The continuously altering nature of the SDH has often put the forensic community in a disadvantageous position about its duration and if improperly interpreted may lead to legal catastrophes in the fact that an innocent may be found guilty and a culprit vice versa. The occurrence of the external injuries, at least, can be related roughly to a particular time interval [6]. But in cases of SDHs which are often not associated with a fracture of the skull, cerebral contusions or any other visible brain injury, it becomes very much difficult to date even roughly. A lot of ambiguity regarding the same remains, especially when multiple traumatic events are detected in the same case. Hence in these cases, it is crucial to determine the time of occurrence of the event leading to SDH. Very few studies have described the histomorphological [7–9] and radiological [10–13] changes of injuries about its time of occurrence.
Barring a few studies in the west, most of which were conducted far back in the early part of the 20th century, there has been no study from India of SDHs for the determination of PTI. In the present study, histopathological changes following SDHs were correlated with known PTIs in medico legal perspective. This knowledge provides for resolving many complicated medico-legal issues related to the age of SDH, as well as in delineating the diagnostic and treatment modalities according to the age of SDH.
Materials and Methods
After obtaining clearance from the ethical clearance committee of the Institute (PGIMER, Chandigarh), this prospective analytical study was conducted during July 2009 to December 2010 in the Department of Forensic Medicine in collaboration with the department of Pathology and Neurosurgery. With a valid written informed consent of the legal heirs of the deceased, 100 cases (50 males and 50 females) above the age of 18yrs and treated conservatively for closed traumatic brain injury with SDH were included in this study. These cases were admitted to the emergency neurosurgery department with confirmed history of head trauma, known topography, exact manner, mode and time since the trauma. Cases with a history of ataxia, stroke, dementia, haemorrhagic tendencies (liver cirrhosis, anticoagulant treatment, and haemorrhagic diathesis), surgical treatment, known prior head injury, recurrent intracranial bleeding (as observed clinically and radiologically) and with more than one episode of epilepsy were excluded from this study. All the cases in the present study had a post mortem interval of less than 48 hours and were stored in cold chamber till the commencement of the autopsy.
Histological Procedure
Sections of the brain along with the dura mater were removed at the time of autopsy; great care was taken not to disturb the clot underlying the dura as it usually falls away from the underside of the dura. The specimen was fixed in 10% neutral buffered formalin for 20 days and embedded in paraffin. Sections of 5 micrometers were cut and prepared for routine light microscopy after staining with Haematoxylin and eosin (H&E), Perl’s stain (Prussian blue reaction), Periodic Acid Schiff (PAS), and Masson’s Trichrome.
Histopathological Evaluation
Histomorphological features of the dura and the clot such as Red Blood Cells (RBCs), Polymorphonuclear Leukocytes (PMN), macrophages, and red blood cell containing macrophages, haemosiderin containing macrophages, fibroblasts, collagen fibers, capillary proliferation and early membrane formation were examined by two independent observers blinded to survival time. The criteria for identification and differentiation of cell types were pragmatic. The red blood cells were grouped into three categories–intact, lysed and mixed depending on the morphological features. Subdural clot having red blood cells of normal size, shape and uniform staining properties were classified as intact. Lysed category comprised laked RBCs with variable staining properties and the mixed group having properties of both the intact and lysed categories. The neutrophils were graded semi- quantitatively depending on their counts in the clot/dura-clot interface (extravascular) into 0, 1+, 2+, and 3+, with 0 representing very scarce/absent neutrophils, 1+ up to 3 clusters, 2+ more than three clusters, and 3+ being diffusely present in the clot/dura-clot interface. The rest of the histomorphological features were grouped depending on their presence or absence. The demonstration of RBC containing macrophages and haemosiderin containing macrophages were considered positive only if they were located within the clot. A histomorphological feature if identified at least twice in each section was regarded as a positive finding. In the case of difference in observation regarding a morphological finding, an additional examination was done by each observer.
Statistical Analysis
Data was analysed using SPSS (SPSS 17.0 for Windows, Chicago, IL, USA). In all cases, a p< 0.05 was considered statistically significant. The cases were arbitrarily divided into groups about post-traumatic interval (PTI) into Group 1 (< 24h), Group 2 (24.1-48h), Group 3(48.1- 72h), Group 4 (72.1-96h), and group 5 (>96h). Histomorphological features were correlated with post-traumatic interval groups using Chi-square test. One-way ANOVA was applied for comparison of RBCs and PMNs with PTI followed with Bonferroni correction for RBCs. Logistic regression of forensic relevant posttraumatic intervals was performed. Cases were divided into two groups with one group having a post-traumatic interval of lesser than 96 hours (n=64) and the other with a post-traumatic interval of more than 96 hours (n=36). All the variants were correlated with the post-traumatic interval.
