One of the challenges faced by the dentists in the dental clinics is the discomfort to patients caused by dentinal hypersensitivity, affecting 4-74% of adult population, for which there is no solution till date [1]. Dentinal hypersensitivity is a clinical condition characterized by short sharp pain arising from exposed dentine, which can occur through incorrect tooth brushing, gingival recession, inappropriate diet and because of various other factors [2]. The most accepted theory, which explains the mechanism of dentinal hypersensitivity is the hydrodynamic theory, according to which any stimulus to the exposed dentine, causes fluid to get displaced in the dentinal tubules which leads to activation of nerve endings at pulp-dentine interface, thus leading to pain [3]. Till date, little is known about the precise aetiology of dentine hypersensitivity and its effective treatment. The most commonly used treatment methods which have been extensively studied are, blocking the exposed dentinal tubules and reducing the excitability of sensory nerves. However, most of the therapies are still not completely effective, the use of dental lasers has been cited as a possible new approach for treating this condition and has become a subject of intensive research.
Desensitization caused by different lasers depends on multiple factors like type of laser device and various irradiation parameters like adequate power density, wavelength, wave mode, pulse frequency and times of repeated irradiation. Recently, application of various lasers, including Nd: YAG (Neodymium-doped: Yttrium-Aluminium-Garnet) [4,5], CO2 (Carbon Dioxide) [6], Er:YAG (Erbium-doped: Yttrium-Aluminium-Garnet) [7], He:Ne (Helium- Neon) [8] and 810-nm Diode lasers [9] have been found to be effective in providing a solution to the problem of dentine hypersensitivity to a great extent.
Nd: YAG laser is thought to affect dentine hypersensitivity, by obliterating or narrowing the dentinal tubules, which occurs due to melted hydroxyapatite crystals induced by the laser heat [10]. An exposure to Nd: YAG laser energy even for a short time leads to morphological changes of dentine surface characterized by a glazed, melted, re-solidified surface and sometimes even by the formation of globules and cracks [11]. It has also been reported that energy from non-penetrating type, long wavelength CO2 lasers can be used for surgical applications and effective treatment modality for dentine hypersensitivity [12]. Even at moderate energy densities, CO2 laser has been found to achieve adequate sealing and obliteration of dentinal tubules, so as to resolve dentinal hypersensitivity [13]. However, the hazarduous effects like fissuring, charring, fracturing and cratering on the dentinal surface has been reported by the use of CO2 laser radiation [14]. Diode lasers have been found to mainly work by interacting with the dental pulp thus leading to induction of photobiomodulating effect, which causes an increase in cellular metabolic activity of odontoblasts and intensifing tertiary dentine production, thus obliterating the dentinal tubules [15]. Thus, although the use of lasers for the treatment of dentinal hypersensitivity is well proven and claimed, but it is still a controversy as to which laser is most effective for the treatment of dentine hypersensitivity. Therefore, an attempt was made in the present study to compare the effects of Nd:YAG, CO2 and 810-nm Diode lasers on width of exposed dentinal tubule orifices and to evaluate the morphologic changes on dentinal surface of human tooth by irradiation with these lasers, by means of scanning electron microscope (SEM).
Materials and Methods
The present in-vitro study was conducted over a period of four months i.e., started in Jan 2015 and completed in April 2015. A total of 40 specimens were obtained from 10 freshly extracted human premolars due to orthodontic reasons, after approval of the ethical committee of Sri Gobind Tricentenary Dental College, Hospital, and Research Institute, Budhera, Gurgaon. The inclusion criteria’s were teeth extracted from subjects between 12-25 years of age, of both the sexes with healthy periodontium. The teeth which had caries on crown or root, restoration or fillings, tooth crack or fractures, pulp or periapical diseases before extraction, or teeth extracted from patient’s using desensitizing paste or mouthwash in the last three months prior to the extractions were excluded from the study. Immediately after extraction loose debris/calculus were removed by using Gracey’s curette no. 5-6 (Hu-fridey, USA) giving 50 apical cervical strokes and then the teeth were cleaned and rinsed in distilled water and kept immersed in distilled water with 0.01% thymol for a period of one week for disinfection. Transverse sections for each tooth at the Cemento-Enamel Junction (CEJ) and at 3mm distance, were done twice from the CEJ toward the apex, yielding two 3mm tall cylinders of the remaining root. After this, each cylinder was sectioned longitudinally using a high speed hand piece with copious water irrigation and a tapered fissure bur was used to obtain two dentine blocks approximately 3×3×1mm in size, thus yielding four sections from a single tooth. Thus, 40 root specimens were finally obtained. The horizontal shallow grooves for identification purpose were made on the pulpal surface and pulpal tissues of all the specimens were removed. After that, a thorough root planing was done for all the root surfaces and were flattened using a fine diamond tapered fissure bur for the removal of entire cementum and exposure of underlying dentine. Then the specimens were stored in small separate containers filled with distilled water until the laser application was done. Just before the laser irradiation, the specimens were submerged into 17% EDTA solution (pH =7.8) for 5 min to remove the smear layer and expose the dentinal tubules. Finally, the specimens were divided into four groups of 10 each. All the specimens excluding Group I were then lased at a predetermined site by a single practitioner using allocated laser radiation parameters as:
Group I: Control group treated with saline and not lased.
