Rare Mimickers of Exostosis: A Case Series
Phani Chakravarty Mutnuru1, Lakshmi Manasa Perubhotla2
1 Assistant Professor, Department of Radiology, Nizam’s Institute of Medical Sciences, Punjagutta, Hyderabad, Telangana, India.
2 Ex Lecturer, Department of Pathology, Nizam’s Institute of Medical Sciences, Punjagutta, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Phani Chakravarty Mutnuru, Department of Radiology, Nizam’s Institute of Medical Sciences, Punjagutta, Hyderabad-500082, Telangana, India.
E-mail: phani_chakravarty@yahoo.co.in
Exophytic growths from bones are a common entity. Osteochondroma is the most common benign exophytic lesion and we tend to diagnose every benign looking exophytic lesion as osteochondroma. Here we reported two entities of cases, one was Nora’s lesion and another one was supracondylar process of humerus, both of which were mimickers of osteochondroma and their salient and differentiating features from osteochondromas.
Nora’s lesion, Osteochondroma, Supracondylar process of humerus
Introduction
Osteochondroma is the most common benign tumour of bone and seen upto 1%–2% of individuals undergoing extensive radiographic evaluation [1]. Even though the diagnosis of osteochondroma is straight forward due to characteristic radiological findings, few other bony lesions like Nora’s lesion and supracondylar process of humerus can create diagnostic and theurapeutic challenge due to the extremely rare presentation and imageological