Acquired Solitary Glomangiomyoma on the Forearm: A Rare Case Report
Ayse Nur Deger1, Hakki Deger2, Mahir Tayfur3, Mecdi Gurhan Balcioglu4, Emine Kadioglu5
1 Assistant Professor, Department of Pathology, Medicine Faculty, Dumlupinar University, Kutahya / Turkey.
2 Faculty, Department of Neurosurgery, Kutahya Evliya Celebi Training and Research Hospital, Kutahya / Turkey.
3 Assistant Professor, Department of Pathology, Medicine Faculty, Erzincan University, Erzincan / Turkey.
4 Assistant Professor, Department of Pathology, Medicine Faculty, Erzincan University, Erzincan / Turkey.
5 Assistant Professor, Faculty of Medicine, Department of Emergency Medicine, Dumlupinar University, Kutahya / Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ayse Nur Deger, Department of Pathology, Medicine Faculty, Dumlupinar University, Kutahya, Turkey.
E-mail: ayhade@yahoo.com
Glomus tumours are benign lesions which are frequently seen on hand (particularly subungual region). In this report a 52-year-old male patient with glomangiomyoma on the left forearm has been presented. With a preliminary diagnosis of haemangioma, a subcutaneous well-circumscribed nodular lesion of the patient was excised. On histomorphological examination glomus cells, vascular structures and spindle-shaped smooth muscle cells were seen around it. Immunohistochemistry of smooth muscle cells and glomus cells showed positivity for smooth muscle actin. By means of these findings, the patient was diagnosed with glomangiomyoma. Glomus tumours are rare in the forearm (In the literatüre there are two cases). Moreover, glomangiomyomas are the least common histomorphological type of glomus tumour and are generally seen in the lower extremity. In the literature, a few cases of glomangioma and solitary glomus tumour has been described on the forearm histologically and only a few glomangiomyoma cases on forearm location. We have presented the glomangiomyoma on the forearm as a rarely-seen case. Early diagnosis of the glomangiomyoma on the forearm is of importance for the prevention of morbidity.
Glomus body, Glomus tumour, Upper extremity, Vascular lesion
Case Report
A 52-year-old male patient presented with a history of lesion on left forearm, which had been growing slowly for the last 6 months and was admitted to the department of dermatology. Physical examination revealed a 1.5 X 1 cm round mobile subcutaneous nodular lesion [Table/Fig-1a&b].
Solid nodular lesion is seen on left forearm.

During the physical examination, lesion was tender and mildly painful. Routine laboratory tests were within normal limits. In dermatoscopy, the lesion was interpreted as a vascular lesion. With the preliminary diagnosis of haemangioma, it was decided to be excised. Well-defined dark blue lesion from the surrounding tissue was seen. Surgical exploration was performed under local anaesthesia Within the normal limits of surrounding tissue, the lesion was totally excised.
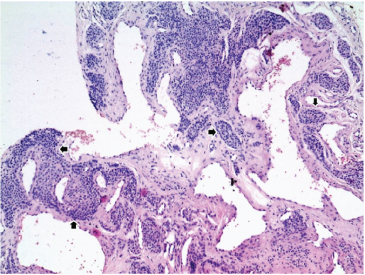
On macroscopic examination a 5 mm-diameter non-encapsulated, much well-circumscribed than surrounding tissue, dark-blue mass extending to subcutaneous tissue was seen. On microscopic examination a single layer of vascular channels lined by flat endothelial cells were seen. Around vascular channels, monomorphic round cells were observed. These cells were uniform, with round, oval, dark-stained nuclei and eosinophilic cytoplasm [Table/Fig-2,3].
Uniform tumour cells around the dilated blood vessels (H&E, 10X).
