Phyllodes tumours (PT) of the breast are generally circumscribed fibroepithelial neoplasms that histologically resemble intracanalicular fibroadenoma and have unpredictable biologic behaviour. They are composed of a double-layered epithelial component surrounding hypercellular stromal component, which in combination form leaf-like papillary (phyllodes) structures. Phyllodes structures project into cleft-like cystic spaces. WHO has graded PTs into benign, borderline and malignant categories on the basis of stromal characteristics including the degree of stromal pleomorphism, mitoses, stromal overgrowth and nature of the tumour margins [1]. In benign PT the stroma is more cellular than in fibroadenoma and constitutes 60-75% of all PTs. Though rare, some studies have shown coexistence of benign PT with fibroadenoma [2] and epithelial hyperplasia, lobular and ductal neoplasia arising even within histologically benign PTs [3–7]. The aim of this study is to analyse clinicopathologic features of benign PT and to report unusual features.
Materials and Methods
This was a retrospective study, where formalin-fixed, paraffin-embedded and H&E (Haematoxylin and Eosin) stained sections from 11 cases of benign PTs of the breast diagnosed in our medical college hospital between Dec 2014 and Jan 2016 were studied. During this one year two months period total 65 cases of breast tissue were submitted to the Pathology department Inclusion criteria was all cases of histologically confirmed benign PTs including those showing intraductal proliferative lesions and invasive ductal malignancy. Benign PTs with coexistent fibroadenoma are also included in the study. Exclusion criteria was borderline and malignant PTs.
The number of microscopic slides reviewed for each case ranged from 3 to 15. At least three H&E sections of all tumours were available and were reviewed independently by two observers for verification of diagnosis. WHO histologic criteria was used for classifying PTs. A benign PT was diagnosed when the lesion showed pushing margins, mild or moderate stromal hypercellularity, mild or moderate stromal cytologic atypia, occasional mitoses that numbered up to 4/10 hpf, and no stromal overgrowth. Patient details and tumour laterality were determined from case files. Pathological findings of haemorrhage, myxoid change, gross necrosis and cystic degeneration were obtained from surgical pathology reports. Pathologic criteria used to distinguish benign PT from fibroadenoma are leaf-like pattern and increased stromal cellularity. Additional histologic changes like usual epithelial hyperplasia, the presence or absence of epithelial metaplasia, benign tubular adenoma like areas, Premalignant lesion (atypical ductal hyperplasia), Malignant lesions (DCIS, IDC), pseudoangiomatous Stromal Hyperplasia (PASH) within the tumour, histologic infarction, tumour necrosis, and haemorrhage were recorded. Coexistent fibroadenomas were also documented. Adjacent breast tissue was not available for review as all the cases were excisional biopsy specimens.
Results
Patients
The clinicopathologic features of eleven benign PT cases were analysed during one year two months study period [Table/Fig-1,2]. Their ages ranged from 13 to 45 years. The youngest patient was 13 years old. Right breast was affected in five cases and left breast was affected in six cases. Tumour size ranged from 2.5 to 18 cm. Currently all the cases are under follow up and none of them have developed recurrence.
Clinicopathologic features of benign PTs.
| S.No. | Age | Clinical Features | Laterality | Size of the Tumour |
|---|
| 1 | 25 year | Pain, lump 4 months | Right | 4 cm |
| 2 | 45 year | Pain, lump bleeding 4days | Left | 3.5cm |
| i3 | 18 year | Pain, lump 6 months | Left | 3 cm |
| 4 | 13 year | Pain & lump 8 months | Right | 5.5cm |
| 5 | 24 year | Lump 2 Months | Right | 4 cm |
| 6 | 19 year | Lump 2 Months | Left | 3.5cm |
| 7 | 17 year | Lump 2 months | Right | 4.5cm |
| 8 | 45 year | Lump 8 months | Left | 9 cm |
| 9 | 30 year | Pain, Lump 9 months | Right | 18 cm |
| 10 | 22 year | Lump 1 months | Left | 4.5 cm |
| 11 | 22 year | Lump 1 year | Left | 2.5 cm |
Gross and Microscopic Features of Benign PT.