and clinical similarity to the more common osteochondromas. Here we reported series of four cases, two of them were Nora’s lesion and rest were supracondylar process of humerus. The clinical and histopathological findings are summarized below.
Case series
| S. No. | | Patient-1 | Patient-2 | Patient-3 | Patient-4 |
|---|
| 1 | Age (Y) | 25 | 38 | 16 | 8 |
| 2 | Gender | Female | Male | Female | Male |
| 3 | Site | Left middle finger | Right thumb | Left lower arm. | Right elbow |
| 4 | Clinical features | Slightly painful swelling at left middle finger since one year with history of trauma two years back. | Slightly painful swelling at distal aspect of right thumb since 10 months. | Minimal pain at left lower arm due to blunt injury. | Pain and swelling right elbow with history of fall onto ground. |
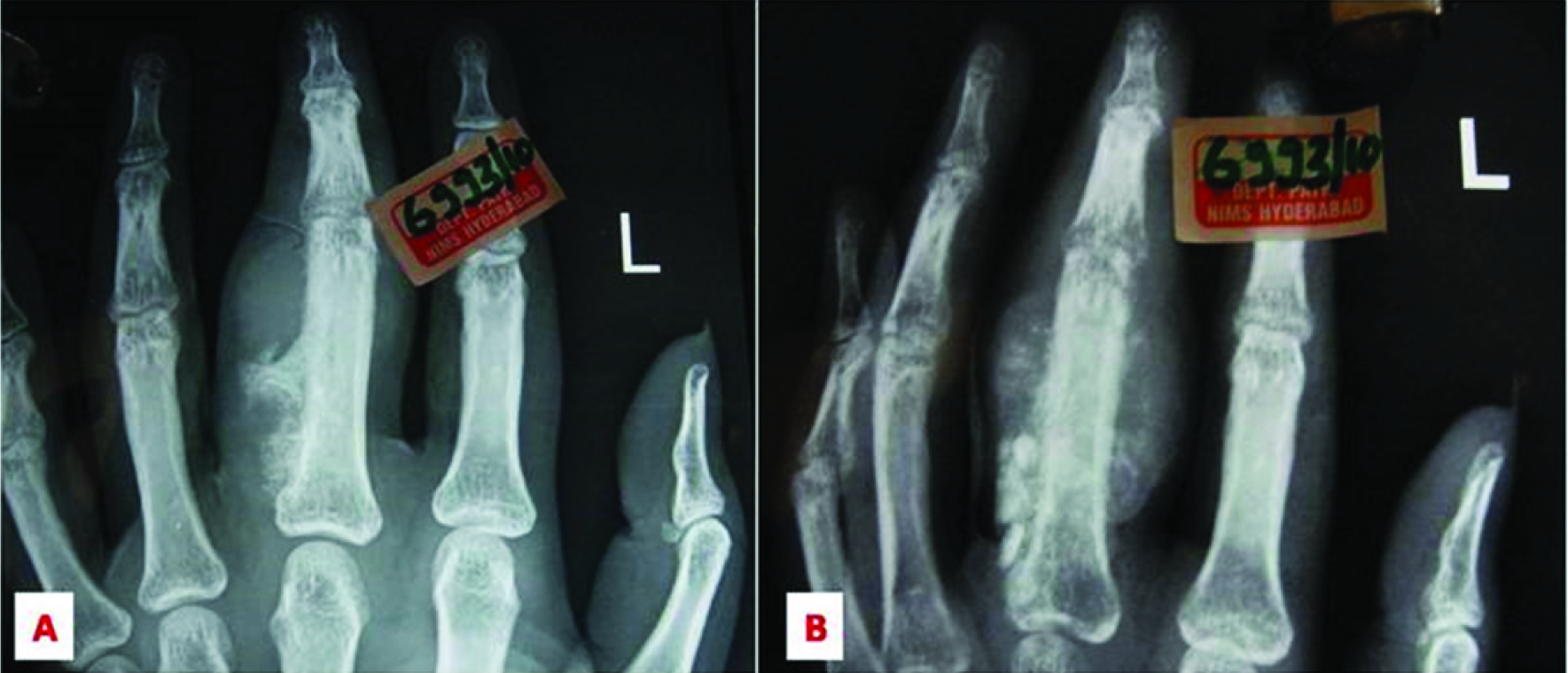
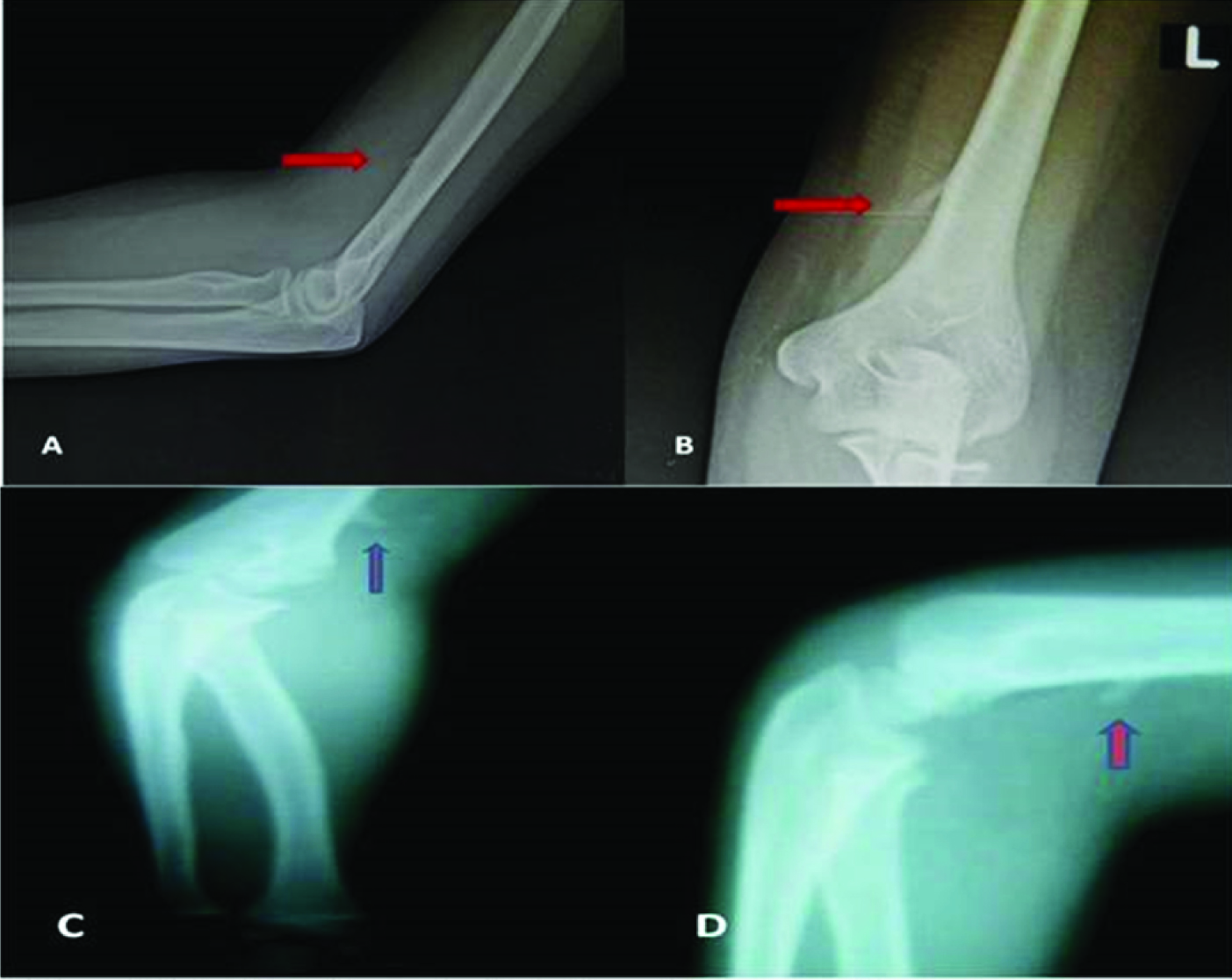
| 5 | Radiographic findings | Well defined, exophytic, osseous lesion arising from medial aspect of proximal phalanx of left middle finger with adjacent soft tissue swelling [Table/Fig-1a,b]. | Well defined, exophytic, osseous lesion arising from medial aspect of distal phalanx of right thumb with adjacent soft tissue swelling.[Table/Fig-3] | A small bony excrescence arising from anteromedial margin of distal 1/3rd of left humerus projecting towards elbow joint.[Table/Fig-4a&b] – s/o supracondylar process of humerus. | A small bony excrescence arising from anterior margin of distal 1/3rd of right humerus projecting towards elbow joint [Table/Fig-4 c&d]- s/o supracondylar process of humerus. |
