Tooth extraction is one of the most common procedures practiced since beginning of civilization. It is the only dental procedure which was carried out by dentists in the previous centuries and various instruments have evolved for this procedure over time. In 14th century, Guy de Chauliac invented the dental pelican, which was used through the late 18th century [1]. The pelican was replaced by the dental key which, in turn, was replaced by tooth extraction forceps in the 20th century. Conventional tooth extraction forceps is metallic instrument with two beaks to grasp crown of tooth, with a hinge in centre and handle, which is widely used in recent times.
However tooth extraction is a traumatic procedure that results in immediate destruction and loss of surrounding alveolar bone and soft tissues [2]. The instrument selection and the technique used for extraction significantly affects the amount of paradental tissue loss. There has also been an increased interest in atraumatic tooth extraction in order to maintain bone for future implant insertion in the past decade. Marginal alveolar bone ridge protection has influence in achieving optimal functional, aesthetic and orthodontic treatment results. So, newer instruments and techniques for extraction were developed for minimizing trauma to paradental structures over the period of time. These instruments include Periotomes, Powered Periotomes, Physics Forceps, Benex extractor and many other which assist the surgeon to perform extractions more predictably, atrumatically and with minimum discomfort to patient [3,4]. The Physics forceps were developed by Golden Dental Solutions, Michigan which is based on the biomechanical principles of a first-class lever, creep and stress distribution without the squeezing, grasping, twisting and pulling forces to perform atrumatic extraction [5]. Conventional forceps work by forces placed equally on the facial and lingual portion of the tooth and elevating it out of the socket by movement of the operator’s arm and wrist. This pulling force technique invites unnecessary complications including fracture of roots, bone and loss of tissue [6].
The aim of the present study was to evaluate the efficacy of physics forceps in premolar teeth extraction for orthodontic purpose and compare it to conventional forceps in terms of time taken for extraction, amount of bone and soft tissue loss, ability to perform complete extraction, measuring postoperative pain and occurrence of complications.
Materials and Methods
Eleven patients were included in this prospective study who reported to Department of Oral and Maxillofacial surgery during December 2014 to May 2015, requiring bilateral extractions of upper and lower premolars for orthodontic treatment purpose and consenting for the study. Total 42 extractions (all four first premolars in 10 patients and two second premolars in one patient) were done. In every patient decision of extraction of tooth with particular forceps system (conventional or Physics) was done by tossing a coin for the first extraction followed by alternate use of other system. Thus, 21 extractions were done by using each forceps system.
Every patient underwent an adequate pre-surgical preparation consisting of detailed case history, blood tests wherever indicated and radiographic examination (OPG or IOPA of tooth to be extracted). Patients with absolute contraindication for extraction and with mobile/carious/malaligned teeth to be extracted or teeth indicated for transosseous extraction were not included in study.
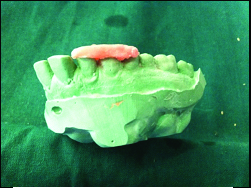
Alginate impression was taken of the dental arch in which extraction was to be carried out. A dental plaster cast was made from the impression. A self cure acrylic template covering the occlusal 1/3rd surface of tooth to be extracted and one tooth on either side was made over the prepared cast [Table/Fig-1].
Extractions were done following standard aseptic surgical protocols. Local anaesthesia containing 1:80,000 Lignocaine Hydrochloride & adrenaline (Lignoter, Lusture Pharma, Ahemdabad, India) was used to give regional nerve block along with local infiltration in every extraction using 26 gauge disposable syringe (Unolok, Hindustan syringes, Faridabad, India).
Acrylic template was then placed intra orally over the teeth and was used as the reference point. A Williams periodontal probe was used for measuring the distance between gingival margin and the lower edge of template, which suggested pre extraction gingival level (Peg) [Table/Fig-2a]. The probe was then inserted deep into the gingival margin to measure the distance between the edge of template and the marginal bone, which showed the pre extraction bone level (Peb) [Table/Fig-2b]. Peg and Peb were measured at three different points on mesial 1/3rd, middle 1/3rd and distal 1/3rd on the buccal side of tooth to be extracted and values were recorded.