Results
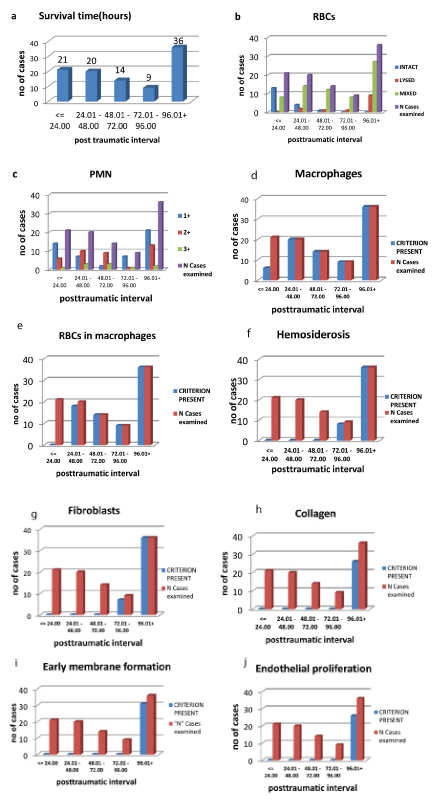
In our study the PTI ranged from a minimum of 5 hours to a maximum of 253 hours and the distribution of cases according to PTI has been presented in [Table/Fig-1a]. [Table/Fig-1-b-j] represents the frequency of different histomorphological features in comparison with the PTI groups.
(a) Classification of all the cases according to survival time, (b) Frequency of detection of red blood cells, (c) PMN, (d) Macrophages, (e) RBCs in Macrophages, (f) Hemosiderin containing macrophages, (g) Fibroblast, (h) Collagenous fibers, (i) Early membrane formation, (j) Endothelial proliferation in the subdural hemorrhage about post-traumatic interval (hours).
Lysis of red blood cells was observed partly beginning at a PTI of 7 hours. The majority of the cases with complete lysis of RBCs were found to have a PTI greater than 96 hours. Bonferroni statistics was applied for post hoc multiple comparisons of intact, mixed and lysed groups of RBCs as the ANOVA table value was significant (F=27.619, p=0.0001). It was observed that there was significant difference between all the RBC groups i.e., the intact, mixed and the lysed groups (p=0.0001) [Table/Fig-2a-c].
Results -One-wayANOVA test for RBC
| (a) Descriptive |
|---|
| Time | N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum |
|---|
| Lower Bound | Upper Bound |
|---|
| Intact | 18 | 18.0278 | 12.41118 | 2.92534 | 11.8558 | 24.1997 | 5.00 | 52.50 |
| Lysed | 8 | 185.0125 | 85.82143 | 30.34246 | 113.2640 | 256.7610 | 28.00 | 253.00 |
| Mixed | 74 | 86.6716 | 55.77459 | 6.48366 | 73.7497 | 99.5935 | 7.00 | 245.00 |
| Total | 100 | 82.1830 | 66.77513 | 6.67751 | 68.9334 | 95.4326 | 5.00 | 253.00 |
| (b)ANOVA |
|---|
| PTI | Sum of Squares | df | Mean Square | F | p- value |
|---|
| Between Groups | 160168.246 | 2 | 80084.123 | 27.619 | .0001 |
| Within Groups | 281264.595 | 97 | 2899.635 | | |
| Total | 441432.841 | 99 | | | |
| c) Post Hoc Tests |
|---|
| Multiple Comparisons (Bonferroni) |
|---|
| (I) RBC | (J) RBC | Mean Difference (I-J) | Std. Error | p- value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Intact | Lysed | -166.98472* | 22.88111 | .000 | -222.7278 | -111.2416 |
| Mixed | -68.64384* | 14.15186 | .000 | -103.1207 | -34.1670 |
| Lysed | Mixed | 98.34088* | 20.04092 | .000 | 49.5171 | 147.1647 |
(DF=degree of freedom,F=F-Value).