Group II: Nd:YAG laser {Wavelength:1,064nm; energy per pulse:40mJ; frequency:25Hz; power:1W; exposure time:30s; pulse duration:100ms; fiber delivery system:300μm silica fiber; distance:5mm perpendicular to sample; non contact mode with wet conditions [Fotona Light Walker (USA)]}.
Group III: CO2 laser {Wavelength:10,600nm; power:1W; frequency:50Hz; irradiation mode: continuous pulse mode; exposure time:30s; distance:1cm; non contact mode with wet conditions [Surgical Laser System (UM-L25, Brussela, Belgium)]}.
Group IV: 810-nm Diode laser {Wavelength:810nm; power:1W; irradiation time:30s; irradiation mode: continuous pulse mode; distance:1cm; fiber delivery system:400μm; non contact mode with wet conditions [Picasso Lite (Indianapolis, USA)]}.
The specimens were washed and dehydrated in a series of graded alcohol solutions (50%, 70%, 80%, 95%, 100%) for 10 minutes each. After two additional 10 minute washes in absolute alcohol, the specimens were dried overnight, mounted on SEM stubs. Mounted samples were coated with gold in a sputter coater (Polaron SC7640, UK). The coated specimens [Table/Fig-1] were examined using SEM (Carl Zeiss EVO40, Germany) at JNU, New Delhi. Photomicrographs of the central portion of each specimen were taken at 1500x magnification. These photomicrographs depicted partially or totally occluded dentinal tubules [Table/Fig-2,3,4 and 5]. The calculations were done by one single examiner, who was not aware of the type of laser used while examining. Six dentinal tubules were evaluated twice and their average was taken for calculating the dentinal tubule diameters (μm or nm), using Scale-bar software running on the SEM on the photomicrograph. The surface morphological changes like regular, irregular or flaky surface before and after laser irradiation were also recorded [Table/Fig-6,7,8 and 9].
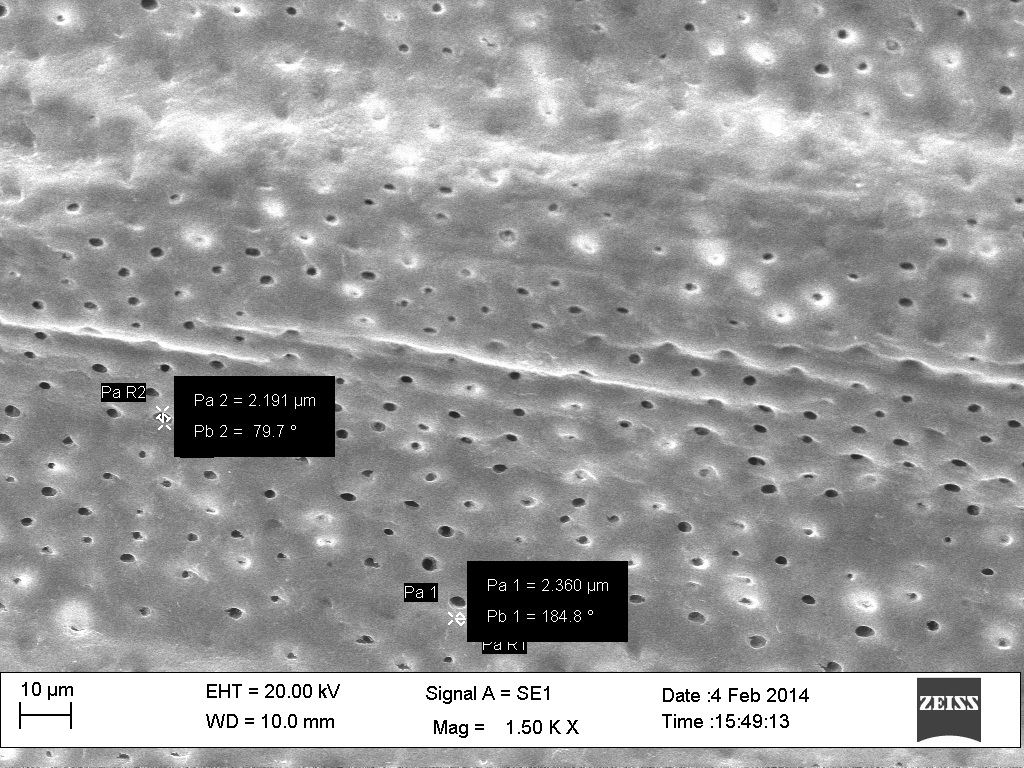
SEM photomicrographs (Group I: Control Group) depicting open dentinal tubules.