(a) Measurement of Pre extraction gingival level (Tip of probe placed over gingival margin). (b) Measurement of Pre extraction Bone level (Tip of probe placed into gingival suclus on bone margin).

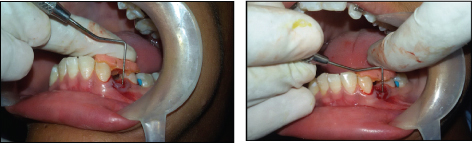
Mucoperiosteal flap reflection using periosteal elevator was only done in extractions which were to be carried out using conventional forceps. Elevators were not used for luxation of tooth to be extracted. Tooth specific forceps were used for extraction of specific tooth in conventional forceps system. The beaks of conventional forceps were placed at the cemntoenamal junction of particular tooth and it was extracted giving tooth specific movements [Table/Fig-3b]. The beak of Physics forceps was placed on lingual/palatal aspect of tooth at or below Cementoenamal Junction (CEJ) and bumper was placed on buccal alveolar ridge at mucogingival junction and constant controlled traction force was given until tooth was displaced out of the socket [Table/Fig-3b].
(a) Conventional forceps engaged over tooth. (b) Physics forceps engaged over tooth.

Time taken for extraction was considered from the point of application of the beaks on the tooth to the delivery of tooth out of socket, measured using stop watch and recorded in seconds (sec). Compression of socket was not done following the extractions. Extracted tooth was clinically examined for root fracture and adherence of buccal plate to the root and recorded.
Following the extraction the template was again placed over the teeth and distance between the marginal gingiva and lower edge of template was measured which showed Post Extraction Gingival level (Pog) [Table/Fig-3c]. Post Extraction Bone level (Pob) was measured by placing the probe into extracted socket and feeling the bone margin, distance was measured from the edge of the template [Table/Fig-3d].
(c) Measurement of post extraction gingival level (Tip of probe placed on gingival margin). (d) Measurement of post extraction bone level (Tip of probe placed over bone margin).
The mean value of pre extraction and post extraction level at three points was then calculated and the difference between these two values suggested the amount of marginal gingiva and bone loss.
The extraction was given success score based on the criteria given by Choi et al., [7]:
Complete success (Score 5): extraction without crown and root fracture.
Limited success with root tip fracture (Score 4): extraction involving root tip fracture.
Limited success with root fracture (Score 3): extraction involving root one or more root fracture or crown fracture.
Limited success with osteotomy (Score 2): fracture-free extraction and partial osteotomy in case divergent roots and thick cortical bone was present.
Failure (Score 1): Failure to extract.
Betadine soaked gauze pressure pack were placed over the extraction socket and similar post extraction instructions were given to all the patients.
All the patients were prescribed following medications:
Cap. Amoxicillin 500mg (TID)-3days
Tab. Diclofenec Sodium 50mg (BD)-3 days
Tab. Ranitidine 150mg (BD)-3days
Patients were followed up for postoperative pain evaluation on VAS scale on 1st and 3rd post op day. Any other complications were also recorded on 3rd post op day.
Statastical Analysis
The collected data was tabulated and analysed using SPSS v 22. Descriptive statistics was used to infer the mean SD of socio-demographic data. Unpaired Student t-test was used for probability measurements.
Results
This split mouth study included 11 patients, 7 males and 4 females with mean age of 19.4 years and age range was 14-23 years. Total 42 premolar extractions were included in the study. Ten patients underwent extractions of all 4 first premolars while 1 patient underwent bilateral extraction of upper second premolars.
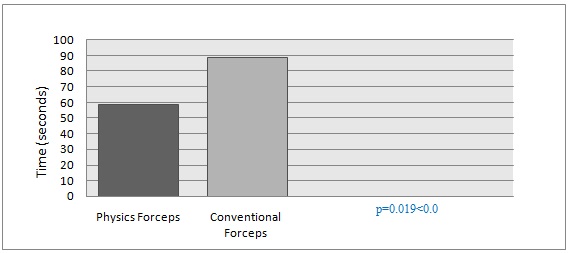
Extraction time: The mean time taken for extraction using Physics forceps was 58.8 (±48.13) sec while that with conventional forceps were 88.33 (±37.59) sec. When subjected to student t-test this difference was found statistically significant with p=0.019<0.05 [Table/Fig-4].
