Irreversible pulpitis is the most common reason for endodontic treatment in primary and permanent teeth. Root canal therapy and extraction are the two viable and most documented treatment options for the same. Studies with regards to management of mature permanent teeth with carious exposure and treatment with vital pulp therapies such as adult permanent tooth pulpotomy are scarce. However, permanent tooth pulpotomy with the new calcium-silicate based cements (Mineral Trioxide Aggregate and Biodentine) can help preserve the tooth pulp vitality and promote healing and repair foregoing the more invasive root canal therapy procedure. A 12-year old male patient with irreversible pulpitis in right mandibular first permanent molar was treated with complete coronal pulpotomy with placement of Biodentine in the pulp chamber and a full coronal coverage using stainless steel crown. Clinical and radiographic examinations were performed at three, six, twelve and eighteen months. At the end of 18 months, the patient was completely asymptomatic and the tooth was free of any clinical and radiographic signs of inflammation and infection.
Calcium enriched mixture, Irreversible pulpitis, Root canal therapy, Stainless steel crown
Case Report
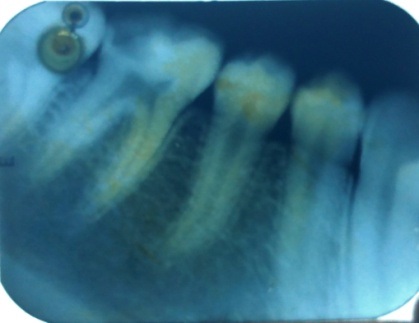
A 12-year old male patient reported with chief complaint of pain in right back tooth region since 4-5 days. On clinical examination, there was presence of a large deep carious lesion involving the right mandibular first permanent molar. The patient had a history of mild to moderate pain on intake of hot and cold fluids since 4-5 days with no history of any previous pain. There was no history of swelling or medications. There was no tenderness on percussion and no associated sinus opening adjacent to the involved teeth. Diagnostic tests revealed lingering pain to hot and cold tests. Electric pulp testing (EPT) results showed a more intense response in the involved tooth as compared to the contralateral healthy mature permanent tooth. Radiographic examination revealed presence of a large radiolucency in the coronal portion of the involved tooth approaching the pulp with normal periodontal ligament space and lamina dura [Table/Fig-1]. There was no periapical lesion visible on the radiograph. After complete clinical and radiographic examination, a diagnosis of irreversible pulpitis was made in the involved tooth. The patient was treated with complete coronal pulpotomy with placement of Biodentine in the pulp chamber and full coronal coverage with stainless steel crown was performed.
Pre-operative radiograph of 46 showing a deep carious lesion.
The tooth was anaesthetized with 2% lidocaine with 1: 2,00,000 adrenaline. Access cavity was prepared using high speed handpiece with water coolant. The coronal pulpal tissue was then removed with the help of sharp spoon excavator (PREMIER USA 1003446). The pulp chamber was irrigated with sterile normal saline solution to remove any pulpal tags and bleeding from the root canals was arrested with the help of gentle application of cotton soaked in sterile normal saline solution for 5 minutes. A 2mm layer of freshly mixed Biodentine was packed in the pulp chamber with the help of plastic instruments and a permanent restoration was given.
The patient was recalled after one day for evaluation of post-operative pain and swelling. After seven days, a full coronal restoration was placed on the tooth. Regular follow ups were carried out after three, six, twelve and eighteen months to examine any pain or tenderness to percussion, and radiographic examination was done to check for any periapical changes as periodontal ligament space widening or internal or external resorption [Table/Fig-2].
Immediate post-operative radiograph after Biodentine pulpotomy. Follow up radiographs after 6 and 18 months.

At six, twelve and eighteen months, follow-up of the tooth showed absence of any periapical pathology with normal periodontal ligament space. The tooth was fully functional and the patient was asymptomatic.
Discussion
The treatment of teeth with irreversible pulpitis is generally done with root canal therapy that can be considered as a prophylactic procedure, since the radicular pulp is often free of infection and the philosophy is to avoid further infection of the root canal system [1]. Even with the advanced techniques and materials, root canal procedures still continue to be a challenge the clinician due to the intricacies in the root canal system and the associated treatment procedures [2]. Root canal therapy also makes the tooth non-vital with removal of a substantial amount of tooth structure leading to frequent fractures of such teeth and subsequent loss of teeth. Therefore, pulpotomy which is a vital pulp therapy procedure in which the coronal portion of the pulp is removed and the radicular pulp is preserved with the aim of maintaining the pulp vitality can be performed in such teeth with no periapical lesions. On the remaining radicular pulp, a suitable biocompatible material is packed to protect the pulp from further insult and initiate healing and repair [3].