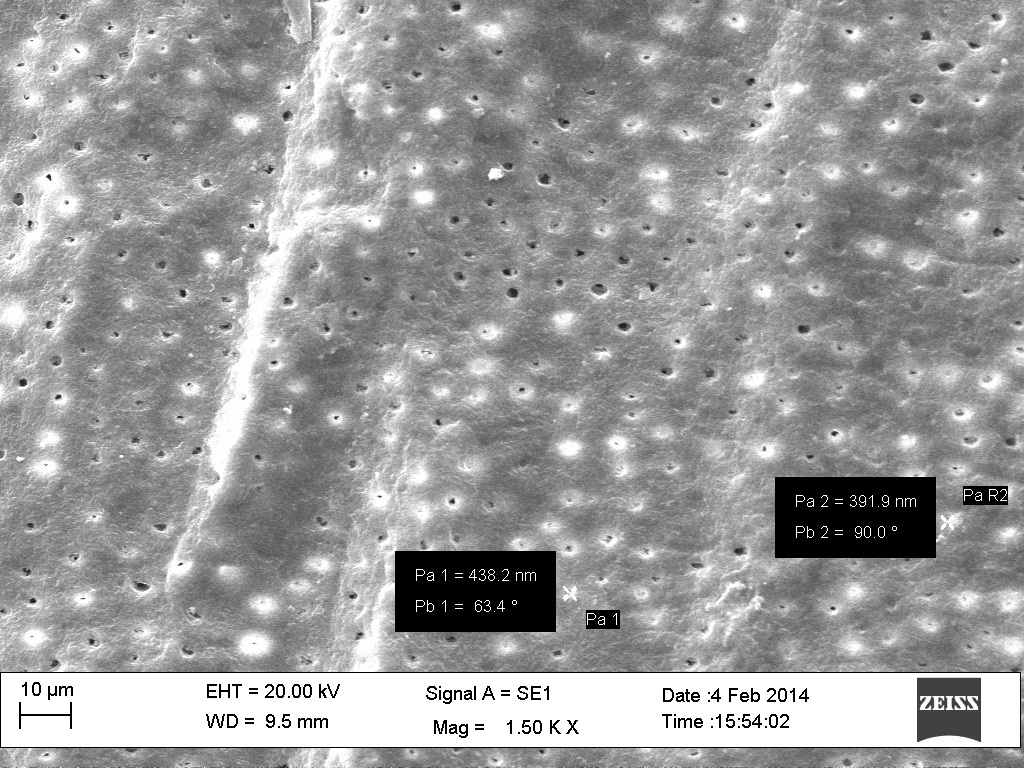
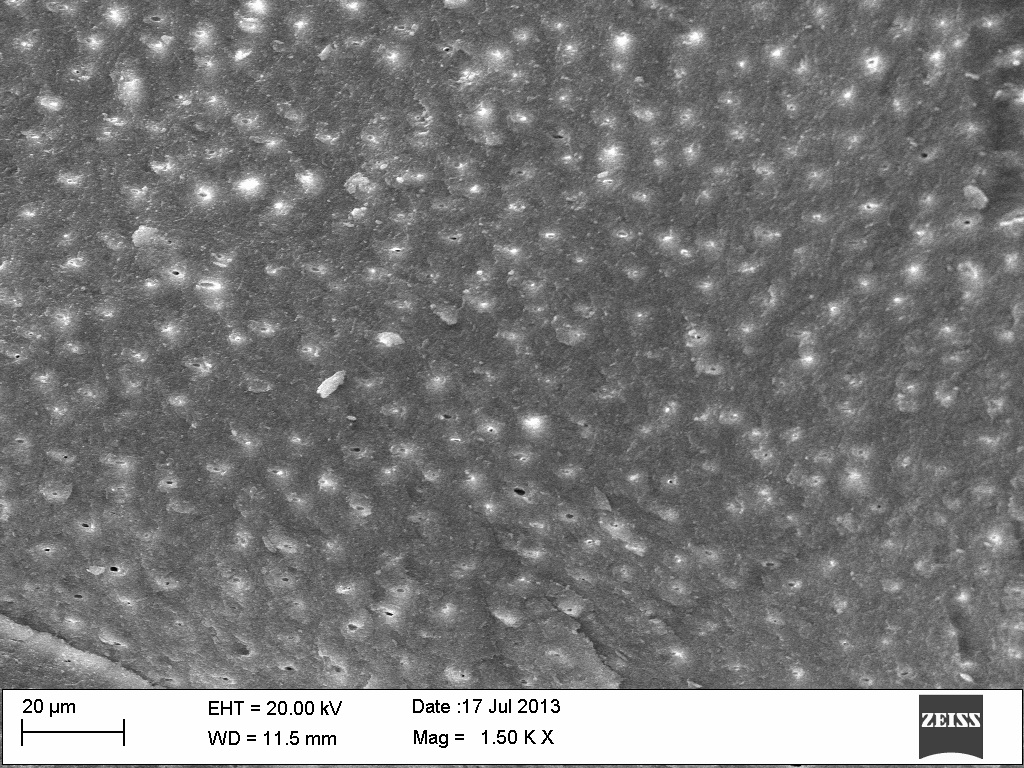
SEM photomicrographs (Group II: Nd:YAG Laser) depicting mostly obliterated dentinal tubules.
