Minagawa H, Cross-sectional area of the tendon and the muscle of the biceps brachii in shoulders with rotator cuff tears: a study of 14 cadaveric shouldersActa Orthopaedica 2005 76(4):509-12. [Google Scholar]
[18]. Refior HJ, Sowa D, Long tendon of the biceps brachii: sites of predilection for degenerative lesionsJournal of Shoulder and Elbow Surgery 1995 4(6):436-40. [Google Scholar]
[19]. Pfahler M, Branner S, Refior HJ, The role of the bicipital groove in tendinopathy of the long biceps tendonJ Shoulder Elbow Surg 1999 8:419-24. [Google Scholar]
[20]. Robertson DD, Yuan J, Bigliani LU, Flatow EL, Yamaguchi K, Three-dimensional analysis of the proximal part of the humerusJ Bone Joint Surg Am 2000 82:1594-602. [Google Scholar]
[21]. Gupta S, Naqshi BF, Shah AB, Variations in the bicipital groove in north Indian population: a morphological and morphometric study and review of literatureInt J Health Sci Res 2015 5(9):220-26. [Google Scholar]