Bilateral Multi-Focal Sporadic Papillary Renal Cell Carcinoma: A Unique Surgical Challenge
Priyadarshan Anand Jategaonkar1, Smita Priyadarshan Jategaonkar2, Sudeep P. Yadav3, Satyendranath Mehra4
1 Professor and Surgical Gastroenterologist, Department of General, Gastrointestinal and Minimal Access Surgery, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
2 Associate Professor, Department of Pediatrics, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
3 Surgical Trainee, Department of General Surgery, Jagjivan Ram Hospital, Western Railway, Mumbai Central, Mumbai, Maharashtra, India.
4 Head of Unit, Department of General Surgery, Jagjivan Ram Hospital, Western Railway, Mumbai Central, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyadarshan Anand Jategaonkar, 201, Yamuna Apartment, Yashasvi Nagar, Balkum, Thane (W), Thane, Maharashtra-400 608, India.
E-mail: jategaonkarpa@gmail.com
Bilateral renal masses, Kidney cancer, Nephrectomy
Sir,
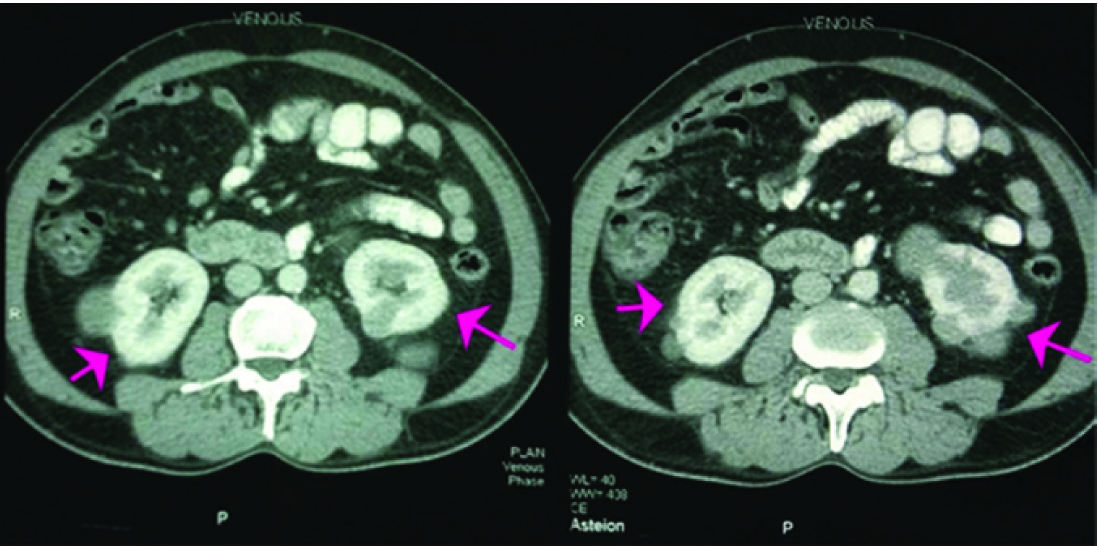
A 53-year-old male presenting primarily for bilateral inguinal hernia had an incidentally detected large left renal mass. His haemogram was normal. Contrast-Enhanced Computed Tomography (CECT) revealed bilateral multi-focal hypodense renal masses suggestive of bilateral Renal Cell Carcinoma (RCC) without dissemination [Table/Fig-1,2]. His renal functions were normal on nuclear scintigraphy. Subsequently, he underwent bilateral staged nephron-sparing surgery (NSS) successfully. Histopathology showed papillary variant (type 1) of RCC on either side. The patient remains healthy on regular follow-up over the last five years.
Abdominal CECT (Transverse section). It depicts bilateral multi-focal hypodense renal masses suggesting RCC (arrows). Note the brightly enhancing nephrograms (preserved renal functions), absence of caval tumour thrombus and dissemination signifying operability.
