Congenital Aniridia with Ectopia Lentis
Rakhi Kusumesh1, Anita Ambastha2
1 Associate Professor, Department of Cornea and Refractive Services, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
2 Assistant Professor, Department of Community Ophthalmolgy, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rakhi Kusumesh, Associate Professor, Cornea and Refractive Services, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
E-mail: drkrakhi@yahoo.com
Foveal hypoplasia, Iris Hypoplasia, PAX6 gene, Subluxated lens, WAGR syndrome
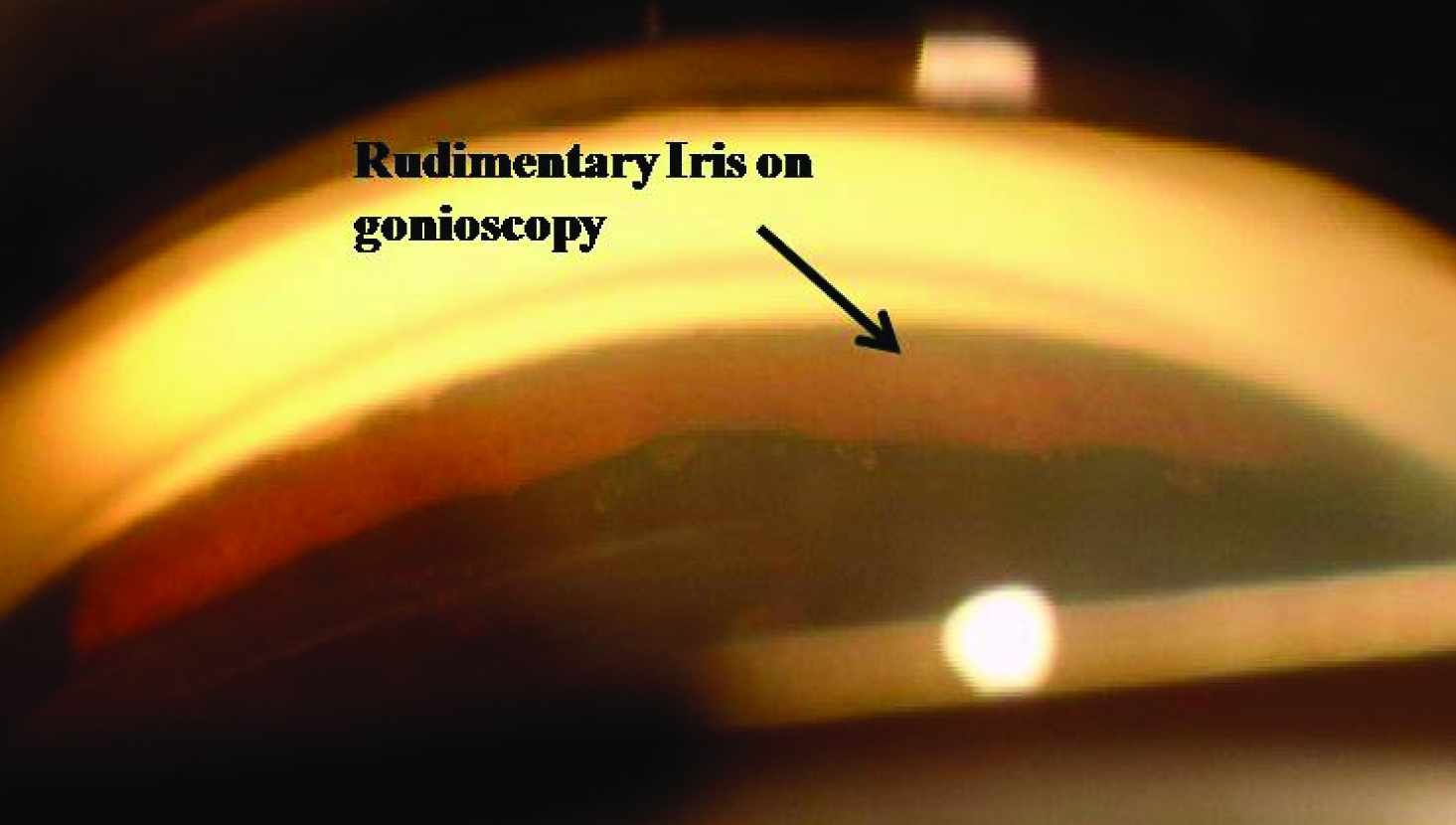
A 13-year-old male presented with complaints of gradual diminution of vision and photophobia in both eyes since early childhood. He had history of recurrent falls and difficulty in reading. Family history was noncontributory. Best corrected visual acuity at the time of presentation was 6/60 in both eyes. Anterior segment examination revealed total aniridia [Table/Fig-1a] and superiorly subluxated lens with broken and stretched zonules [Table/Fig-1b]. On gonioscopy, rudimentary iris tissue was present [Table/Fig-2]. Fundus examination showed absent foveal reflex. A diagnosis of bilateral congenital aniridia with ectopia lentis with foveal hypoplasia was made and lens extraction with transscleral fixation of intraocular lens in right eye followed by left eye was performed. Postoperative best corrected visual acuity at 1 week was 6/36 in right eye with marked decrease in photophobia.
