Native Triple Valve Endocarditis as Complication of Post-Abortal Sepsis
Mohan Venkata Sumedha Maturu1, Tom Devasia2, Mugula Sudhakar Rao3, Hashir Kareem4
1 Junior Resident, Department of Medicine, KMC Manipal, Manipal University, Manipal, Karnataka, India.
2 Professor, Department of Medicine, KMC Manipal, Manipal University, Manipal, Karnataka, India.
3 Registrar, Department of Cardiology, KMC Manipal, Manipal University, Manipal, Karnataka, India.
4 Associate Professor, Department of Cardiology, KMC Manipal, Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mugula Sudhakar Rao, Registrar, Department of Cardiology, Kasturba Medical College, Manipal university, Manipal, Karnataka, India.
E-mail: msudhakar88@gmail.com
Infective endocarditis (IE) is a highly morbid condition in pregnancy which poses both maternal and fetal risk. In majority of cases, endocarditis occurs only on single valve and usually occurs on valve with structural disease or prosthetic valve. Multi-valvular involvement is not common and so we report a case of native triple valve endocarditis as a complication of post abortal sepsis which was successfully treated medically.
Infective endocarditis, Pregnancy, Rheumatic heart disease
Case Report
A 25-year-old primigravida reported to the Department of Cardiology, with fever of 2 weeks duration which was not responding to conventional antibiotics. She recently had a spontaneous second trimester abortion at 5 months period of gestation at another hospital. There was no history suggestive of rheumatic heart disease in the past. The details regarding the condition of patient at presentation to another hospital, duration of rupture of membranes, duration between rupture of membranes and expulsion of products of conception, characteristics of fluid upon rupture of membranes, presence of any discharge, reason for spontaneous abortion or the details of medications prescribed after abortion were not known as there was no documented evidence available with patient or her relatives. On the second day patient started to have fever spikes and was started on oral antibiotics for which she responded only transiently. Once fever recurred she was referred to us.
On presentation to our hospital she was conscious, alert and oriented. She was febrile, tachypenic but was maintaining fair saturation without oxygen support and her vitals were stable except for sinus tachycardia. On general examination, she was pale, nail beds showed splinter haemorrhages and she had painless erythematous lesions over palms which were consistent with janeway lesions. Respiratory system examination revealed bilateral fine basal crepitations. Cardiovascular examination revealed pan systolic murmur which was heard all over the precordium. Obstetric opinion was sought and was advised conservative management as there were no retained products of conception. During the stay she developed new onset left haemiparesis with dysarthria. She was empirically started on teicoplanin, piperacillin-tazobatum in view of post-abortal sepsis with possible infective endocarditis. Her laboratory investigations showed low haemoglobin (7.9 gm/dl), elevated total leukocyte counts (27,300 cells/c.mm), deranged renal functions (creatinine – 6.1 gm/dl) and deranged liver functions (AST – 62, ALT – 68, ALP – 196). Chest X-ray showed features suggestive of pulmonary oedema. Transvaginal USG did not reveal any retained products of conception.
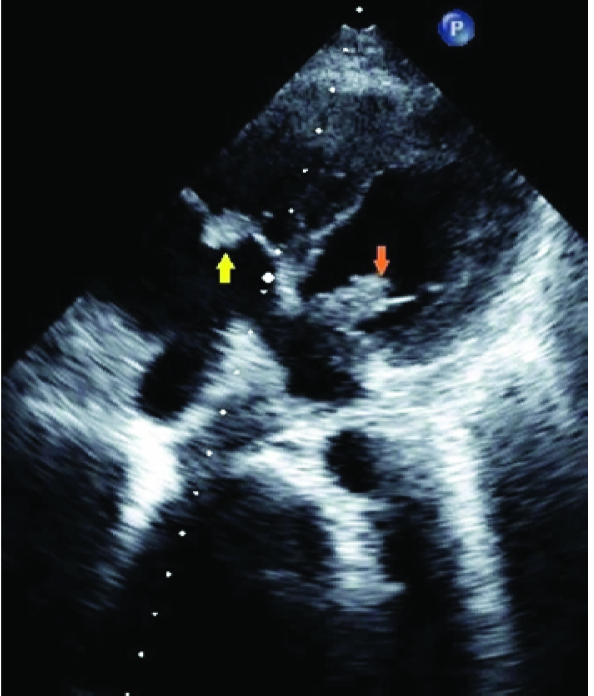
Echocardiography [Table/Fig-1,2] revealed features suggestive of rheumatic heart disease – Moderate mitral stenosis (MS), with vegetations involving three native valves (1.1X 0.6cm vegetation over anterior mitral leaflet with Moderate MS and mild Mitral regurgitation (AR), 0.5cm X 0.4cm vegetation on aortic valve with moderate Aortic regurgitation (AR), 2.0cm X 0.8cm vegetation on anterior tricuspid leaflet with moderate TR).