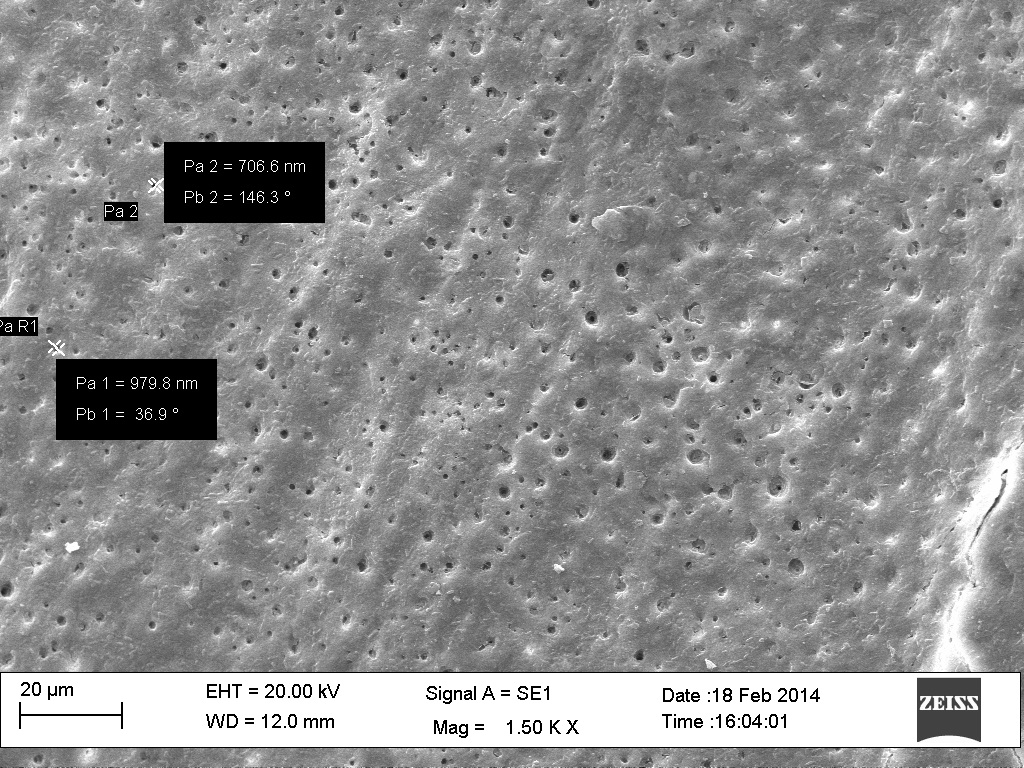
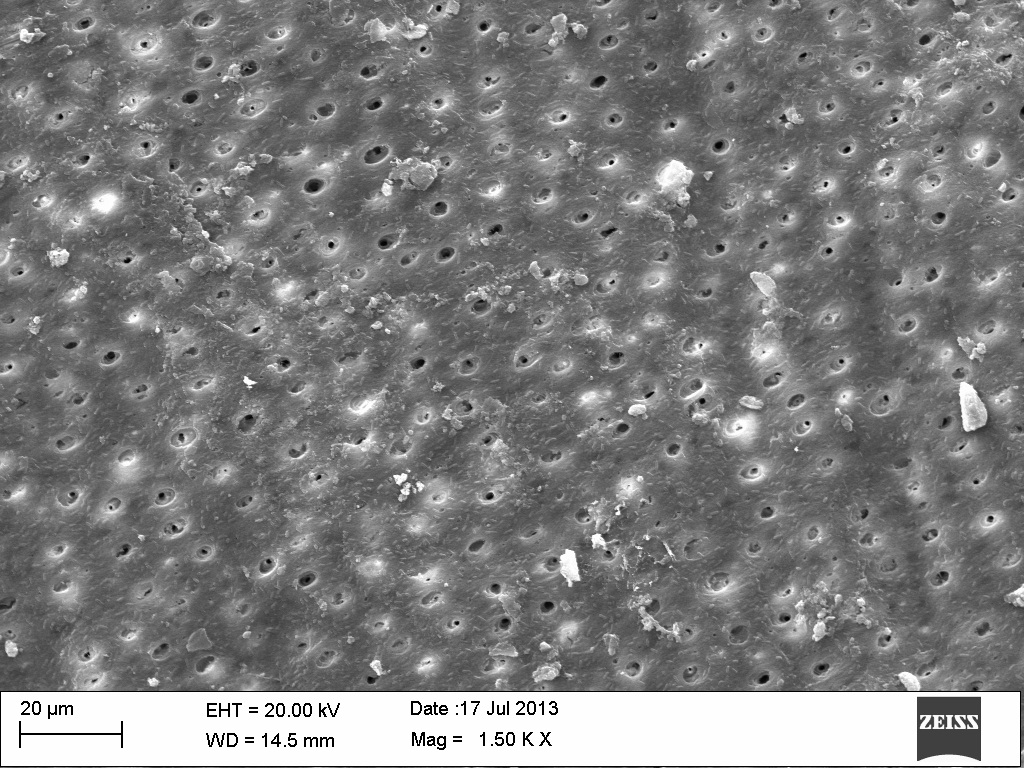
SEM photomicrographs (Group III: CO2 Laser) depicting partially obliterated dentinal tubules.