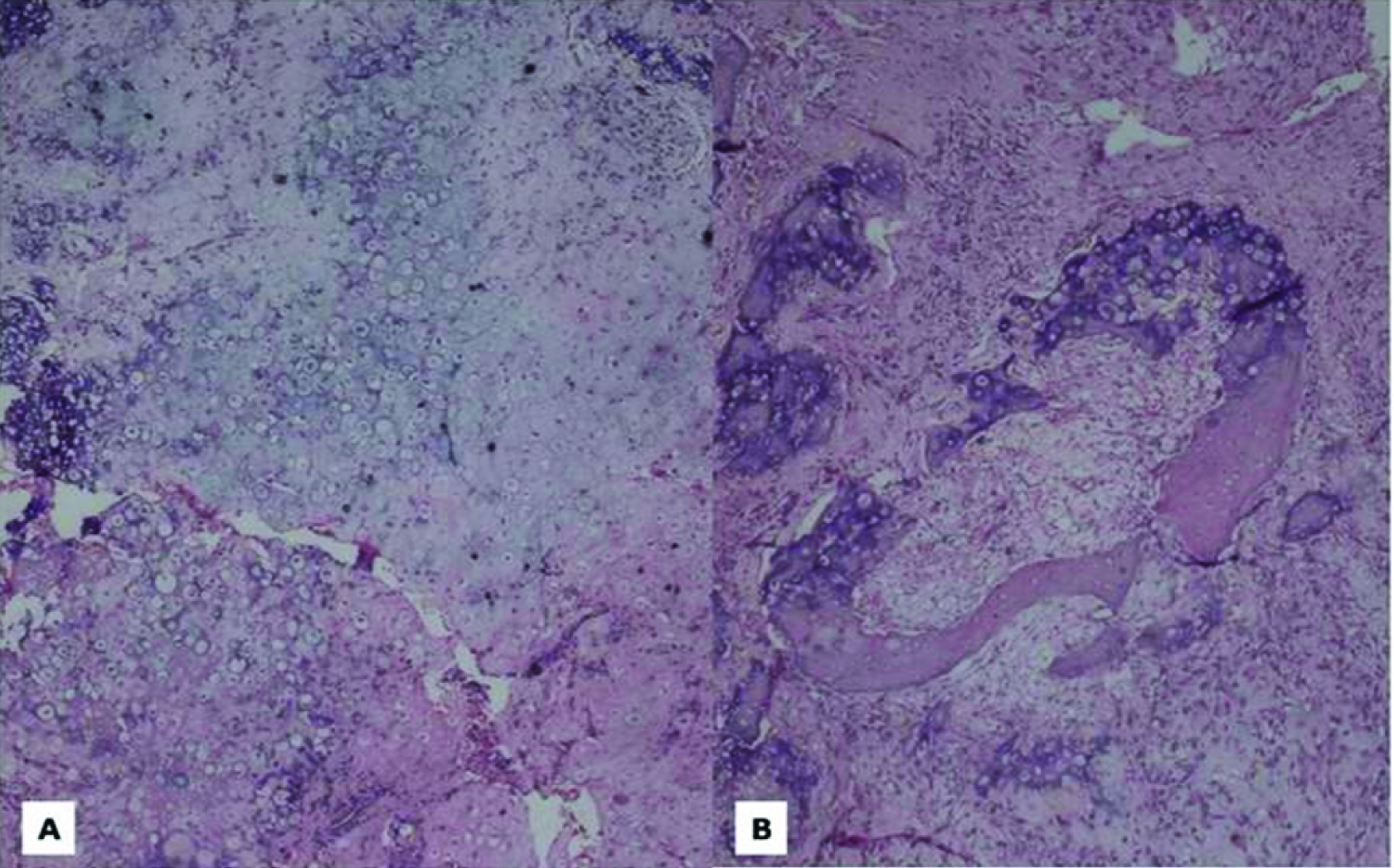
| 6 | Histopathological findings | Nora’ s lesion [Table/Fig-2a,b]. | Nora’ s lesion | - | - |
Discussion
Nora’s Lesion
Nora’s lesion, also known as Bizarre Parosteal Osteochondromatous Proliferation (BPOP), is a lesion of osteochondromatous origin that was first described in 1983 by Nora et al., in a report of 35 cases [2,3]. The cause is unknown and it might be related to a reparative process following trauma to the periosteum, as this finding was noted in 30% of cases in the series of Meneses et al., [4]. In our series, history of trauma was present in one case. Most of patients are in their third to fourth decades, and both sexes are affected equally [4]. The tumour usually affects bones of the distal extremities (hands and feet), but can also be found in long bones and mandible [4,5]. It generally presents as a minimally painful, pedunculated mass with slow growth for months or years [4].
In standard radiographs, Nora’s lesion is generally well marginated, but with lack of communication with underlying medullary canal [6] and lacks characteristic orientation away from nearby physis [Table/Fig-1], whereas osteochondromas have communication with medullary canal and shows characteristic orientation away from physis and more common in long bones than distal extremities [4,5,7].