Pulpotomy can be carried out with various materials based on their biocompatibility, sealing ability and antimicrobial efficacy on coming in contact with the dental pulp. Latest bioactive materials such as Mineral Trioxide Aggregate (MTA) and Biodentine, Calcium-Enriched Mixture (CEM) have excellent biocompatibility and sealing abilities with the added advantage of inducing proliferation of the pulpal cells. MTA was introduced in 1993 as a root-end filling material in surgical endodontic treatment [4]. In various studies, limitations of MTA as difficulty in manipulation, increased cost, two visit treatment and longer setting time have been noticed. In comparison to MTA, Biodentine provides better sealing ability with a reduced setting time [5]. Biodentine causes increased calcium and TGF- ß1 secretion from pulp cells which induces angiogenesis, cell differentiation and mineralization [6,7]. The mechanism of action of Biodentine is its ability to induce odontoblast differentiation and enhanced proliferation, migration and adhesion of human pulp stem cells, when placed in direct contact with the dental pulp [8]. Another major advantage of Biodentine over MTA is its reduced cost.
Calcium enriched mixture has similar properties to Biodentine. The important constituents of CEM are alkaline earth metal oxides and hydroxides (for example, calcium oxide and calcium hydroxide, calcium phosphate and calcium silicate) [9]. CEM cement and Biodentine display combined properties of biocompatibility of MTA with more efficient characteristics, such as a significantly shorter setting time, good handling characteristics, and no tooth staining. However, the setting time for CEM is nearly 50 minutes as compared to Biodentine, which has a setting time of 12 minutes. Therefore, Biodentine was chosen as the material of choice for pulpotomy of carious teeth in our patient.
Nowicka et al., studied the response of Biodentine on direct pulp-capping in 28 maxillary and mandibular permanent human molars that were extracted for orthodontic treatment purposes. The histology of teeth showed a complete dentinal bridge formation with well-arranged layers of odontoblasts that formed tubular dentine under the osteodentine. There was no inflammatory pulp response [10].
The patient showed no post-operative pain and discomfort in the follow-up showing complete success in the treatment after 18 months. Study by Matsuo et al., found similar success rate at the end of three months and 18 months follow-up and they concluded that three months was an adequate time to evaluate the success or failure of such treatment [11].
In a review by Aguilar and Linsuwanont, the success rate for partial pulpotomy was 99.4% and for full pulpotomy was 99.3% in vital permanent teeth with closed apices [12]. In another study, Asgary and Ehsani performed pulpotomy with new endodontic cement on 12 permanent molars with established irreversible pulpitis. They demonstrated 100% success in all the teeth with the presence of a hard dentinal tissue bridge and normal pulp [13]. Simon et al., performed pulpotomy on permanent molar teeth using proRoot MTA and showed 82% success at the end of 24 months [14].
Asgary and Ehsani compared the treatment outcomes of Pulpotomy with a Calcium-Enriched Material (PCEM) and conventional RCT procedure in mature molars with irreversible pulpitis. They concluded that PCEM significantly reduced post-operative pain and showed a higher radiographic success rate than conventional RCT [15]. McDoughal et al., [16] performed eugenol pulpotomy in 73 patients with irreversible pulpitis and Nosrat and Nosrat [17] performed calcium hydroxide pulpotomy on two adult teeth with carious exposures and demonstrated healthy dentinal pulps after treatment with pulpotomy. Thereby, suggesting pulpotomy as an alternative therapy for mature teeth with irreversible pulpitis.
The healing of the dental pulp may be associated to the placement of an immediate full coronal restoration on the tooth after seven days, thereby reducing the chances of microleakage and bacterial invasion. Most of the failures in vital pulp therapy and endodontic treatment are attributed to micro-leakage at the coronal tooth-restoration interface. Massler demonstrated the most important cause of failure in vital pulp therapy as the presence of leakage in the healing process [18].
The selection of patients is an important criterion for consideration of pulpotomy procedures in permanent teeth with closed apices. The pre-operative pain in the patient was mild to moderate in nature and he reported to the dentist in the first 4-5 days of its initiation. When mild to moderate pain is present with no previous history of pain in the tooth under evaluation, the histologic picture usually manifests as mild inflammation or chronic partial pulpitis without histologic areas of necrosis [19].
The age of the patient was 12 years. Increasing age of a patient may negatively affect clinical success. Studies have shown that in older patients, typically more fibrous dental pulp has a reduced ability to overcome insult due to less cellularity with limited blood supply affecting the treatment outcomes in such cases [20,21].
The bleeding from the radicular pulp could be controlled by pressure from cotton pellets dipped in sterile normal saline for 5 minutes showing that the radicular pulp was vital and non-infected. A sluggish bleeding present even after application of pressure suggests an infected radicular pulp with need of root canal treatment.