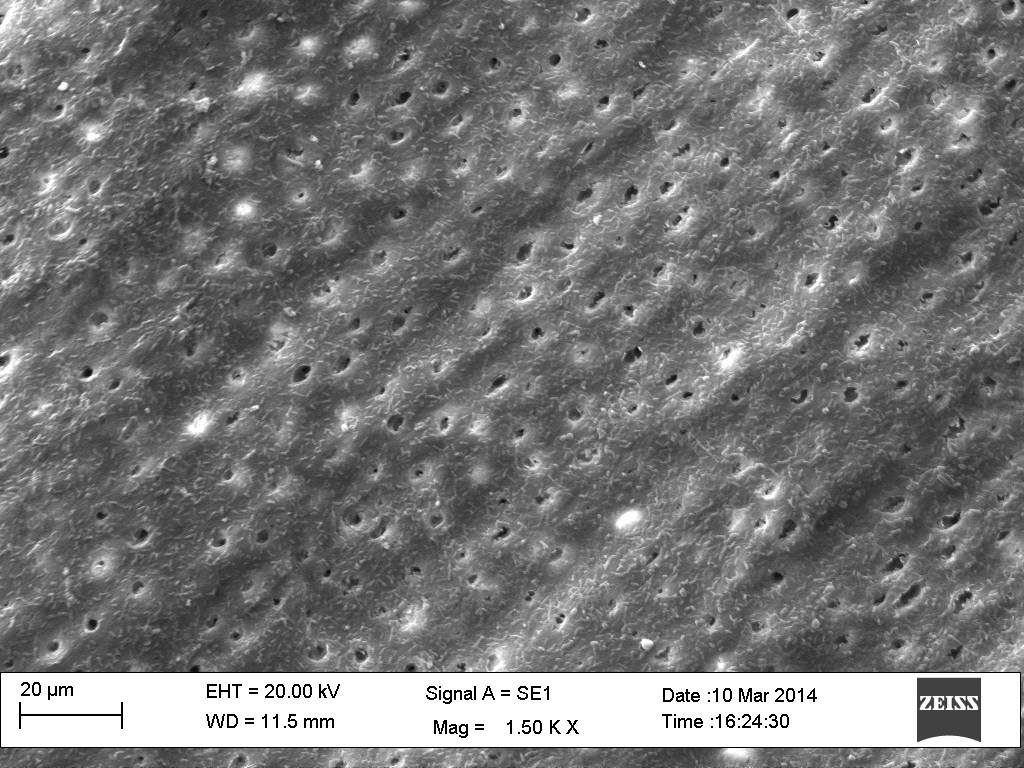
SEM photomicrographs tubules (Group IV: 810-nm Diode Laser) depicting slightly oblterated dentinal tubules.
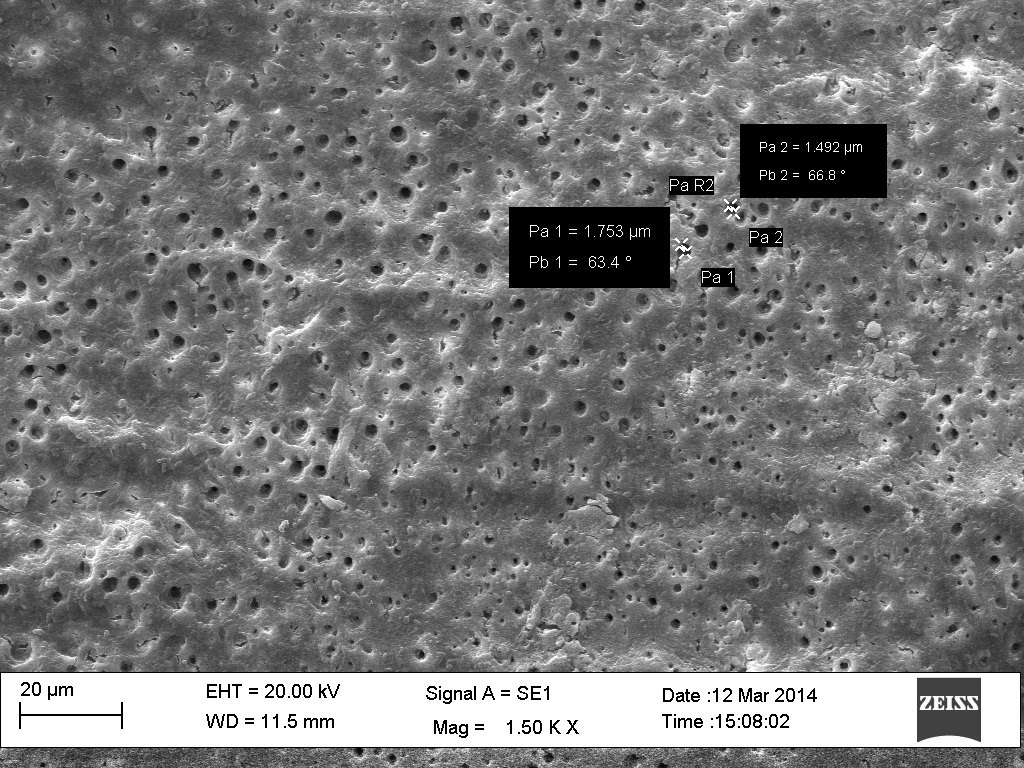
SEM photomicrograph (Group I: Control group) depicting smooth and regular surface before laser irradiation.