Mean extraction time using physics forceps and conventional forceps.
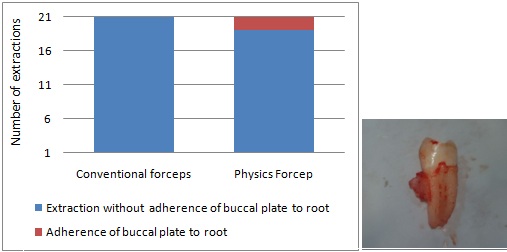
Root and buccal cortical plate fracture: Root tip fracture occurred in 2 teeth (4.76%) extracted using conventional forceps which was not seen in extractions done with physics forceps. Fracture of buccal cortical plate which remained adhered to roots of extracted teeth was found in 2 teeth (4.76%) extracted using physics forceps [Table/Fig-5a&b].
Occurrence of root fracture using physics forceps and conventional forceps.
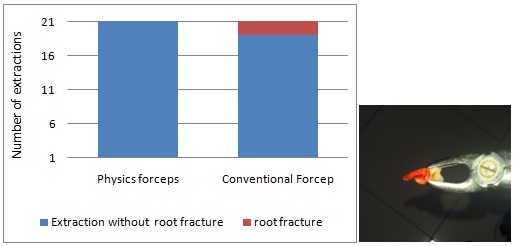
Fracture of buccal cortical plate and its adherence with the root.
Success score of extraction: In the study, out of total of 42 extractions complete success (Score 4) was found in 40 extractions (96.34%) and limited success with root tip fracture (Score 3) was found in 2 extractions (4.76%) done using conventional forceps. Mean success score of extraction using physics forcep was 4 and using conventional forcep was 3.9 [Table/Fig-6].
Success score of extraction using physics forceps and conventional forceps.
| Extraction System | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 | Mean Score |
|---|
| Physics Forceps | 0 | 0 | 0 | 0 | 21 | 4 |
| Conventional Forceps | 0 | 0 | 0 | 2 | 19 | 3.9 |
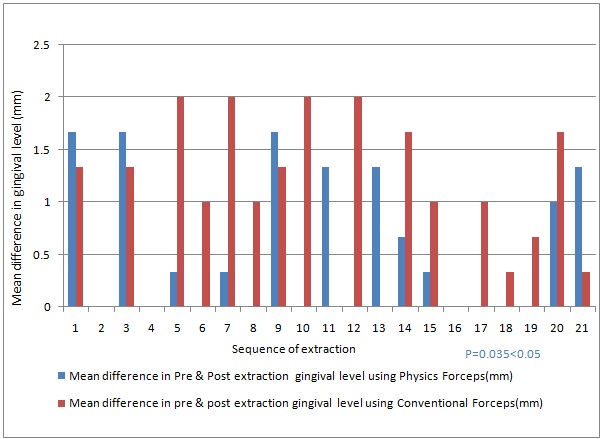
Gingival and Marginal bone loss: The mean difference in the pre and post extraction gingival level using physics forceps and conventional forceps was 0.57mm (±0.65) and 1.01mm (±0.75) respectively. The difference between these values was statistically significant p=0.035 [Table/Fig-7].
Graphical comparison of changes in gingival level using physics forceps and conventional forceps.
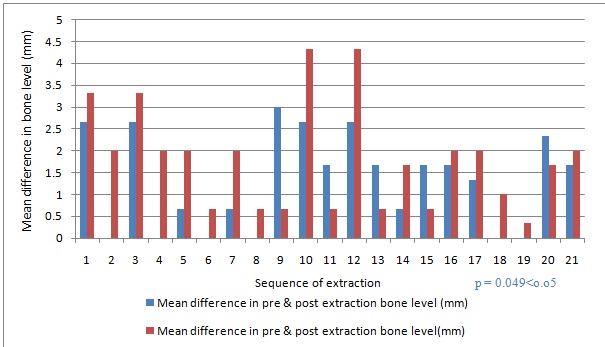
The mean difference in the pre and post extraction bone level using physics forceps and conventional forceps was 1.26mm (±1.08) and 1.87mm (±1.13) respectively which was statistically significant p=0.037 [Table/Fig-8].