Conclusion
In accordance to the favorable results of our cases, a reasonable argument supporting mature tooth pulpotomy in cases of irreversible pulpitis can be stated. Biomaterials such as Biodentine with pulp healing properties may challenge the complete philosophy of our conventional endodontic treatment. Case selection including age, status of pulp and control of bleeding; however, remains an important criterion for the same.
[1]. Spanberg LS, Endodontic treatment of teeth with apical periodontitis. In: Orstavik D, Pittford T, editorsEssential Endodontology 1998 OxfordBlackwell Science Ltd:211-14. [Google Scholar]
[2]. Solomon RV, Faizuddin U, Karunakar P, Sarvani GD, Soumya SS, Coronal pulpotomy technique analysis as an alternative to pulpectomy for preserving the tooth vitality, in the context of tissue regeneration: a correlated clinical study across 4 adult permanent molarsCase Reports in Dentistry 2015 (2015):1-12. [Google Scholar]
[3]. Eghbal MJ, Asgary S, Ali Baglue R, Parirokh M, Ghoddusi J, MTA pulpotomy of human permanent molars with irreversible pulpitisAust Endod J 2009 35:4-8. [Google Scholar]
[4]. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR, Physical and chemical properties of a new root-end filling materialJ Endod 1995 21:349-53. [Google Scholar]
[5]. Singh H, Kaur M, Markan S, Kapoor P, Biodentine: A promising dentin substituteJ Interdiscipl Med Dent Sci 2014 2:140 [Google Scholar]
[6]. Han L, Okiji T, Bioactivity evaluation of three calcium silicate-based endodontic materialsInt Endodon J 2013 46(3):808-14. [Google Scholar]
[7]. Laurent P, Camps J, About I, Biodentine TM induces TGF- ß1 release from human pulp cells and early dental pulp mineralizationInt Endodon J 2012 45(5):439-48. [Google Scholar]
[8]. Zanini M, Sautier JM, Berdal A, Simon S, Biodentine induces immortalised murine pulp cell differentiation into odontoblast-like cells and stimulates biomineralisationJ Endodon 2012 38(9):1220-26. [Google Scholar]
[9]. Asgary S, Kamrani FA, Antibacterial effects of five different root canal sealing materialsJ Oral Sci 2008 50:469-474. [Google Scholar]
[10]. Nowicka A, Lipski M, Parafiniuk M, Sporniak-Tutak K, Lichota D, Kosierkiewicz A, Response of human dental pulp capped with biodentine and mineral trioxide aggregateJ Endodon 2013 39:743-47. [Google Scholar]
[11]. Matsuo T, Nakanishi T, Shimizu H, Ebisu S, A clinical study of direct pulp capping applied in carious-exposed pulpsJ Endodon 1996 22:551-56. [Google Scholar]
[12]. Aguilar P, Linsuwanont P, Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic reviewJ Endodon 2011 27(5):581-87. [Google Scholar]
[13]. Asgary S, Ehsani S, Permanent molar pulpotomy with a new endodontic cement: A case seriesJ Conserv Dent 2009 12:31-36. [Google Scholar]
[14]. Simon S, Perard M, Zanini M, Smith AJ, Charpentier E, Djole SX, Should pulp chamber pulpotomy be seen as a permanent treatment? Some preliminary thoughtsInt Endodon J 2013 46:79-87. [Google Scholar]
[15]. Asgary S, Eghbal MJ, A clinical trial of pulpotomy vs. root canal therapy of mature molarsJ Dent Res 2010 89(10):1080-85. [Google Scholar]
[16]. McDougal RA, Delano OE, Caplan D, Sigurdsson A, Trope M, Success of an alternative for interim management of irreversible pulpitisJ Am Dent Assoc 2004 135:1707-12. [Google Scholar]
[17]. Nosrat IV, Nosrat CA, Reparative hard tissue formation following calcium hydroxide application after partial pulpotomy in cariously exposed pulps of permanent teethInt Endod J 1998 31:221-26. [Google Scholar]
[18]. Massler M, Preserving the exposed pulpJ Pedodont 1978 2:217-27. [Google Scholar]
[19]. Bender IB, Pulpal pain diagnosis-a reviewJ Endodon 2000 26(3):175-79. [Google Scholar]
[20]. Abarajithan M, Velmurugan N, Kandaswamy D, Management of recently traumatized maxillary central incisors by partial pulpotomy using MTA: case reports with two-year follow-upJ Conserv Dent 2010 13(2):110-13. [Google Scholar]
[21]. Hørsted P, Søndergaard B, Thylstrup A, El Attar K, Fejerskov O, A retrospective study of direct pulp capping with calcium hydroxide compoundsEndod Dent Traumatol 1985 1:29-34. [Google Scholar]