PMN were observed from the minimum PTI to the maximum PTI. There were no cases in which neutrophils were very scarce or absent in our study. Few cases (n=8) showed more than three clusters of neutrophils even in the early PTI (<24h). But for the rest of the cases, the count varied with PTI initially being few, then gradually increasing with the PTI and finally decreasing at higher PTI One-way ANOVA revealed no difference between the three groups (1+,2+, and 3+) of PMN (F=1.320, p=0.272) [Table/Fig-3a-c].
Results-One-way ANOVA test for PMN.
| (a) Descriptive |
|---|
| PTI | N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum |
|---|
| Lower Bound | Upper Bound |
|---|
| 1+ | 50 | 91.7560 | 71.73034 | 10.14420 | 71.3705 | 112.1415 | 5.00 | 253.00 |
| 2+ | 39 | 76.3897 | 65.87203 | 10.54797 | 55.0365 | 97.7430 | 6.30 | 243.80 |
| 3+ | 11 | 59.2091 | 35.68250 | 10.75868 | 35.2373 | 83.1809 | 14.80 | 123.00 |
| Total | 100 | 82.1830 | 66.77513 | 6.67751 | 68.9334 | 95.4326 | 5.00 | 253.00 |
| (b) ANOVA |
|---|
| PTI | Sum of Squares | df | Mean Square | F | p-value |
|---|
| Between Groups | 11696.833 | 2 | 5848.416 | 1.320 | .272 |
| Within Groups | 429736.008 | 97 | 4430.268 | | |
| Total | 441432.841 | 99 | | | |
| (c) Post Hoc Tests |
|---|
| Post Hoc TestsMultiple Comparisons (Bonferroni) |
|---|
| (I) PMNs | (J) PMNs | Mean Difference (I-J) | Std. Error | p- value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| 1+ | 2+ | 15.36626 | 14.21977 | .848 | -19.2760 | 50.0086 |
| 3+ | 32.54691 | 22.16657 | .436 | -21.4554 | 86.5493 |
| 2+ | 3+ | 17.18065 | 22.72330 | 1.000 | -38.1780 | 72.5393 |
(DF=degree of freedom,F=F-Value).
Macrophages, Red Blood Cells containing macrophages, haemosiderin containing macrophages, fibroblast, collagenous fibers, early membrane formation, endothelial proliferation were first observed at a PTI of 17.3 hours, 24.5hours, 80 hours, 89.5 hours, 110.5 hours, 114.5 hours and 123 hours respectively, up to the last case. Also, all the criteria in our study had distribution-free tolerance intervals of more than 90%. [Table/Fig-4] All these histomorphological features were correlated with PTI groups and were statistically highly significant (p=0.0001) [Table/Fig-5a,b].
| Histomorphological criteria | Appearance(hours) | Total no. of casesexamined during the observation period | Number of caseswith morphologicalalteration | Distribution free tolerance interval with 95% reliability (%) |
|---|
| First | Last |
|---|
| Red Blood Cells (RBC) | Intact | 5 | 52.5 | 100 | 18 | 98 |
| Mixed | 7 | 245 | 74 |
| Lysed | 28 | 253 | 8 |
| Polymorphonuclear leukocytes | 0 | - | - | 100 | - | 94 |
| 1+ | 5 | 253 | 50 |
| 2+ | 6.3 | 243.8 | 39 |
| 3+ | 14.8 | 123 | 11 |
| Macrophages | 17.3 | 253 | 100 | 86 | 98 |
| RBCs in Macrophages | 24.5 | 253 | 100 | 79 | 97 |
| Hemosiderin containing macrophages | 80 | 253 | 100 | 45 | 99 |
| Fibroblast | 89.5 | 253 | 100 | 40 | 96 |
| Collagenous fibres | 110.5 | 253 | 100 | 28 | 98 |
| Early membrane formation | 114.5 | 253 | 100 | 26 | 97 |
| Endothelial proliferation | 123 | 253 | 100 | 24 | 97 |
Correlation of histopathological features with post traumatic interval groups using Chi- square test.