Graphical comparison of changes in marginal bone level using physics forceps and conventional forceps.
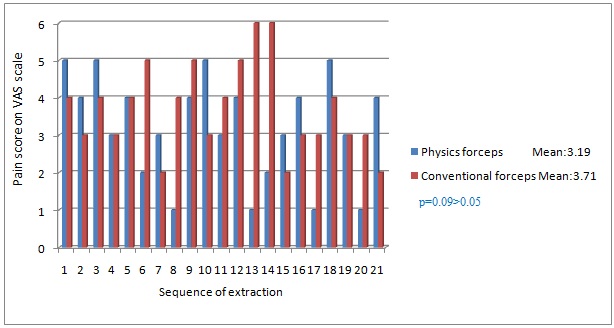
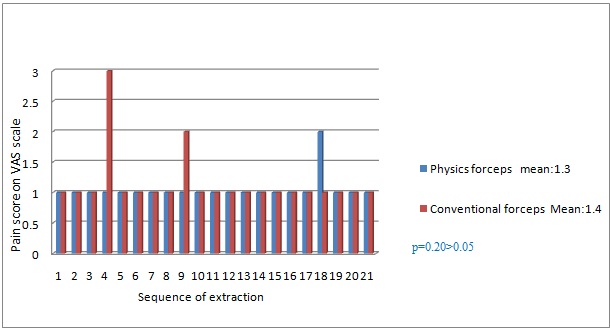
Pain Score: Postoperative pain measured on VAS scale was recorded on 1st and 3rd post-op day. Mean VAS score on 1st post-op day using physics forceps and conventional forceps were 3.19 and 3.71 respectively. Mean VAS score on 3rd post-op day using physics forceps and conventional forceps were 1.04 and 1.14. However, the difference in pain score using either forceps were not statistically significant [Table/Fig-9a&b].
Graphical comparison of Pain on 1st post op day.
Graphical comparison of pain on 3rd post op day.
Discussion
Tooth extraction requires controlled force and fineness for atraumatic extractions [5]. Various instruments and techniques have been described to aid atraumatic tooth extraction. The advantage of physics forceps over conventional forceps and all other extraction techniques is related to their unique design that can deliver a powerful mechanical advantage by employing an efficient first-class lever. Unlike the conventional forceps extraction technique, in physics forceps the buccal portion of the beak is a plastic covered bumper which is placed apically in the vestibule and work by rotation of the wrist rather than a squeezing movement [8].
In physics forceps the length of the forceps handle to the bumper is 8 cm and the distance from the bumper to beak is 1 cm so the torque force that is generated on the tooth, periodontal ligament, and bone is equal to length of handle (8cm) divided by the distance from the bumper to the beak of the forceps (1cm), so the force that is applied on the handle attached to the bumper will therefore increase the force on the tooth, periodontal ligament, and bone by about 8 times [9]. The force applied by the bumper onto the gingiva and bone is distributed over a larger surface area and is a compressive force, so the tooth and alveolus do not fracture. Once the tooth is subluxated it can be delivered with the help of conventional forceps or a rongeur [6]. Conventional dental forceps are class 2 levers that are connected with hinge. Forces are applied on the long side of the lever i.e. the handles, the beaks act as the load arm of the lever, hinge act as fulcrum and tooth to be extracted act as load. Hence the force applied on the handle is magnified to allow the forceps to grasp the tooth and does not provide mechanical advantage to extract the tooth.
According to Dym and Weiss, there is no need to raise a mucoperiosteal flap or use an elevator before attempting extraction with the Physics forceps. This is a major advantage, particularly in cases that require atraumatic extraction [5].
Time taken to extract the teeth can be considered as a time period from engaging the tooth by forceps to completely removing the tooth out of socket. Physics forceps require constant traction force involving only unidirectional force for extraction of any tooth while conventional forceps involve buccal and lingual directing force to luxate the tooth followed by twisting or rotating force depending on the tooth to be removed which can increase the intra operative time. In the present study it was found that the time required to extract using physics forceps was significantly lesser as compared to that of conventional forceps which is in accordance with the results reported by Long et al., in their paper presented at International Association of Dental Research, 2010 [9]. Mandal S et al., in their comparative study also reported the same results with mean extraction time of 139.8 sec using physics forceps and 236 sec using conventional forceps [10]. Whereas S Hariharan et al., in their study did not find significant difference in time taken, with mean extraction time using physics forceps 29.4 sec and conventional forceps 43.5 sec [9].
