The oral cavity is an uncommon habitat which bestows an optimal medium for bacterial proliferation. Aerosols originated during the usage of ultrasonic scaler or air rotor of dental chair have droplet nuclei particles which linger in the surrounding for a long period of time and is a peril factor for evolving contagious diseases for the patient as well as the dental experts.
In the last 15 years, bounteous investigations have demonstrated that antimicrobial solutions when used as pre-procedural rinses can decline the number of microorganisms aerosolized during clinical practice.
The cationic nature of CHX decreases absorption through skin, mucosa and gastrointestinal tract because of which it exhibits very less toxicity. Systemic toxicity from topical application or ingestion is therefore not proclaimed, nor is there any substantiation of teratogenecity in the animal model. Chlorhexidine is fairly tolerated without any stern emanations in humans and animals when intravenous infusion was done [3].
As reported by Kotsilkov, allergic sensitization to PVP is unlikely, only 0.73% of 600 patients displayed a sensitization reaction in a skin patch test [2,4]. However, PVP should not be rendered to individuals who are allergic to iodine, suffering from thyroid dysfunction or are pregnant or nursing [2,4].
The aim of this study was to evaluate the effect of povidone iodine and chlorhexidine gluconate as an ultrasonic liquid coolant on aerosols in comparison with distilled water.
Materials and Methods
This was a comparative study in which 30 patients of both gender (17 males and 13 females) within the age range of 22-55 years were selected. The sample size determination was done after consulting a biostatistician. The subjects for this study were selected from the outpatient Department of Periodontics, MIDSR Dental College, Latur, Maharashtra, India. The duration of the study was from July 2015 to October 2015. This study was done under the ethical guidelines of the Institutional Research and Ethical Committee. Participants who met the inclusion criteria were informed about the purpose of the study and each patient was provided with an informed consent, after explaining the nature and possible risk. Criteria for participation included patients having a minimum of 20 permanent functional teeth. Subjects with mean probing depth ≤ 5mm and clinical attachment loss ≤ 3mm measured with Williams Periodontal Probe (Hu-Friedy) in at least 30% teeth sites were included [5].
Subjects with a history of systemic diseases like diabetes mellitus, hypertension, rheumatoid arthritis, etc., use of tobacco in any form, history of periodontal treatment in the previous six months, pregnant and lactating females, patients with thyroid dysfunction, usage of antibiotic or other drugs that affect periodontal status in the past six months and patients allergic to chlorhexidine and povidone iodine were excluded from study.
Oral examination was carried out by measuring clinical parameters such as Probing Pocket Depth (PPD), Clinical Attachment Loss (CAL), Plaque Index (PI) and Gingival Index (GI) in patients with chronic periodontitis [6,7]. All subjects were assigned to one of the three groups by using randomization table and consisted of 10 subjects in each group depending on different ultrasonic liquid coolants.
Group 1 (Control group): Ultrasonic scaling with distilled water (10 subjects).
Group 2 (Test group): Ultrasonic scaling with 2% povidone iodine in 0.1% dilution [8,9] (10 subjects) 2% povidone iodine is diluted in 1:1 ratio in 1 liter water to prepare ultrasonic liquid coolant.
Group 3 (Test group): Ultrasonic scaling with 0.12% chlorhexidine in 0.06% dilution [10] (10 subjects) 0.12% chlorhexidine gluconate is diluted in 1:1 ratio in 1 litre water to prepare ultrasonic liquid coolant.
Study Design
The closed dental operatory was fumigated for 48 hours before the procedure to prevent contamination.