SEM photomicrograph (Group II: Nd: YAG Laser) depicting morphologic variations like irregular, glazed surface.
SEM photomicrograph (Group III: CO2 Laser) depicting morphologic variations like irregular surface with cracks.
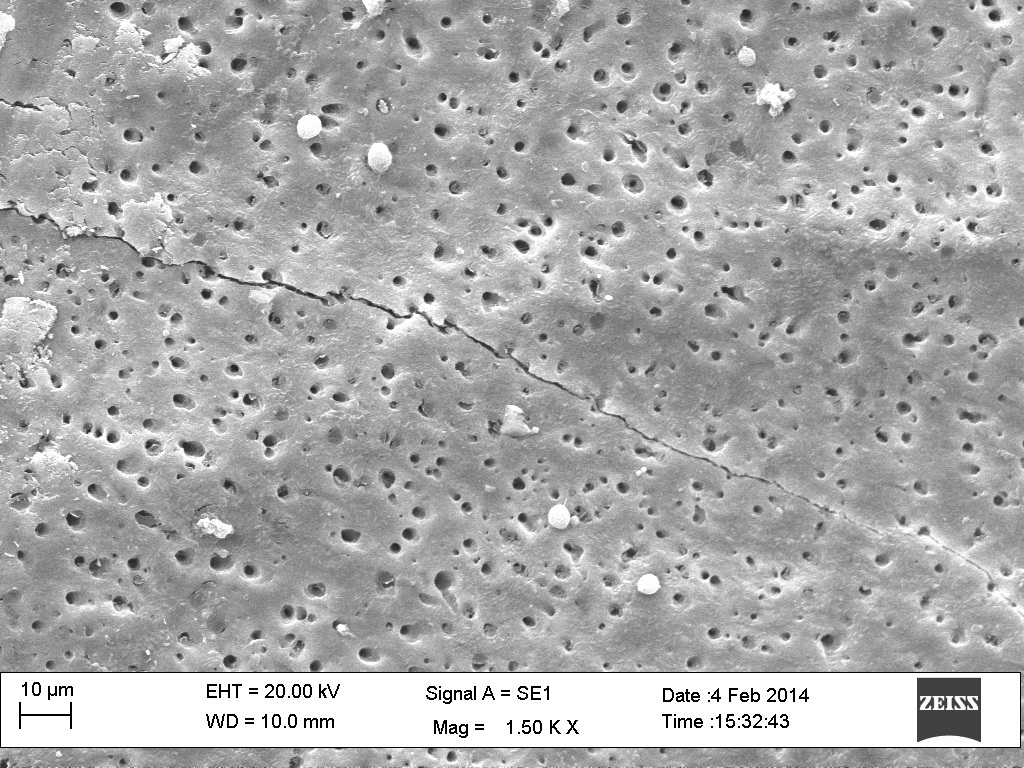
SEM photomicrograph (Group IV: Diode Laser) depicting mild morphologic variations with a smooth surface.
Statistical Analysis
The data were analyzed using Statistical Package for Sciences (SPSS Inc, Chicago, IL) version 16.0 for windows. Parametric one-way ANOVA test was used to compare within groups and Turkey’s Post Hoc multiple range test was used to find the difference between the groups at level p<0.05. The level of statistical significance was set at 95% (p=0.05). The results were interpreted as highly significant with a p-value <0.001.
Results
All the tubule diameters were measured in micrometer (μm). The results of intergroup comparison of dentinal tubular diameter of control group and laser irradiated groups were found to be highly statistically significant. In Group II i.e., after irradiation by Nd: YAG laser, the mean dentinal tubular diameter was found to significantly reduce from 2.612 ± 0.838 to 0.719 ± 0.302 and the reduction was found to be 72.46% with a p-value of <0.001. Similarly, significant values were obtained on comparison of Group I i.e., Control group with Group III i.e., CO2 lased group and the mean dentinal tubular diameter was found to reduce from 2.612 ± 0.838 to 1.036 ± 0.359 with the reduction of 60.31% and highly significant p-value <0.001. Further, Group IV i.e., 810-nm Diode laser showed the mean dentinal tubular diameter to reduce from 2.612 ± 0.838 to 1.563 ± 0.326 and significantly high reduction of 40.14% was found in comparison to Group I with a p-value of <0.001. Thus, all the three groups showed a highly statistical significant result with maximum reduction in Nd:YAG laser group [Table/Fig-10,11].
Mean dentinal tubular diameter of all the groups.
| Group | Treatment | N | Tubular Diameter |
|---|
| Mean (μm) | Standard Deviation |
|---|
| I | (Control) Saline | 10 | 2.612 | 0.838 |
| II | Nd:YAG Laser | 10 | 0.719 | 0.302 |
| III | CO2 Laser | 10 | 1.036 | 0.359 |
| IV | Diode Laser | 10 | 1.563 | 0.326 |
Group I: Control group; Group II: Nd:YAG laser; Group III: CO2 laser; Group IV: Diode laser.