Conservation of marginal bone following tooth extraction is very important in recent era of Implantology. Physics forceps was claimed to prevent the marginal bone loss by its developer GOLDEN/MISCH [8]. So, in the present study quantitative comparison of marginal bone loss after extraction with physics forceps and conventional forceps was done using Williams probe, which according to our knowledge has not been reported in the literature so far. Mean marginal bone loss following extractions using physics forceps was significantly lesser when compared to the conventional forceps. Buccal cortical plate fracture was noted in 2 (4.76%) patients in physics forceps group following extraction in the initial period which may be associated with learning curve of the operator which is also described by Perkins NJ et al., in their paper presented at British Association of Oral and Maxillofacial Surgeons, 2010 [9].
In the present study significant difference of mean changes in pre extraction and post extraction gingival level was found using physics forceps and conventional forceps which suggested that physics forceps was comparatively less traumatic to the gingival tissues when compared to conventional forceps. Mandal S et al., compared the gingival tissue status following extraction using physics forceps and conventional forceps by clinically examining for the presence or absence of laceration on marginal gingiva. They found gingival laceration in 16.6% in physics forceps group and 52.38% in conventional forceps group and concluded physics forceps can performs extractions less traumatically than conventional forceps which is in accordance to present study [10].
Postoperative pain in extractions done by physics forceps and conventional forceps using Visual Analogue Scale (VAS) was also measured in the present study. Results suggested that there was no statistically significant difference in VAS score on 1st and 3rd postoperative days between two groups however lower mean VAS score was noted in the physics forceps group which may be attributed to comparatively less traumatic extractions done by physics forceps. The results are at par with the conclusions of S Hariharan et al., who found significantly lesser postoperative pain in physics forceps group on first postoperative day when compared to conventional forceps [9].
Complications are unexpected events that tend to increase the morbidity, above what would be expected from a particular operative procedure under normal circumstances [11]. Although their occurrences are rare, but it can lead to a prolonged phase of treatment, which is cumbersome to the patient and the clinician also. Complications associated with tooth extraction can range from simple ones like root and crown fracture to uncommon serious ones like displacement of root fragment in the maxillary sinus [12]. In the present study 4.76% root tip fractures were noticed which were all in conventional forceps group. Overall success rate with physics forceps was 96% while that with conventional forceps was 90%. Choi et al., in their study found 93% success rates with physics forceps which is in accordance with our study [7].
In the present study we found mild swelling on 1st postoperative day in 2.38% (1 case) of extraction done by physics forceps and 4.76% (2 cases) extractions done by physics forceps. Tooth fracture (irrespective of crown and root fracture) was noted in 6% of total extractions which was equal in both physics forceps and conventional forceps groups (3% each). Buccal cortical fracture was noted in 4.76% of total extractions done by conventional forceps and no cortical fracture in extractions done by conventional forceps which was in accordance to the study done by Mandal S et al., [10]. No other complications were noted in any of the groups in present study.
The present study was a split mouth study which eliminated many patient related biases (such as nutritional status, oral hygiene, bone quality, patient compliance etc.) and operator related biases as single operator performed all the procedures. The use of the physics forceps is limited to the patients who are having sufficient mouth opening and to teeth which are anatomically aligned in normal positions.
Limitation
The limitations of the present study include limited sample size and inclusion of only premolars. Encouraging results found in the present study with physics forceps in preservation of tooth supporting structures following extraction opens new directions in atraumatic extraction techniques. We leave it to the conscience of the readers to conduct prospective studies with larger sample size and including all the teeth (sound and decayed).
Conclusion
From the present study it can be concluded that physics forceps maintains the integrity of gingiva and surrounding periodontium. So extractions using physics forceps are less invasive over conventional forceps and can be considered as reliable method for extraction requiring comparative less intraoperative time.