Radiograph of left hand shows well defined, exophytic, osseous lesion arising from medial aspect of proximal phalanx of left middle finger with adjacent soft tissue swelling with no continuity of lesion with medulla.
In MRI, the tissues within the Nora’s lesion show signal characteristics that differ sharply from normal bone and cartilage. The lesion is dark on T1 and bright on T2, which is a typical pattern for neoplastic lesions. Whereas, in osteochondromas, the signal characteristics of the bony parts of the lesion are typical of normal bone [8].
Histopathologically in Nora’s lesion, bony trabeculae are typically covered by a cartilaginous cap with irregular endochondral ossification [6]. The cartilaginous component shows irregular groups of numerous, bizarre, and enlarged chondrocytes which are commonly binucleated [3] [Table/Fig-2]. This contrasts with the more regular alignment of chondrocytes in osteochondromas.
H&E stained section shows: (a) lesion comprised of hypercellular cartilagenous plate and bizarre, enlarged chondrocytes with pleomorphism; (b) calcification and enchondral ossification within the lesion and intertrabecular space showed loosely arranged spindle cells.
Nora’s lesion requires more extensive surgical resection than for osteochondroma with a higher recurrence rate upto 55% [Table/Fig-3]. Michelsen et al., described that excising suspicious-looking cortex and the adjacent periosteal tissue was beneficial in preventing recurrence [6].