Intergroup comparison of dentinal tubular diameter of lased group as compared to the control group.
| Comparison Groups | Difference in Percentage Reduction of Tubular Diamemer (%) | p-value |
|---|
| I vs II | 72.46 | < 0.001 |
| I vs III | 60.31 | < 0.001 |
| I vs IV | 40.14 | < 0.001 |
ANOVA Test & Turkey Post Hoc test showed significant reduction in all the lased groups
Group I: Control group; Group II: Nd:YAG laser; Group III: CO2 laser; Group IV:Diode laser [p<0.001 is highly significant].
On comparison between the lased groups, a significant reduction of dentinal tubular diameter i.e., 30.60% was seen In group II i.e by Nd:YAG laser as compared to Group III i.e., CO2 laser. On comparison of Group III and Group IV, a significant reduction of 33.72% was found with the use of CO2 laser as compared to 810-nm Diode laser. Thus, maximum reduction of dentinal tubular diameter was observed with the use of Nd:YAG laser in comparison to 810-nm Diode laser (i.e., comparison between Group II and Group IV) and the results were found to be statistically significant i.e., a reduction of 54.00%. Thus, the results indicated maximum reduction of dentinal tubular diameter by Nd:YAG laser group followed by the CO2 laser group and then by 810-nm Diode laser group [Table/Fig-12].
Intergroup comparison of dentinal tubular diameter between groups irradiated by different lasers.
| Comparison Groups | Difference in Percentage Reduction of Tubular Diameter Reduction (%) | p-value |
|---|
| II vs IV | 54.00 | < 0.001 |
| III vs IV | 33.72 | < 0.001 |
| II vs III | 30.60 | < 0.001 |
ANOVA Test & Turkey Post Hoc test for multiple comparisons among the lased group.
Group II: Nd:YAG laser; Group III: CO2 laser; Group IV: Diode laser [p<0.001 is highly significant].
Discussion
Over a period of time, lasers in dentistry have proved to be a proficient option for treating dentinal hypersensitivity. Different tissue reactions, leading to clinical therapeutic effects depends on various properties of laser like its frequency, power density, wavelength, its active medium and the optical properties of the target tissue. In the present study, only a narrow range of 12-25yrs aged subject’s teeth were included, as it has been suggested that with advancing age, tubule lumen undergoes a decrease in diameter, by continuous deposition of minerals within the lumen and can even get completly obliterated as age progresses [16].
The first use of Nd:YAG laser was reported by Matsumoto K et al., for the treatment of dentinal hypersensitivity [17]. In the present study, it was found that the Nd:YAG laser showed a significant reduction of dentinal tubular diameter i.e., 72.46% as compared to the non-irradiated group (Control group). Similar significant reduction of 53.3% dentinal tubular diameter via mechanical occlusion was shown in another in-vitro study by the use of Nd:YAG laser as compared to non-irradiated group [18]. Even, on inter group comparison among three laser groups, maximum reduction in dentinal tubular diameter was seen by the use of Nd:YAG laser group as compared to CO2 laser group and Diode laser group. Similarly, a study has found, Nd:YAG laser to be very effective in treatment of dentinal hypersensitivity, suggesting that the heat produced by this laser can cause hydroxyapatite structure to melt, which resolidifies on cooling and forms larger size hydroxyapatite crystals as compared to initial structure, thus leading to partial or complete obliteration of dentinal tubules [19]. In the present study, the irradiation parameters used with power of 1W were found to be quite effective in occluding the dentinal tubules, with minimal hazardous effects like craters and cracks, wheras a study has reported that power setting of 0.5W is ineffective and more than 1W can cause irreversible damage to pulp and dentine [20]. However, as this was an in-vitro study, only the positive effect of Nd:YAG on obliteration of dentinal tubules could be evaluated, whereas some in-vivo studies have also determined its biostimulative property, leading to potential analgesic effect on pulp, thus suggesting it to be highly effective for the treatment of dentinal hypersensitivity [21].
The first use of CO2 laser for the treatment of dentine hypersensitivity was reported by Moritz A et al., [22]. This laser has a property of high hydroxyapatite and water absorption with low penetrating depth, thus leading to alteration of dentinal surface, even at moderate energy levels. In the present study, significant reduction of dentinal tubular diameter was observed by use of CO2 laser but lesser than Nd:YAG laser. Dentinal tubular diameter was found to be reduced significantly by 60.31%, with the use of CO2 laser with respect to control group. Nearly, similar results of 42.3% reduction in the mean value of tubular diameter via the melting of peritubular dentine were shown by Gholami GA et al., [18]. The possible mechanism could be that as CO2 laser energy gets highly absorbed in the dentinal hydroxyapatite, thus leading to excessive melting and recrystallization of dentine on cooling, and thus obliterating the dentinal tubules. The similar mechanism could be a possible reason of the successful tubular sealing by the use of CO2 laser, seen in our study too.