| S.No. | Charactersticsof tumour | Case no. |
|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|
| 1 | Gross margins(Well circumscribed,Poorly circumscribed,Not mentioned) | Wellcircumscribed | Poorlycircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed | Wellcircumscribed |
| 2 | Cystic degeneration(Absent, Present,Not mentioned) | Present | Present | Absent | Absent | Absent | Absent | Absent | Present | Absent | Absent | Absent |
| 3 | Gross necrosis(Absent, Present,Not mentioned) | Absent | Present | Absent | Present | Absent | Absent | Absent | Absent | Absent | Absent | Absent |
| 4 | Gross haemorrhage(Absent, Present,Not mentioned) | Present | Absent | Present | Present | Absent | Absent | Absent | present | Absent | Absent | Absent |
| 5 | Microscopic myxoidchange (Absent,Present) | Absent | Absent | Absent | Present | Absent | Absent | Absent | Absent | present | Absent | Absent |
| 6 | Intratumoural PASH(Absent, Present) | Absent | Present | Absent | Absent | Absent | Absent | Absent | Absent | Absent | Absent | Absent |
| 7 | Microscopichaemorrhage(Absent, Present) | Present | Absent | Present | Present | Absent | Absent | Present | Present | Present | Absent | Absent |
| 8 | Infarction or necrosis(none, infarction,tumour necrosis) | Infarction | Tumournecrosis | None | Infarction | None | None | Absent | Absent | Absent | Absent | Absent |
| 9 | Epithelial hyperplasiaPresent | Absent | Present | Present | Present | Present | Present | Absent | Absent | Present(ADH) | Present(UDH) | Present(ADH)(UDH) |
| 10 | DCIS/Invasivecarcinoma | Absent | BothPresent | Absent | Absent | Absent | Absent | Absent | Absent | Absent | Absent | Absent |
| 11 | Surgical procedure(excisional biopsy,wide excision,mastectomy,unknown) | ExcisionBiopsy | Mastectomy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy | ExcisionBiopsy |
| 12 | Margin status(focal involvement,diffuse involvement,complete excision) | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision | CompleteExcision |
| 13 | Other Pathology | Fiboadenoma | Absent | Absent | Squamous & columnarmetaplasia | Absent | Tubularadenomalike-areasPresent | Absent | Absent | Absent | Absent | Absent |
Pathologic Findings
Gross and microscopic findings including unusual findings of benign PT are depicted in [Table/Fig-3,4 and 5]. Although majority of the tumours were grossly well-circumscribed, one was poorly-circumscribed and two had polypoid projection on the surface [Table/Fig-3]. Large areas of haemorrhagic infarction were seen in two cases [Table/Fig-3]. Leafy fronds characteristic of phyllodes tumour were observed in most parts of the tumour. Ipsilateral synchronous fibroadenoma was observed in one case. Epithelial component exhibited squamous metaplasia, columnar cell metaplasia, usual epithelial hyperplasia, atypical ductal hyperplasia, DCIS and IDC [Table/Fig-5]. Stromal metaplasia was not observed in any of the cases. Vascular invasion was noted in benign PT with IDC case. Surgical treatment consisted of excisional biopsy (lumpectomy) in all the cases. Surgical margins were considered complete in all the cases.
(3a) Gross photograph showing well-circumscribed benign PT (3b) Gross photograph showing well-circumscribed benign PT with finger-like/projection on the surface. (3c). Gross photograph showing large areas of haemorrhagic infarction.

(4a) Photomicro graph shows leaf-like phyllodes structures lined by double layered epithelium in a benign PT (HNE,10X). (4b) Photo shows pseudoangiomatous stromal hyperplasia (HEX40). (4c) Photo shows tubular adenoma-like areas (HNE,40X).
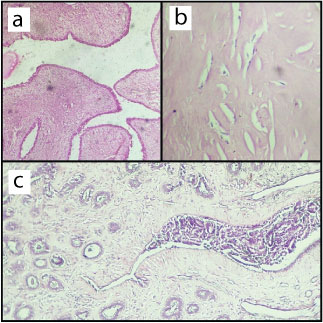
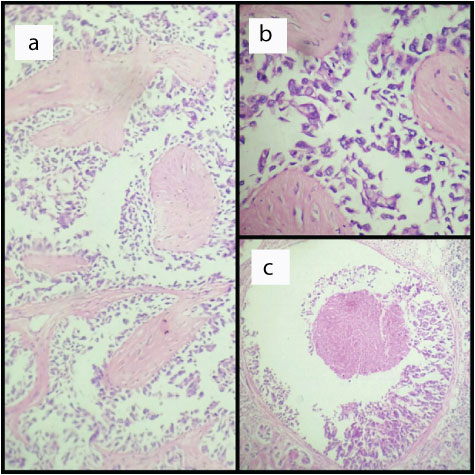
Malignant ductal cells within cystic spaces around leaf-like structures in benign PT (HNE,10X). (5b)- High power of the fig-(5a) (HNE,40X). (5c)-DCIS with comedo necrosis in benign PT (HNE,40X).