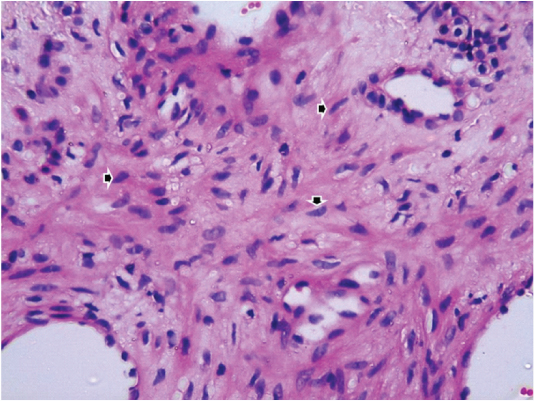
Elongated, spindle-shaped smooth muscle cells having blunt ended nuclei were observed at the site of vascular channels [Table/Fig-4]. IHC was carried out. Glomus cells and spindle-shaped cells were positive for Smooth Muscle Actin (SMA) [Table/Fig-5]. To rule out intradermal nevus S100 was used; but negative reaction for S100 was seen in these cells [Table/Fig-6a&b]. In glomus cells, signs of malignancy such as increased mitotic activity, necrosis, pleomorphism were not seen. By evaluating these histomorphological and immunohistochemical data, the patient was diagnosed with glomangiomyoma.
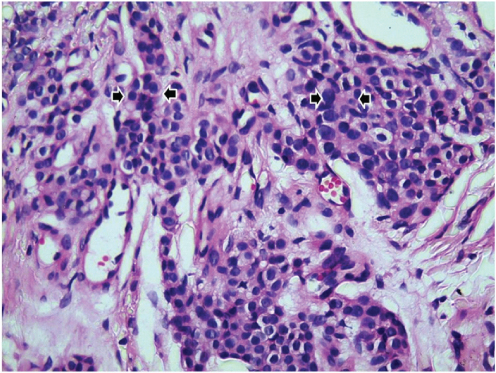
Uniform tumour cells around the dilated blood vessels (H&E, 40X).
Spindle shaped elongated smooth muscle cells which have blunt ended nuclei are observed around the vessels (H&E, 40X).
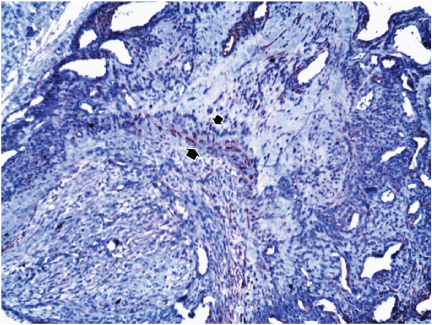
Diffuse cytoplasmic reactions with smooth muscle actin stain, on the smooth muscle cells (arrows) (SMA,10X).
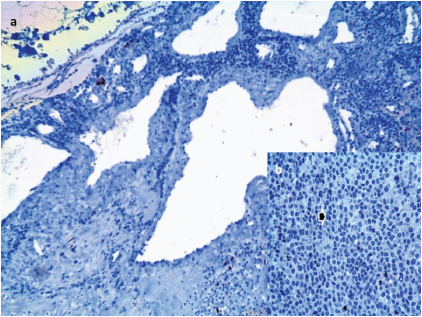
Negative reaction for S100 on the glomus cells S100X10; b) Negative reaction for S100 on the glomus cells (S100, 40X).
Discussion
Glomus bodies are the neuromyoarterial histological structures located on the stratum reticularis of the dermis and they are functioning in regulation of the body temperature by arteriovenous flow [1–3]. Glomus tumours are originated from neuromyoarterial structures forming the glomus body [1,4].
Immunophenotyping and electron microscopic studies indicate that glomus tumour possibly originates from the smooth muscle cells on the walls of blood vessels [1]. So, it is thought that the tumour is formed by the modified smooth muscle cells [4]. Glomus tumours are benign well bordered neoplasias forming less than 2% of all mesenchymal neoplasias [2,3].
The presented case was a rare settlement area with respect to the location. Glomus tumour has two clinical forms, known as multiple and solitary. While most of them are in solitary form, approximately 10% are in multiple forms [2]. Multiple forms are frequently seen on Glomovenous Malformations (GVM), known as glomangioma in the past. GVMs are rare lesions and they are related with localized gene on chromosome 1p21-22 [5].
Glomus tumours are uniformly seen in both sexes in adult age group. They are frequent in 20-40 age interval. Glomus tumour can be seen spontaneously or paroxysmal intense pain is observed in glomus tumour. On the other hand, glomangiomas are generally painless lesions [1].
Glomus tumours are clinically well circumscribed subcutaneous nodules whose colour is pink-purple and whose diameter under 1 cm. Histologically they are well-defined, non-encapsulated lesions and includes 3 components. The first component is the vessel structures separated by collagen tissue. The second component is modified perivascular smooth muscle cells. These cells are named as glomus cells. They are cuboidal, round formed cells with narrow cytoplasm and they form alveolus around veins. The third component is the smooth muscle fibres that can be separately identified inside the lesion [1,4]. Histologically three type of glomus tumour is available according to the rates of these three components. . These are solid glomus tumour (25%), glomangioma (60%) and glomangiomyoma (15%).