| (a) Post traumatic Interval(hrs) |
|---|
| <= 24.00 | 24.01 - 48.00 | 48.01 - 72.00 | 72.01 - 96.00 | 96.01+ | Total |
|---|
| Macrophage | Absent | 14 | 0 | 0 | 0 | 0 | 14 |
| Present | 7 | 20 | 14 | 9 | 36 | 86 |
| Fibroblast | Absent | 21 | 20 | 14 | 5 | 0 | 60 |
| Present | 0 | 0 | 0 | 4 | 36 | 40 |
| RBC in macrophage | Absent | 21 | 0 | 0 | 0 | 0 | 21 |
| Present | 0 | 20 | 14 | 9 | 36 | 79 |
| Hemosiderosis | Absent | 21 | 20 | 14 | 0 | 0 | 55 |
| Present | 0 | 0 | 0 | 9 | 36 | 45 |
| Collagen | Absent | 21 | 20 | 14 | 9 | 12 | 76 |
| Present | 0 | 0 | 0 | 0 | 24 | 24 |
| Capillary formation | Absent | 21 | 20 | 14 | 9 | 8 | 72 |
| Present | 0 | 0 | 0 | 0 | 28 | 28 |
| Membrane formation | Absent | 21 | 20 | 14 | 9 | 10 | 74 |
| Present | 0 | 0 | 0 | 0 | 26 | 26 |
| (b) Pearson Chi-Square Tests |
|---|
| PTI | Chi-square | df | p- value |
|---|
| Macrophage | 61.24 | 4 | 0.0001 |
| Fibroblast | 90.741 | 4 | 0.0001 |
| RBCs in Macrophage | 100 | 4 | 0.0001 |
| Hemosiderosis | 100 | 4 | 0.0001 |
| Collagen | 56.14 | 4 | 0.0001 |
| Capillary formation | 69.136 | 4 | 0.0001 |
| Membrane formation | 62.462 | 4 | 0.0001 |
(DF=degree of freedom)
Logistic regression was deduced using all the histopathological variables with respect to time since the injury. The rate of successful classification was 93.8% for the group with a survival time of </=96 hours, and 100% for the group surviving more than 96 hours. The average success rate was 96%. Out of all the variants, only fibroblasts and early membrane formation were found to be significant [Table/Fig-6a-e].
Results of logistic regression tables using histopathological variables with respect to time since injury (a-e).
| (a) Dependent Variable Encoding |
|---|
| Original Value | Internal Value |
|---|
| <= 96 | 0 |
| >96 | 1 |
| (b) Omnibus Tests of Model Coefficients |
|---|
| | Chi-square | df | Sig. |
|---|
| Step 2 | Step | 13.641 | 1 | .000 |
| Block | 118.318 | 2 | .000 |
| Model | 118.318 | 2 | .000 |
| (c) Model Summary |
|---|
| Step | -2 Log likelihood | Cox & Snell R Square | Nagelkerke R Square |
|---|
| 2 | 12.365a | .694 | .951 |
| (d) Classification Table |
|---|
| Observed | Predicted |
|---|
| PTI | Percentage Correct |
|---|
| <= 96.00 | 96.01+ |
|---|
| PTI | <= 96.00 | 60 | 4 | 93.8 |
| 96.01+ | 0 | 36 | 100.0 |
| Overall Percentage | | | 96.0 |
| (e) Variables in the Equation (Logistic Regression) |
|---|
| Variable | B | S.E. | Model Log Likelihood | Change in -2 Log Likelihood | df | p-value |
|---|
| Fibroblast | 21.426 | 5188.890 | -17.938 | 23.510 | 1 | .0001 |
| Membrane formation | 20.980 | 7218.871 | -13.003 | 13.641 | 1 | .0001 |
| Constant | -21.203 | 5188.890 | | | | |
Discussion
There is an increasing awareness among the common public as well as the medical fraternity of the prevalence of traumatic brain injury and its clinical sequelae which have led to an exponential increase in the number of lawsuits and medico-legal cases. Microscopic study of the organization of the SDH verified against the time period can help us in the determination of its age. This determination can be especially valuable in the absence of a true history of the events along with other parameters for the determination of PTI.
The majority of the SDH cases which are encountered in routine practice have PTIs within the clinically classified acute and subacute phases [13]. In this study, all the cases were observed within the PTI period of 253 hours. The lysis of red blood cells was initially observed in the center of the clot and later along the periphery [Table/Fig-7a]. Although Walter et al., found intact red blood cells even up to 4 months of PTI; their study did not consider it as criteria for the histological dating of SDHs in their study [7]. Fibrin strands were noted within a few hours of the occurrence of the SDH though was not quantified in this study.