(a) Congenital aniridia shows near total absence of iris with superior subluxation of lens; and (b) stretched and broken zonules on retroillumination.
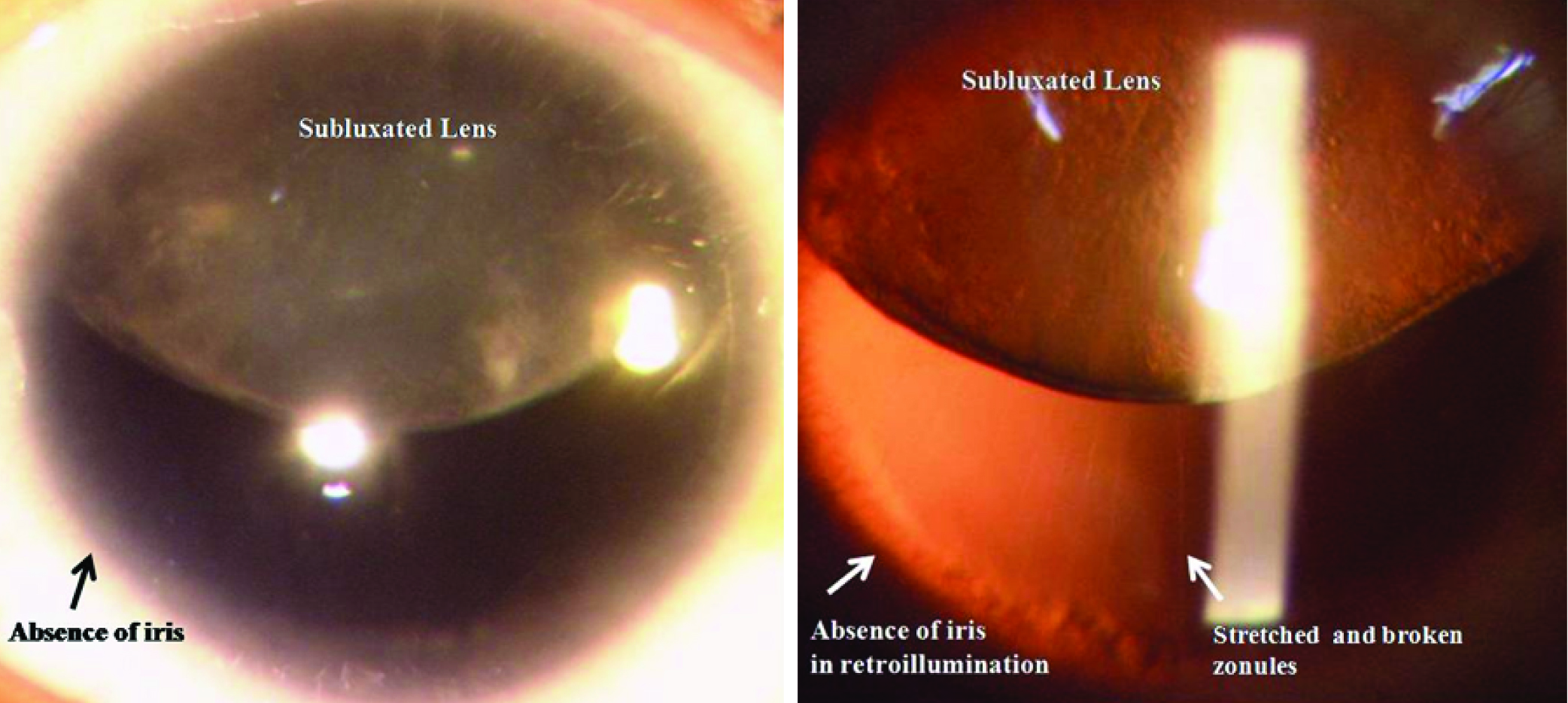
Figure shows rudimentary iris on gonioscopy.