A significant reduction in dentinal tubular diameter of 40.14% was even seen by the use of 810-nm Diode laser when compared with the Control group, but it was much lesser when this group was compared with other two lased groups, which signifies that 810-nm Diode laser is not as effective as CO2 and Nd:YAG lasers for treatment of dentinal hypesensitivity. Similarly, an author reported that the 810-nm Diode laser caused a mild, random, and irregular melting in peritubular and intertubular dentine throughout the relevant site, thus causing partial obliteration of dentinal tubules [9]. Contrary to this, another author has found its minimal effect on dentinal tubular diameter and suggested that 810-nm Diode laser can only get poorly absorbed in hard dental tissues and cannot lead to desirable changes in micro-structure of dentin, and thus not very effective in obliterating the dentinal tubules [18] However, its definite role to treat dentinal hypersensitivity has been suggested by blocking depolarization of afferent fibres, and thus having a profound analgesic effect by depressing nervous signal transmission [23]. Thus, although biostimulatory action of Diode laser is well confirmed, but its action on occlusion of dentinal tubules is still controversial. This explains the mechanism of action for Diode laser, however further studies are required in this field to reach to a definitive conclusion.
This study also tried to evaluate the morphological variations seen on photomicrographs of all the three lased groups. The ultimate effect of laser irradiation depends on the distribution of energy inside the tissue. The process of heat conduction influences the rise in temperature at different distances from the irradiated site. Under SEM, Group I (Control group) which was non-irradiated group showed numerous exposed dentinal tubule orifices with regular and smooth, dentinal surface, as there was no heat conduction on the dentinal tubules [Table/Fig-6].
The Nd:YAG laser group (Group II) photomicrographs analysis on SEM showed obliterated dentinal tubules with irregular, glazed surfaces without any, black staining or charring of the dentinal surface. These features were also shown in a study done by Lan WH et al., [24]. On the contrary, craters had been mentioned as a possible side effect in a study performed by Gaspirc B and Skaleric U [25], but in our study we didn’t find any craters or cracks following Nd:YAG laser irradiation [Table/Fig-7].
On the other hand, specimens irradiated by CO2 laser group (Group III) showed a charred dentinal surface with craters and cracks. These results were found to be similar to a study, which found charred regions of dentine which would indicate temperature sufficiently high to carbonize the organic matter of the dentine. The possible reason for cracks formation by the use of CO2 laser could be the shrinkage of organic crystals of dentine, owing to its property of high absorption in water [Table/Fig-8] [7].
The specimens treated by 810nm-Diode laser (Group IV) showed least morphologic changes as this laser shows least absorption in hard tissues. This laser caused very mild and not appreciable morphologic changes of the dentine [Table/Fig-9]. On photo-micrographs minor tubular occlusion, with almost a smooth and regular surface was observed with the 810-nm diode laser. A study done by Umana M et al., reported that 810-nm Diode laser at power output 0.8 - 1W and continuous wave mode, similar to the parameters taken in our study, slightly reduced the diameter of dentinal tubules without causing craters, cracks and charring effect, whereas higher output power (1.6-2W) resulted in these hazardous effects [9].
Thus, the results of the present study justify the use of above mentioned lasers to be beneficial as an alternative treatment modality for dentinal hypersensitivity, as it successfully causes occlusion of dentinal tubules. These properties of lasers makes them highly attractive and effective therapy for dentinal hypersensitivity.
Moreover, it is proposed that before coming to any conclusion for the selection of laser, based on efficiency in causing the occlusion of exposed dentinal tubules, one should look into the parameters such as wavelength, output power, exposure time, mode of action, etc., along with the mechanism of action of the laser to be used. It has also been well documented that Nd: YAG and Diode laser, owing to their lower absorption in hydroxyapatite and water and deeper penetration into the dentinal tubules, have an affect on the nerve endings whereas no biostimulative or any effect on nerve analgesia has been reported for CO2 laser.
Limitation
As the present study was an in-vitro one, hence the direct nerve analgesic effect which is an additional mechanism to treat dentinal hypersensitivity, could not be determined and therefore, the results of the present study cannot be directly implemented clinically. Other limitation of this study is small sample size which was taken. Therefore, we recommend more randomized controlled trials with larger sample size to be designed and conducted, first in-vitro and then on patients (in-vivo) to evaluate both their micro-structural effects and clinical results.
Conclusion
Based on the overall analysed results of this study, it can be concluded that:
All the three lased groups i.e., Nd:YAG, CO2 and 810-nm Diode laser showed more effective occlusion of dentinal tubular diameter than the Control group. Therefore, use of lasers can be considered as a definitive treatment modality for dentinal hypersensitivity.
Within the parameters used in this study, Nd:YAG laser was found to be most effective out of the three lasers, followed by the CO2 laser and 810-nm Diode laser was found to be the least effective in causing the dentinal tubular diameter reduction.
The morphologic changes like craters, cracks and charring effect of the dentine were seen with the use of CO2 laser.
Group I: Control group; Group II: Nd:YAG laser; Group III: CO2 laser; Group IV: Diode laser.
ANOVA Test & Turkey Post Hoc test showed significant reduction in all the lased groups
Group I: Control group; Group II: Nd:YAG laser; Group III: CO2 laser; Group IV:Diode laser [p<0.001 is highly significant].
ANOVA Test & Turkey Post Hoc test for multiple comparisons among the lased group.
Group II: Nd:YAG laser; Group III: CO2 laser; Group IV: Diode laser [p<0.001 is highly significant].