Transthoracic echocardiogram in apical four chamber view - yellow arrow shows 2.0cmX0.8cm vegetation on anterior tricuspid leaflet, orange arrow shows 1.1cmX0.6cm vegetation over anterior mitral leaflet.
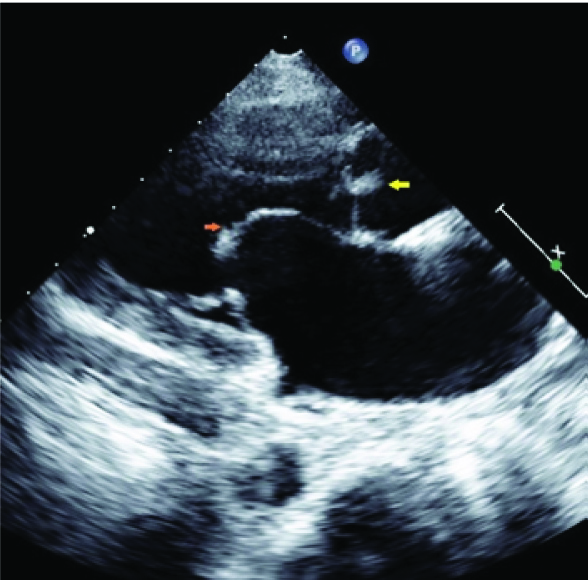
Transthoracic echocardiogram in parasternal long axis view - yellow arrow shows 0.5cmX0.4cm vegetation on aortic valve, orange arrow shows doming of mitral valve which represents mitral stenosis.
Three blood cultures grew methicillin Sensitive Staphylococcusaureus (MSSA). But her urine culture and cultures of swabs taken from vaginal fornices and cervix did not grow any organism.
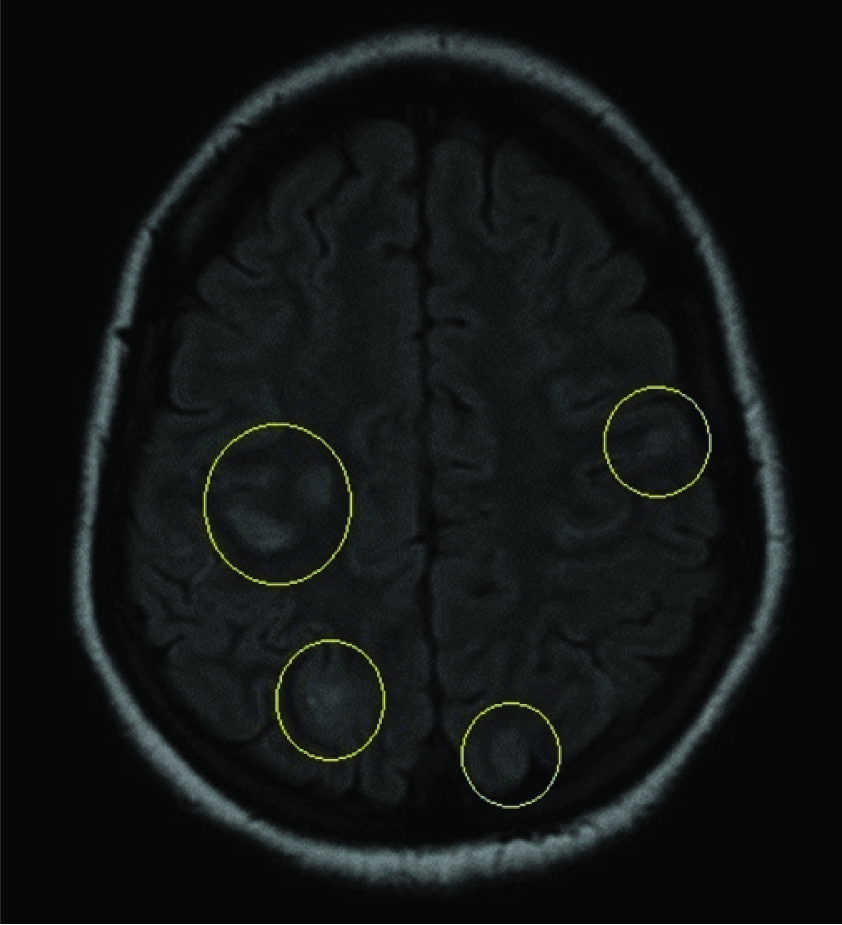
MRI brain [Table/Fig-3,4] showed features suggestive of early sub-acute infarcts in the bilateral frontal (R>L), bilateral parietal, left occipital lobes, right cerebellar hemisphere, right centrum semiovale.
MRI Brain, FLAIR sequence - yellow circles show areas of hyper-intensities distributed in bilateral frontal and parietal regions.