Discussion
Aniridia is a rare congenital disorder, characterized by profound hypoplasia of the iris, in association with multiple ocular anomalies such as ectopia lentis, corneal defects, glaucoma, strabismus and optic nerve hypoplasia [1–3], which can lead to glare, photophobia and other visual disturbances. This condition may be associated with systemic defects consisting of mental retardation, genital anomalies, and Wilms’ tumour (WAGR syndrome) [1]. Two-third cases of aniridia occur as an isolated ocular malformation with autosomal dominant inheritance, which is caused by a mutation in the PAX6 (paired box gene family) gene and remainders are sporadic, which occurs due to de novo deletions on chromosome 11p13 involving the PAX6 gene [1]. Larger deletions affecting the adjacent WT1 (Wilm’s tumour) genes are the underlying cause of the WAGR syndrome [1,2]. Gene expression associated with PAX6 is regulated by both paternal and maternal alleles may result in phenotypic variation even in cases with the same PAX6 genotype [4]. Because there is considerable phenotypic variability, the clinician must perform a careful slit-lamp examination on other family members [4].
As far as treatment options for ocular diseases are concerned in aniridia, implantation of artificial iris implants or colored iris diaphragm intraocular lens following cataract surgery improve postoperative outcomes by reducing glare disability and improving visual acuity [5,6]. Spectrums of corneal diseases are treated with artificial tears and autologus serum drops to limbal stem cell transplantation with or without sequential keratoplasty [7]. Additionally, these patients are always at high risk for developing glaucoma. Thus, all patients with aniridia should undergo periodic glaucoma screening throughout life including intraocular pressure recording, gonioscopy and visual fields. Management of aniridic glaucoma includes antiglaucoma medications, trabeculectomy and glaucoma drainage devices [1].
Despite many ocular problems, most aniridia patients can retain useful vision with appropriate and timely ophthalmic care. Therefore, every medical personnel besides ophthalmologist should be able to detect the disease at an early stage and proper genetic counseling should be obtained.
[1]. Nelson LB, Spaeth GL, Nowinski TS, Margo CE, Jackson L, Aniridia. A reviewSurv Ophthalmol 1984 28(6):621-42. [Google Scholar]
[2]. Käsmann-Kellner B, Seitz B, Aniridia syndrome: clinical findings, problematic courses and suggestions for optimization of care (“aniridia guide”)Ophthalmologe 2014 111(12):1145-56. [Google Scholar]
[3]. Jusufovic V, Cabric E, Popovic-Beganovic A, Musanovic Z, Zvornicanin J, Treatment of congenital aniridia associated with subluxated infantile cataractMed Arh 2014 68(3):212-14. [Google Scholar]
[4]. Yokoi T, Nishina S, Fukami M, Ogata T, Hosono K, Hotta Y, Genotype-phenotype correlation of PAX6 gene mutations in aniridiaHum Genome Var 2016 3:15052 [Google Scholar]
[5]. Qiu X, Ji Y, Zheng T, Lu Y, The efficacy and complications of black diaphragm intra-ocular lens implantation in patients with congenital aniridiaActa Ophthalmol 2015 [Google Scholar]
[6]. Rickmann A, Szurman P, Januschowski K, Waizel M, Spitzer MS, Boden KT, Long-term results after artificial iris implantation in patients with aniridiaGraefes Arch Clin Exp. Ophthalmol 2016 254(7):1419-24. [Google Scholar]
[7]. Shiple D, Finklea B, Lauderdale JD, Netland PA, Keratopathy, cataract, and dry eye in a survey of aniridia subjectsClin Ophthalmol 2015 9:291-95. [Google Scholar]