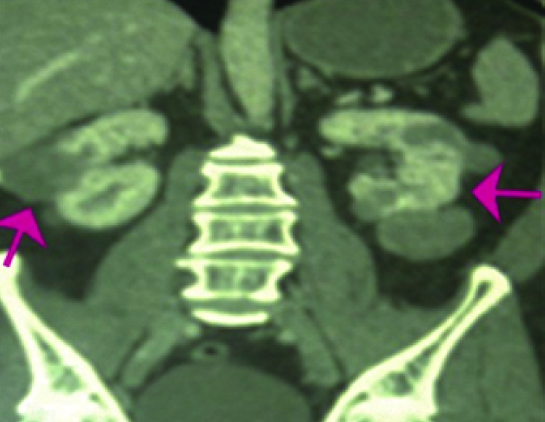
Abdominal CECT (Coronal section). It confirms the multifocality and absence of loco-regional spread (arrows).
Although generally correlated with familial cancer syndromes (particularly the Von Hippel-Lindau syndrome), bilateral RCCs are rare (3-5%) in the epidemiology of the disease [1]. Like in our case, majority are incidentally detected on imaging studies performed for other purposes [2]. Bilateral RCC greatly challenges the surgeons for striking a delicate balance between oncological principles vis-à-vis exploiting renal function to circumvent Renal Replacement Therapy (RRT).
Amongst all pathological sub-types of RCC, papillary variant accounts for 5-15% [2]. It is a slow-growing neoplasm with a relatively favorable prognosis [3]. It is further classified into two broad categories depending on the type of cells noted on the histopathological examination. Type-1 variant has singular cell layer with scanty pale cytoplasm, lesser propensity for dissemination and hence a better prognosis than type 2 having high-grade nuclei and eosinophilic cytoplasm [4]. Abdominal CECT remains the most preferred imaging modality for evaluating their clinical staging and operability [2].
Intending to achieve R0 resection in bilateral RCC, three diversified approaches are considered prudent: 1) Bilateral radical nephrectomy with RRT followed by renal transplantation at a later date; 2) Unilateral radical nephrectomy with contra-lateral NSS; and 3) Bilateral NSS. Amongst them, bilateral NSS is desirable it offers better quality of life and survival benefits akin to those of unilateral tumours [1,2]. It may be accomplished concomitantly or in a staged manner. Considering its higher dissemination propensity and better cancer-specific survival, staged NSS is prioritized for the patient with greater kidney tumour load. This acquires some time not only for designing options for contra-lateral side but also for recuperation of the operated kidney [5]. Though tumours with < 3 cm size do qualify for a vigilant “enucleation”, partial nephrectomy is deemed essential for those with > 3cm size [5]. In any case, the ischemia time critically dictates the ultimate outcome pertaining glomerular filtration [5]. Moreover, at the background of many on-going major clinical trials, the precise role of recently developed targeted/immune-therapies for sporadic papillary RCCs remains elusive, even today [5].
In summary, treating bilateral RCC is a unique surgical challenge that necessitates accurate tailoring of available surgical choices. Bilateral NSS that protects the renal functions without compromising the oncological principles tenders better “quality” and “quantity” of life to these unfortunate individuals.
[1]. Singer EA, Vourganti S, Lin KY, Gupta GN, Pinto PA, Rastinehad AR, Outcomes of patients with surgically treated bilateral renal masses and a minimum of 10 years of follow upJ Urol 2012 188(6):2084-88. [Google Scholar]
[2]. Gossios K, Argyropoulou M, Vazakas P, Stefanaki S, Stavropoulos NE, Bilateral papillary renal cell carcinomaEur Radiol 2001 11(2):242-45. [Google Scholar]
[3]. Deng FM, Melamed J, Histologic variants of renal cell carcinoma: does tumour type influence outcome?Urol Clin North Am 2012 39(2):119-32. [Google Scholar]
[4]. Sari A, Evcim G, Ermete M, Bal K, Bolukbasi A, Papillary renal cell carcinoma with lipocyte-like cells: A rare morphological variant or an indication of aggressiveness?Indian J Pathol Microbiol 2010 53(3):541-43. [Google Scholar]
[5]. Shuch B, Singer EA, Bratslavsky G, The surgical approach to multifocal renal cancers: hereditary syndromes, ipsilateral multifocality, and bilateral tumoursUrol Clin North Am 2012 39(2):133-48. [Google Scholar]