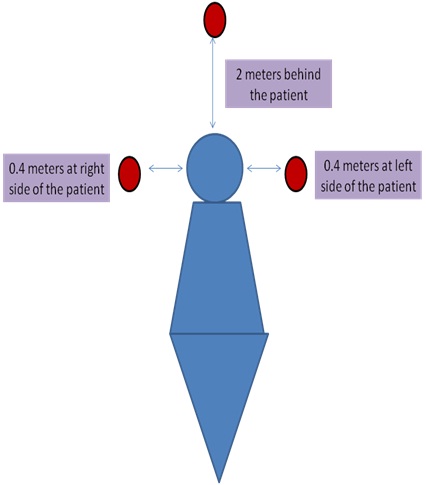
At the baseline, one blood agar plate was kept for 10 minutes in the fumigated closed chamber before ultrasonic scaling [Table/Fig-1]. Patients were made comfortable in dental chair. Three blood agar plates were kept at a distance of 0.4 meters away on either side of the patient and 2 meters behind the patient’s mouth during ultrasonic scaling [11,12] [Table/Fig-2]. The patients ultrasonic scaling was executed for 20 min by the clinician, with universal tip attached to the ultrasonic scaler. The normal rate of flow of water in ultrasonic scaler is 20-30ml/min. The same rate of flow of water for each agent, while performing ultrasonic scaling was maintained. To assure that the room was free from aerosols, only one patient was treated per day. For every scaling procedure, high vacuum suction was used. After the treatment, three coded blood agar plates were left uncovered for 20 min at the pre-designated sites for gravitometric settling of airborne bacteria. After gravitometric settling of aerosols, blood agar plates were transferred to laboratory for incubation at 37°C for 48 hours [Table/Fig-3] followed by colony counting procedure with the help of colony counter device by the microbiologist.
Baseline blood agar plate after fumigation.

Positions of blood agar plates in the fumigated dental operatory.
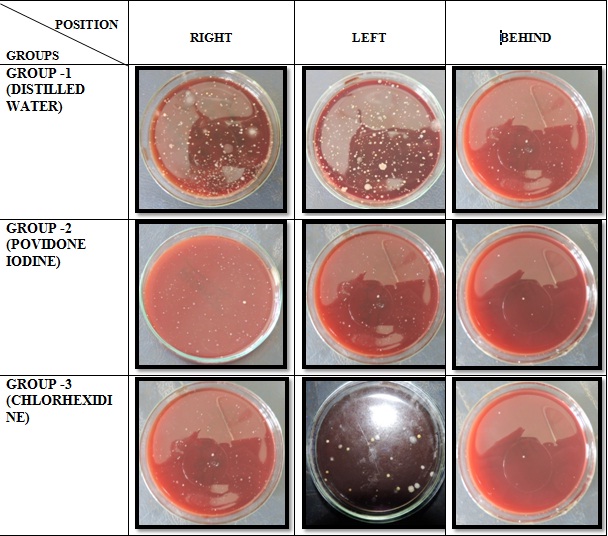
Blood agar plates at right, left and behind patient’s mouth respectively in Group 1, 2 and 3.
Statistical Analysis
For determination of overall inference, one way-ANOVA test was performed. Tukey’s Post hoc test was applied for analyzing intergroup comparison of CFU.
Results
In this study, 30 patients were selected and were randomly divided into distilled water, povidone iodine and chlorhexidine groups; each group consisted of 10 subjects. The clinical parameters were recorded to confirm diagnosis of chronic periodontitis.
The mean colony counts on all sides in Group 1, Group 2 and Group 3 were compared in [Table/Fig-4]. This indicates that Group 3 (chlorhexidine gluconate) had effective CFU reduction (27.17 ± 12.5 CFU) when compared to distilled water (124.5 ± 30.08 CFU) and povidone iodine (60.43 ± 33.33 CFU). On applying one way-ANOVA test, the ‘F’ ratio obtained was 81.3 with p value 0.001 which was statistically significant. These results can be attributed to the antiseptic and antimicrobial properties of chlorhexidine. The comparison of mean CFU on right side in Group 1, Group 2, Group 3 (165.3 ±18.47, 100.6 ± 6.43, 41.3 ± 4.5) respectively showed statistically significant (p-value is 0.001) results as demonstrated in [Table/Fig-5].
Comparison of mean colony count on all sides among different groups.
| Sr. No. | Groups | Colony Count | F ratio | p-value | Significance |
|---|
| Mean | SD |
|---|
| 1. | Group 1 (Distilled Water) | 124.5 | 30.08 | 81.3 | 0.001* | Significant |
| 2. | Group 2 (Povidone Iodine) | 60.43 | 33.33 |
| 3. | Group 3 (Chlorhexidine) | 27.17 | 12.5 |
Mean comparison among study groups using ANOVA one way test.
*p <0.05 Statistically significant
Comparison of mean colony count on right side among different groups.
| Sr. No. | Groups | Colony Count | F ratio | p-value | Significance |
|---|
| Mean | SD |
|---|
| 1. | Group 1 (Distilled Water) | 165.3 | 18.47 | 286.5 | 0.001* | Significant |
| 2. | Group 2 (Povidone Iodine) | 100.6 | 6.43 |
| 3. | Group 3 (Chlorhexidine) | 41.3 | 4.5 |
Mean comparison among study groups using ANOVA one way test.