Radiograph of both hands shows well defined, exophytic, osseous lesion arising from medial aspect of distal phalanx of right thumb with adjacent soft tissue swelling without continuity of lesion with medulla of distal phalanx.

Supracondylar Process of Humerus
In 1854, Sir John Struthers described a supracondylar process (or spur) which was a bony projection on the anteromedial aspect of the humerus about 5 cm above the medial epicondyle. Sometimes a band of fibrous tissue (Struther’s ligament) may join the medial epicondyle with the apex of this process [9].
The incidence of the supracondylar process is 0.3%-2.7% of the population [10]. It can be uni- or bilateral. A supracondylar process may cause symptomatic compression of the median nerve and/or brachial artery [9,10]. More rarely, ulnar nerve compression can also occur.
In standard radiograph, supracondylar process of humerus is oriented distally, towards the elbow joint without continuity with the cortex of the humerus [Table/Fig-4a-d], whereas an osteochondroma points away from the joint and the cortex of the lesion is continuous with the cortex of humerus [11].
(a,b) Radiograph of left elbow shows a small bony excrescence arising from anteromedial margin of distal 1/3rd of left humerus projecting towards elbow joint. (c,d) Radiograph of right elbow shows a small bony excrescence arising from anterior margin of distal 1/3rd of right humerus projecting towards elbow joint/
If there is neurovascular compression, continuous pain or fracture in the supracondylar process/spur, surgery is indicated [10,12]. Surgical management consists of excision of the supracondylar process along with Struthers ligament. However due to chances of recurrence, it is recommended that the process be removed together with the overlying periosteum [10,12].
Conclusion
In conclusion, even though osteochondroma is most common cause of benign exophytic lesions and its diagnosis is simple and straightforward, other causes can mimic it and knowledge of them is essential for differential diagnosis and surgical management.
[1]. Resnick D, Kyriakos M, Greenway GD, Osteochondroma. In: Resnick D, edsDiagnosis of bone and joint disorders 1995 Vol 53rd edPhiladelphia, PaSaunders:3725-46. [Google Scholar]
[2]. Rana P, Duhan A, Verma S, Siwach RC, Bizarre parosteal osteochondromatous proliferation of phalanxIndian J Pathol Microbiol 2013 56(1):71-72. [Google Scholar]
[3]. Twiston Davies CW, Bizarre parosteal osteochondromatous proliferation in the hand. A case reportJ Bone Joint Surg 1985 67(4):648-50. [Google Scholar]
[4]. Meneses M, Krishnan U, Swee R, Bizarre parosteal osteochondromatous proliferation of bone (Nora’s lesion)Am J Surg Pathol 1993 17(7):691-97. [Google Scholar]
[5]. Abramovici L, Steiner GC, Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bonesHum Pathol 2002 33:1205 [Google Scholar]
[6]. Michelsen H, Abramovici L, Steiner G, Posner MA, Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) in the handJ Hand Surg 2004 29A:520 [Google Scholar]
[7]. Nora FE, Dahlin DC, Beabout JW, Bizarre parosteal osteochondromatous proliferations of the hands and feetAm J Surg Pathol 1983 7:245 [Google Scholar]
[8]. Torreggiani WC, Munk PL, Al-Ismail K, O’Connell JX, Nicolaou S, Lee MJ, MR imaging features of bizarre parosteal osteochondromatous proliferation of bone (Nora’s lesion)Eur J Radiol 2001 40(3):224-31. [Google Scholar]
[9]. Al-Qattan MM, Husband JB, Median nerve compression by the supracondylar process: A case reportJ Hand Surg 1991 16(1):101-03. [Google Scholar]
[10]. Ivins GK, Fulton MO, Supracondylar process syndrome : A case reportJ Hand Surg 1996 21(2):279-81. [Google Scholar]
[11]. Subasi M, Kesemenli C, Necmioglu S, Kapukaya A, Demirtas M, Supracondylar process of the humerusActa Orthop Belg 2002 68(1):72-75. [Google Scholar]
[12]. Spinner RJ, Lins RE, Jacobson SR, Nunley JA, Durham NC, Fractures of the supracondylar process of the humerusJ Hand Surg 1994 19(6):1038-41. [Google Scholar]