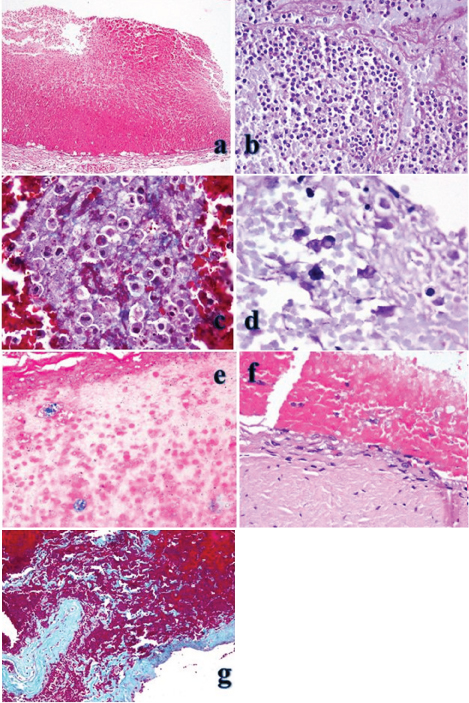
(a) Photomicrographs of acute SDH of <24 hrs duration is showing fresh hemorrhage with intact red blood cells. There is acute hemorrhage with alarge number of neutrophils seen on the dural side. (H&E x200) (H&E-hematoxylin and eosin). (b) Acute SDH (24-48hrs)-There is acute hemorrhage with fibrin infiltration. Many neutrophils (4+grade) and a few macrophages are seen (PAS, x400) (PAS-Periodic acid-Schiff) (c) Photomicrograph of SDH (4 days old) showing hemophagocytosis (Masson’s trichrome x1000) (d) Photomicrograph of SDH (4 days old) showing hemophagocytosis (PAS x1000) (PAS-Periodic acid-Schiff). (e) Photomicrograph showing hemosiderin-laden macrophages in the SDH-6 day old. (Prussian blue-reaction x400) (f) Photomicrograph showing SDH (6 days old) having a 3-5 cells thick layer of fibroblastsat the dural-clot interface. (H&E, x400) (H&E-hematoxylin and eosin). (g) Photomicrograph showing SDH 8 days old. Infiltration of the collagen into the hematoma can be observed (Masson’s trichrome, x200).
As observed by Walter et al., during the early stages of trauma, the polymorphs are usually seen within or in the vicinity of the blood vessels of the meningeal dura [7]. Later they spread along the dura-clot interface and into the clot. But statistically, polymorphs did not correlate with the PTI groups in the present study [Table/Fig-7b]. Also, neutrophils were observed in larger numbers in a few early cases. To explain the above phenomenon, one may hypothesize that the increase in the number of neutrophils may be due to the injury rather than a reaction to it. In simple terms, few of the circulating neutrophils in hemic proportions might have spilled into the subdural space at the moment of rupture of the bridging veins. This accumulation of the neutrophils along the dura-clot interface would have resulted in greater number of neutrophils observed in the early posttraumatic periods. The neutrophils which are reactionary to the injury appeared late and were accompanied by vascular alterations such as dilatation, endothelial swelling, emargination, and emigration, etc. (signs resembling inflammatory changes). Also, the biological function of leukocyte immigration is not known about traumatic brain injury and haemorrhage [14].
This study differed from the observations of Walter et al., in that the first detection of macrophage was made at the 12th hour [7]. This may be because CD68 monoclonal antibody was used to detect the presence of the same. Though Munro and Merritt made no mention of the duration of appearance of the macrophages, the pigment-laden histiocytes appeared on the 5th day [9]. Engel et al., detected the macrophages as early as 6 hours in their study on the markers of macrophages in cases of closed head trauma [15]. Another study conducted to detect the macrophage reactivity of the dura and the SDH using immunohistochemistry revealed that the expression of major histo-compatibility complex (MHC) class II can be observed within the first 24 hours whereas the CD68 expression can be detected quantitatively in 24-48 hours following the trauma along the inner aspect of the dura [16].
Haemophagocytosis was first observed at 24.5 hours in the present study, compared to 20 hours and 72 hours by Walter et al., and Munro & Merritt studies respectively [Table/Fig-7c,d]. Perls stained sections were considered reliable as it could differentiate between formalin pigments and the haemosiderin. Haemosiderin containing macrophages were detected at similar time periods as in Walter et al., study (79h) whereas it was detected around the 5th day by Munro and Merritt [Table/Fig-7e].