*p <0.05 Statistically significant
Tukey’s Post hoc test was performed for intergroup comparison in Group 1, 2 and 3. Comparing the p values between the groups, that is, Group 1 and 2 (p-value 0.01), Group 1 and Group 3 (p-value 0.01) and Group 2 and 3 (p-value 0.01) were all statistically significant [Table/Fig-6].
Comparison of mean colony count on all sides among different groups by tukey’s post hoc test.
| Sr. No. | Groups | p-value | Significance |
|---|
| 1. | Group 1 vs. Group 2 | 0.01* | Significant |
| 2. | Group 1 vs. Group 3 | 0.01* | Significant |
| 3. | Group 2 vs. Group 3 | 0.01* | Significant |
Multiple comparison done using Tukey’s Post hoc test
*p < 0.05 Statistically significant
The comparison of mean colony counts on right, left and back side in Groups 1, 2 and 3 are depicted in [Table/Fig-7]. It showed highest CFU in Group 1 right, left and behind positions 165.3 ± 18.47, 128.7 ±11.1, 79.5 ± 9.42 CFU respectively, followed by Group 2: 100.6 ± 6.43, 59.1 ± 4.72, 21.5 ± 4.7 respectively and in Group 3: 41.3 ± 4.5, 27.7 ± 3.86, 12.5 ± 2.51 respectively.
Comparison of mean colony count among different positions.
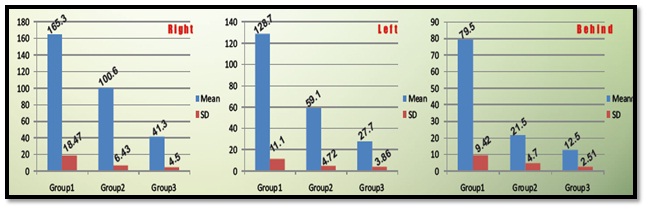
The mean colony counts of Groups 2 and 3 at right, left and back positions are 100.6 and 41.3, 59.1 and 27.7, 21.5 and 12.5 respectively. Group 3 showed better CFU reduction when compared to Group 2.
Discussion
Periodontal disease is a multifactorial, microbially initiated and chronic inflammatory disease which results in the tissue destruction of the supporting apparatus of the dentition. The risk factors for periodontal disease represent a particular aspect of response to the environment that may be associated with periodontal disease, the combination of which may or may not be causal. Some risk factors are variable while others are not. Dental plaque is the prime harbor for various oral microorganisms. Disruption of dental plaque is necessary which can be done by using various mechanical devices. However, the total eradication of plaque and calculus is difficult to gain. Incomplete eradication of microbes and its by-products could eventually cause the proliferation of microorganisms.
In dental practice, various dental procedures like ultrasonic scaling, crown preparation, caries excavation, etc., cause production of aerosols which may contain potentially infectious blood borne and airborne pathogens [13].
There are methods to control airborne contamination produced by various dental procedures such as barrier protection (mask, gloves and eye protection), pre-procedural rinse with antiseptic mouthwash such as chlorhexidine, high-volume evacuator, high-efficiency particulate air room filters and ultraviolet treatment of ventilation system [14].
Barrier protections are a part of standard precaution and it is inexpensive but mask will only filter out 60%-95% of aerosols. Ill fitting of mask can cause leakage [14].
Preprocedural rinsing is suggested to be most effectual on planktonic microorganisms. It will not influence biofilm microbes such as plaque, subgingival microorganisms, blood from the surgical site or nasopharyngeal organisms [14].
It is well proven and accepted fact that pre-procedural rinse with chlorhexidine and povidone iodine will reduce the bacterial count but the depth of pocket penetration is less than 2 mm [15–17].
The average length of universal ultrasonic scaler tip is 7mm. The water coolant of the ultrasonic unit does extend apically as far as the probe tip thereby providing coolant at the tip of the instrument [18].
There is need for use of chemical agents as an adjunct to reduce the contamination from dental aerosols. Chlorhexidine has antimicrobial property which is attributed to its action on the inner cytoplasmic membrane. Due to its broad spectrum antimicrobial activity and good substantivity it is recommended as a gold standard for plaque control [19].