Discussion
The term “phyllodes tumour” was first used in WHO histologic classification of 1981 [8], with the prefix of benign, borderline and malignant to denote putative behaviour based on stromal histologic characteristics. Classification is still not ideal. There is difficulty in distinguishing benign PT from fibroadenoma and even benign histology can be associated with aggressive biologic behaviour. Recent evidence indicates that benign PT may progress to malignancy not only in the stromal direction, but also in the epithelial direction [9]. Also, an indeterminate category of “benign fibroepithelial neoplasm” has been described, which histologically do not fit into the category of fibroadenoma or benign phyllodes tumour. Periductal stromal tumour is another rare lesion that may progress to PT. It has low grade sarcomatous behaviour and both are considered part of the same spectrum of disease. But it is non-circumscribed and does not show leaf-like processes [10]. There are some overlapping histologic features among these fibroepithelial lesions and there is a tendency for progression to malignant phenotype. But given the significant differences in their clinical behaviour, complete excision of such indeterminate or synchronous fibroepithelial lesions on needle biopsies may be needed, along with appropriate clinical correlation for accurate pathologic classification [11].
In western countries PTs account for 0.3-1% of all primary tumours of the breast. They mostly occur in 40-50 years age group. In Asian countries PTs may occur in 25-30 years age group and account for a higher proportion of primary breast tumours as observed in this study [2]. Clinical features of PT include unilateral, firm, painless breast mass, not attached to the skin. Average size is 4-5 cm, but with mammographic screening 2-3 cm in diameter tumors are becoming more common. Very large tumours may stretch the skin, but ulceration is rare. Bloody nipple discharge caused by spontaneous infarction of the tumour may be seen [1,12], as noted in two cases.
Benign PTs are well-circumscribed firm, bulging masses. The cut surface is tan or pink to grey in color and may be mucoid and fleshy. The characteristic whorled pattern with curved clefts resembling leaf buds is best seen in larger lesions. But smaller lesions may have a homogeneous appearance. Haemorrhage and infarction may be present in large lesions as noted in two cases. Histologically benign PT may show stromal heterogeneity like peri-epithelial or subepithelial accentuation of stromal cellularity, uncommonly hyalinization and myxoid change. Benign lipomatous, cartilaginous and osseous metaplasia of stroma may be seen. It is reported that both benign and malignant PTs may harbor DCIS, invasive ductal and lobular neoplasia [3,9]. Interestingly epithelial component of benign PT showed a range of hyperplastic, metaplastic, dysplastic and neoplastic changes (tubular adenoma like areas, DCIS & IDC) in this study. Benign PT has pushing margin, but small tumour buds may protrude into the surrounding tissue as seen in two cases. Such tumour protrusions are a source of recurrence if they are not completely removed [1].
Clonality studies have suggested that stromal cells are monoclonal and epithelial cells are polyclonal [13]. So phyllodes tumours were considered earlier mainly as stromal neoplasms, where stroma can progress to malignancy. It was also considered that benign PT possibly arises from fibroadenomas. This hypothesis has been challenged. More recent studies [14,15] have demonstrated oncogenic mutations in both epithelium and stroma, which suggests that both epithelium and stroma can undergo neoplastic changes. There is also initial interdependence or cross-talk between the two components. In addition to epithelial-stromal cross-talk via epithelial Wnt signalling and stromal insulin growth factors and beta-catenin pathway, there is inverse correlation between epithelial and stromal overexpression for various biological markers like estrogen receptor & p53, c-kit, Ki-67, endothelin-1, epidermal growth factor receptor, heparan sulfate. This suggests an initial epithelial-stromal interdependence at the benign phase. Upon malignant progression, the stroma is postulated to assume an autonomous growth overriding any epithelial influence. Frequent genetic alterations are chromosomal gains of 1q and losses at chromosome 13. Immunohistochemical, cytogenetic and molecular studies have detected that acquisition of new mutations creates different subclones in histologically benign PT, which contributes to its unpredictable clinical behaviour [14,15].
Several studies have described progression of fibroadenoma to phyllodes tumour [13,16,17]. Kuijper et al., have documented that fibroadenoma not only progresses in a stromal direction to phyllodes tumour, but also progresses in an epithelial direction towards carcinoma in situ [16]. Because benign PTs can co-exist with fibroadenoma and ductal and lobular neoplasia can arise in benign PT, adequate macroscopic sampling is required for excision specimens to detect these synchronous and progressing tumours. Till date, clinicopathologic and molecular studies involving p53, Ki-67, c-kit, CD34 and actin have not helped much in predicting clinical outcome. Grading and prognostication of PT based on histomorphologic findings may not predict clinical outcome. Currently, wide resection with 1 cm margin is the treatment of choice for PT. Wide resection improves prognosis, regardless of the histologic classification [18].
Conclusion
This study shows a spectrum of proliferative changes like hyperplastic, metaplastic, dysplastic, benign, in-situ-malignancy and even invasive ductal malignancy occurring in epithelial component of benign PTs. So adequate and extensive sampling is necessary for correct diagnosis of malignant progression in benign PT and its management. As this study includes smaller number of cases, future studies including large number of cases or multi-institutional studies are needed to understand the malignant potential of its epithelial component.