If smooth muscle fibres are observed in a glomangioma where both solid glomus tumour and vascular components are condense then the lesion is named as glomangiomyoma. Glomus tumour is frequently seen on hand, finger and nail bed [3,4]. It was reported in the literature that glomus tumour is an unusual settler on ankle, foot, knee, femur and hip [4]. When we scanned pubmed we encountered 2 case presentations which were related to glomus tumour on forearm. One of them was a solitary glomus tumour and the other was a case which was clinically multiple and histomorphologically glomangioma [6,7].
There were glomangiomyoma cases in the literature in different locations as well [3,8]. We saw only a few glomangiomyoma cases on forearm location when we scanned the literature [9]. We presented this case report as a rare condition.
Glomus cells are immunohistochemically positive for vimentin, smooth muscle actin, neuron specific enolase despite their negativity for cytokeratin and S100. In case, diagnosis cannot be made histologically, immunohistochemical examination may be helpful for a differential diagnosis in such lesion groups [1]. In addition to that, intradermal nevus, haemangioma and other vascular lesions should be considered at the differential diagnosis. Soft tissue lesions such as leiomyoma, ieiomyomasarcoma with epitheloid differentiation and rabdomyomasarcoma should be considered as well [4].
Surgical method of treatment is total excision. With the inclusion of surrounding normal tissue, a wide excision should be performed [1,2,4]. After conservative excision, recurrence rate is around 10% [1]. Studies have shown that after such wide excisions, no recurrence is noted [1]. Glomus tumours are known as benign lesions. However, rare cases have been reported as atypical and malignant glomus tumours [1,2]. If there are signs of malignancy in lesions, wide excision should be applied and a close follow-up of patient is required for regional and distant metastases [1].
Conclusion
In the literature, a few cases of glomangioma and solitary glomus tumour has been described on the forearm histologically and only a few glomangiomyoma cases on forearm location. Late diagnosis of the lesion can lead to morbidity in patients. In addition, although rare, malignant and atypical forms of glomus tumour are seen. For early diagnosis this rare lesion, localization and rare histological forms are important to be kept in mind by clinicians and pathologists.
[1]. Gencosmanoglu R, Inceoglu R, Kurtkaya-Yapicier O, Glomangioma of the hipDermatol Surg 2003 29(12):1244-47. [Google Scholar]
[2]. Nishida K, Watanabe M, Yamamoto H, Yoshida R, Fujita A, Koga T, Glomus tumour of the esophagusEsophagus 2013 10:46-50. [Google Scholar]
[3]. Siddiqui NH, Rogalska A, Basil IS, Glomangiomyoma (glomus tumour) of the kidneyArch Pathol Lab Med 2005 129(9):1172-24. [Google Scholar]
[4]. Frumuseanu B, Balanescu R, Ulici A, Golumbeanu M, Barbu M, Orita V, Topor L, A new case of lower extremity glomus tumour up-to date review and case reportJ Med Life 2012 5(2):211-14. [Google Scholar]
[5]. Farias MM, Kolbach M, Perez M, Gonzalez S, Hasson A, Acquired telangiectatic plaque-like glomangioma on the foreheadInt J Dermatol 2013 52(6):731-32. [Google Scholar]
[6]. Hrubý J, Novotny R, Spacek M, Mitáš P, Hlubocký J, Janák D, Povýšil C, Lindner J, Surgical extirpation of glomus tumour from rare localization on the upper extremityCase Rep Vasc Med 2013 [Google Scholar]
[7]. Lee S, Le H, Munk P, Malfair D, Lee ChH, Clarkson P, Glomus tumour in the forearm: a case report and review of MRI findingsJBR-BTR 2010 93(6):292-95. [Google Scholar]
[8]. Kim JA, Lee ES, Lee DY, A case of acquired multiple plaque-like glomangiomyomaClin Exp Dermatol 2010 35(2):202-04. [Google Scholar]
[9]. Yang JS, Ko JW, Suh KS, Kim ST, Congenital multiple plaque-like glomangiomyomaAm J Dermatopathol 1999 21(5):454-57. [Google Scholar]