The first mesenchymal reaction was observed on the fourth day of PTI and was mainly characterized by proliferation and invasion of fibroblasts into the clot from the dural side. The fibroblasts were earliest detected at 89.5 hours in the present study compared to 120 hours by Walter et al. The same was observed by Munro and Merritt on the third day. These cells produce reticular and collagen fibers and mark the onset of early membrane formation at the dura-clot interfaces which are observable on the 5th day [Table/Fig-7f,g], but its thickness was not quantified in the present study. This reactive scarring process is accompanied by endothelial proliferation along the dural margins of the clot. Endothelial proliferation was observed much earlier in our study as compared to Munro and Merritt.
Overall, the observations of the present study deviates from the Munro and Merritt study in the fact that lysed RBCs, neutrophils, and macrophages were detected earlier in our study [9]. When compared to Walter et al., study, the main difference was in the observations regarding PMN as described previously [7].
A brief comparison of two studies on the dating of SDH reveals that the present study scores over the others in the way of producing similar results using routine histopathology staining methods [Table/Fig-8]. Further the authors would like to propose a new classification of the SDH according to the histological features into forensically relevant acute, early subacute and late subacute stages. Till the engulfing of the red blood cells by the macrophages, the SDH may be called acute and from there on till the appearance of the membrane, the early subacute and once the neo-membrane has appeared it may be called late subacute, i.e. <24 hours, 24-114.5 hours, and >114.5 hours respectively in the present study.
Dating of SDH -Comparison with previous studies.
| Present study | Leestma [8] | Walter et al., [7] |
|---|
| Histomorphological criteria | Appearance(hours) | Appearance(h-hours, d-days) | Appearance (Min-minute, h-hours, d-day, m-month, y-year) |
|---|
| First | Last | First | Last |
|---|
| Red Blood Cells (RBC) | Intact | 5 | 52.5 | 36h | 0min | 4m |
| Mixed | 7 | 245 | 3-5d |
| Lysed | 28 | 253 | 15-17d |
| Polymorphonuclear leukocytes | 1+ | 5 | 253 | - | 2.5h | 1m12d |
| 2+ | 6.3 | 243.8 |
| 3+ | 14.8 | 123 |
| Macrophages | 17.3 | 253 | 24-48h | 12h | 30y |
| RBCs in Macrophages | 24.5 | 253 | 3-4d | 20h | 1m2d |
| Hemosiderin containing macrophages | 80 | 253 | 5d | 3d7h | 30y |
| Fibroblast | 89.5 | 253 | 3d | 5d | 28y |
| Collagenous fibres | 110.5 | 253 | 3-5d | 5d | 30y |
| Early membrane formation | 114.5 | 253 | 4d | 5d | 30y |
| Endothelial proliferation | 123 | 253 | 10-15d | 5d | 6y |
| Total no. of cases examined during the observation period | 100 | 105 | 222 |
Limitation
The influence of hypothermia, shock, hypoxia, variations in the blood pressure, the effect of medications during emergency care, potential effects of associated injuries and failure of the internal organs were not evaluated. The variations in the hospital care and treatment, the mode of injuries (high velocity), have considerably changed over the years and hence could have contributed to the observed variations in spite of proper study design. These are also in part due to the active nature of such lesions and the diverse manner in which trauma victims respond to injury. Also due to the short PTI in our study, the role of rebleeding could not be accounted completely in influencing the histological observations about post-traumatic interval.
Conclusion
Though this study was limited to cases with shorter PTIs, there was an apparent correlation between the frequency of a given histomorphological phenomenon and the length of the PTI. Thus we can conclude that histopathology remains the primary tool for estimating the PTIs in SDHs. Further in developing countries, routine staining scores over immunohistochemistry considering cost effectiveness and requirement of technical expertise. For future prospects a long-term study involving more number of cases will help in the better understanding of the overlapping histomorphological characteristics of the SDH with relation to time using routine methods. This study could be extended to cases below 18 years. of age, where its importance is as much as that in the adult age group. Also, additional criteria may be established using other staining methods and by the electron microscope.
(DF=degree of freedom,F=F-Value).
(DF=degree of freedom,F=F-Value).
(DF=degree of freedom)