Iodine is a non-metallic essential nutrient with a persuasive wide range of microbicidal actions against almost all of the imperative health-related microorganisms, including bacteria, fungi, viruses and protozoa. Since povidone slowly and continuously releases free iodine into solution, these qualities help to maintain antimicrobial competence for an extensive duration and to decline toxicity [20].
Based on these facts, we have designed our study in which chlorhexidine and povidone iodine were used as ultrasonic liquid coolant and not as pre-procedural rinse.
The American Dental Association has suggested potential contaminated aerosols or splatter can be controlled during dental procedures [14].
The long term inhalation of chlorhexidine and povidone iodine will not affect the operators health because as studies have proven that aerosols linger only till 30 min [21–25] and CHX and PVP iodine are used in solution form and in low concentration in our study.
There have been no definitive epidemiologic studies that have linked the correlation of dental aerosols to different ultrasonic liquid coolants, the cloud of contaminated aerosols and splatter such as that created by an ultrasonic scaler and its concern to the dental professionals. Our study demonstrates that a sufficient amount of aerosols and splatter from the patient were ejected at different radius and at different positions.
In conducting this study, an attempt was made to evaluate and compare the ability of different ultrasonic liquid coolants to lower the microbial counts in aerosols produced due to ultrasonic scaler.
The highest CFU reductions were shown in Group 3 (chlorhexidine gluconate) when compared to povidone iodine. These results are in accordance with the study done by Kaur et al., who has also found that chlorhexidine is better than povidone iodine and ozone when used as pre-procedural rinse on micro-organisms in dental aerosols [12].
Sahrmann concluded that bacteremia was reduced but not totally eliminated after subgingival instrumentation with concomitant povidone iodine rinsing. Hence, povidone iodine can be suggested as an ultrasonic liquid coolant [26].
Muir et al., found that a 2min pre-rinse with CHX significantly decreased aerosols produced by ultrasonic scalers [27].
CHX pre-procedural rinse with the use of air polisher was effective in decreasing bacterial aerosols contamination [28].
Rahn et al., chose PVP-iodine at a concentration of 10% as an antiseptic agent, as it has been recommended as a first choice solution to reduce oral pathogens by mouthwash or rinsing due to a quicker and more pronounced bactericidal effect compared to 0.2% chlorhexidine, the most popular antiseptic agents in dentistry [29].
The CFU were maximum on right side and these results can be absolved as the operator included in this study was right handed and the patients were asked to tilt his/her face towards operator’s side.
Proper protective barriers such as face mask, eyewear, head caps, high vacuum suction were used during ultrasonic scaling for every patient to avoid spillage of the these agents into eyes of operator or doctor. If the agent is spilled into eyes then thorough washing of eyes with water is recommended.
The newer facts in the study were
In this study, the antimicrobial agents were used in less concentration than pre procedural rinse and oral irrigations.
Chlorhexidine and povidone iodine when used as ultrasonic liquid coolant instead of distilled water can cause less contamination of waterlines.
Advantages of using these agents as coolant were
Dental aerosol contamination during various dental procedures such as root canal treatment, scaling, caries excavation etc., will also be reduced.
Depth of penetration of ultrasonic liquid coolant in periodontal pocket will be increased.
Disadvantage of using these agents as coolant were
Some subjects might complain of unpleasant taste.
Limitation
Qualitative estimation of bacterial aerosols could have been carried out.
Future Studies
The heat transfer to the tooth during scaling may affect the chemical agent. Further studies should be carried out to study the effect of dilution and heat transfer during ultrasonic scaling.
Further studies can be conducted comparing plaque index and gingival index scores before and after treatment.
Left handed operators can be included along with right handed operators for future studies.
Further studies can be carried out with a larger sample size.
Conclusion
This study indicates that chlorhexidine gluconate as an ultrasonic liquid coolant significantly reduces the microbial content of dental aerosols generated during scaling when compared with distilled water. Chlorhexidine gluconate showed better CFU reductions when compared with povidone iodine. Povidone iodine also showed better CFU reduction when compared with distilled water. Hence, povidone iodine can also be used as an ultrasonic liquid coolant for reducing the number of dental aerosols during ultrasonic scaling.
Mean comparison among study groups using ANOVA one way test.
*p <0.05 Statistically significant
Mean comparison among study groups using ANOVA one way test.
*p <0.05 Statistically significant
Multiple comparison done using Tukey’s Post hoc test
*p < 0.05 Statistically significant