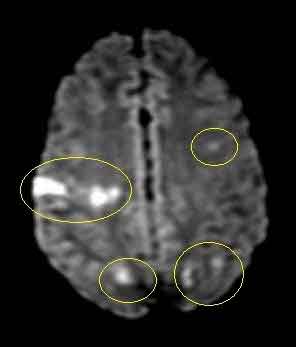
MRI brain, diffusion weighted image - yellow circles show areas of diffusion restriction indicating acute infarction which are distributed in bilateral frontal and parietal regions.
She was empirically started on teicoplanin, piperacillin-tazobactum as possibility of infective endocarditis complicating post-abortal sepsis was considered based on clinical features. As culture and sensitivity showed MSSA, her antibiotics were revised to cloxacillin and vancomycin which were given for a period of 6 weeks. General cardiac failures regimens were continued along with closely monitored intravenous hydration in view of both cardiac and renal failure. She was also prescribed anti-platelets along with physiotherapy and speech therapy in view of multiple infarcts.
Discussion
Infective Endocarditis (IE) refers to inflammation of inner layer of heart viz. the endocardium along with valves which is caused by a multitude of infectious agents, staphylococci and streptococci being most common [1]. The exact incidence of IE is difficult to determine as the incidence of predisposing conditions like rheumatic heart disease or intravenous drug abuse vary over time and place [2]. Majority of patients with IE have underlying structural, congenital or prosthetic valve while IE of native valve if relatively uncommon [3]. Pregnancy, especially third trimester and post – partum period are extremely prone to develop IE owing to physiologic changes in circulation, cardiac hypertrophy which is maximum in third trimester and tend to return to baseline by 8 weeks post-partum [4]. Also, pregnancy itself is a pro-inflammatory state which predisposes to infection [5]. Our patient presented within first week post abortion and there was no evidence of any structural or congenital valvular lesions.
In a patient who is being evaluated for IE, demonstration of number of involved valves is very important. It has been shown that as the number of valves involved increase, the likelihood of complications like congestive heart failure, acute renal failure, occurrence of embolic events (i.e., pulmonary embolism, cerebral vascular accident, disseminated intravascular coagulation, etc.,) and splenic abscess/infarct increase [6]. Majority of IE occur on a single valve and multi-valvular involvement is rare. Among the case reports of multi-valvular IE, left sided lesions predominate with very few reports showing involvement of both left and right sided lesions [7]. Most likely reason for left side predominance would be higher turbulent flow across valves and higher prevalence of congenital and acquired anomalies of left sided valves. Right sided lesions can be explained by intravenous drug use [8]. Our patient had native triple valve endocarditis with echocardiographic evidence of mitral, aortic and tricuspid valve involvement which is complicated by congestive cardiac failure, renal failure and multiple embolic infarcts.
As rate of complications and mortality is high in multi-valvular endocarditis, management usually requires aggressive antibiotic therapy and surgical interventions [6]. However, our patient has improved with just medical management without any need for any surgical interventions. We report this case as our patient presented with native valve endocarditis involving both left and right sided valves as part of post-abortal sepsis which was successfully treated
Conclusion
Though infective endocarditis is fairly common in pregnancy and peri-partum period, native multi-valve endocarditis as a complication of post abortal sepsis has been rarely described in literature.
[1]. Selton-Suty C, Célard M, Le Moing V, Doco-Lecompte T, Chirouze C, Iung B, Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-based surveyClinical Infectious Diseases 2012 54(9):1230-39. [Google Scholar]
[2]. Tleyjeh IM, Abdel-Latif A, Rahbi H, Scott CG, Bailey KR, Steckelberg JM, A systematic review of population-based studies of infective endocarditisCHEST Journal 2007 132(3):1025-35. [Google Scholar]
[3]. de Sa DDC, Tleyjeh IM, Anavekar NS, Schultz JC, Thomas JM, Lahr BD, Epidemiological trends of infective endocarditis: a population-based study in Olmsted County, MinnesotaMayo Clinic Proceedings 2010 Elsevier [Google Scholar]
[4]. Schannwell CM, Zimmermann T, Schneppenheim M, Plehn G, Marx R, Strauer BE, Left ventricular hypertrophy and diastolic dysfunction in healthy pregnant womenCardiology 2002 97(2):73-78. [Google Scholar]
[5]. Mor G, Cardenas I, Review Article: The immune system in pregnancy: a unique complexityAmerican Journal of Reproductive Immunology 2010 63(6):425-33. [Google Scholar]
[6]. Kim N, Lazar J, Cunha B, Liao W, Minnaganti V, Multi-valvular endocarditisClinical Microbiology and Infection 2000 6(4):207-12. [Google Scholar]
[7]. Sakakura K, Kubo N, Katayama T, Umemoto T, Oosawa S, Murata S, Successfully treated triple valve infective endocarditis: a case reportJ Cardiol 2005 45(6):257-62. [Google Scholar]
[8]. Frontera JA, Gradon JD, Right-side endocarditis in injection drug users: review of proposed mechanisms of pathogenesisClinical Infectious Diseases 2000 30(2):374-79. [Google Scholar]