Signet Ring Cell Carcinoma of Urachal Origin Presenting as Irritative Lower Urinary Tract Symptoms and Pain Abdomen: A Rare Case Report
Amit Verma1, Vinay Tomar2
1 Resident, Department of Urology, SMS Medical College, Jaipur, Rajasthan, India.
2 Professor and Head, Department of Urology, SMS Medical College, Rajasthan, Jaipur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amit Verma, Flat No. 202, Plot No. 565, Shivam Enclave, Gali No. 7, Raja Park, Jaipur-302004, Rajasthan, India.
E-mail: dramver.ms@gmail.com
Signet ring cell carcinoma of urachus is a very rare tumour. It generally presents as a high grade, high stage tumour and in most of the cases it has regional or distant metastasis at the time of presentation. It is known to have a uniformly poor prognosis. We present here a very interesting and rare case report of signet ring cell carcinoma of urachus in a 61-year-old male who presented with irritative lower urinary tract symptoms and pain abdomen. High index of suspicion led to the early diagnosis and timely surgical intervention. The patient is doing well on follow-up.
Poor prognosis, Radical cystectomy, Supravesical mass
Case Report
A 61-year-old male, non smoker presented to our hospital with pain lower abdomen, increased frequency of urination (about 15 times during day and 6 times during the night) and urgency of urination for last 6 months. His pain was dull, continuous, non colicky, non radiating and had no relation to food intake. There was no history of weight loss.
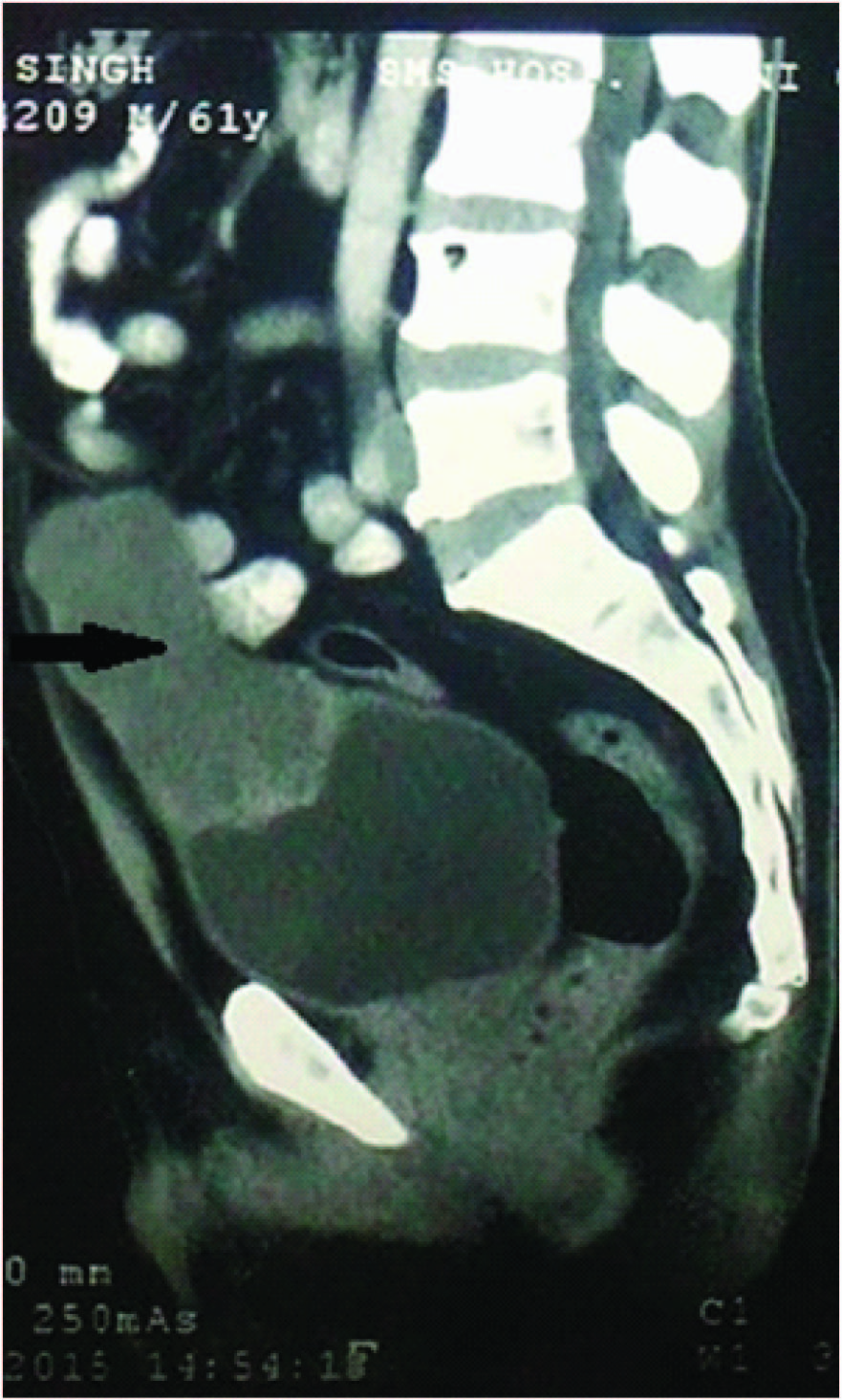
On physical examination, a well defined lump was palpable in the umbilical and hypogastic region, globular in shape, of approximate size 6×5cm, had smooth surface and regular margins all around. The rest of the physical examination was absolutely normal. Ultrasonography showed a solid heterogenous mass of size about 10×5cm above urinary bladder. Urine microscopy and urine cytology were absolutely normal. Computed Tomography (CT) of the abdomen showed a hypodense soft tissue density lesion of size 9×5×6cm in supravesical region with obliterated fat planes from the dome of urinary bladder and the lesion extended superiorly up to just below the umbilicus [Table/Fig-1]. Provisional diagnosis made was urachal remnant malignancy or the carcinoma urinary bladder.
Computed Tomography of abdomen film showing urachal mass (arrow) attaching the bladder dome.
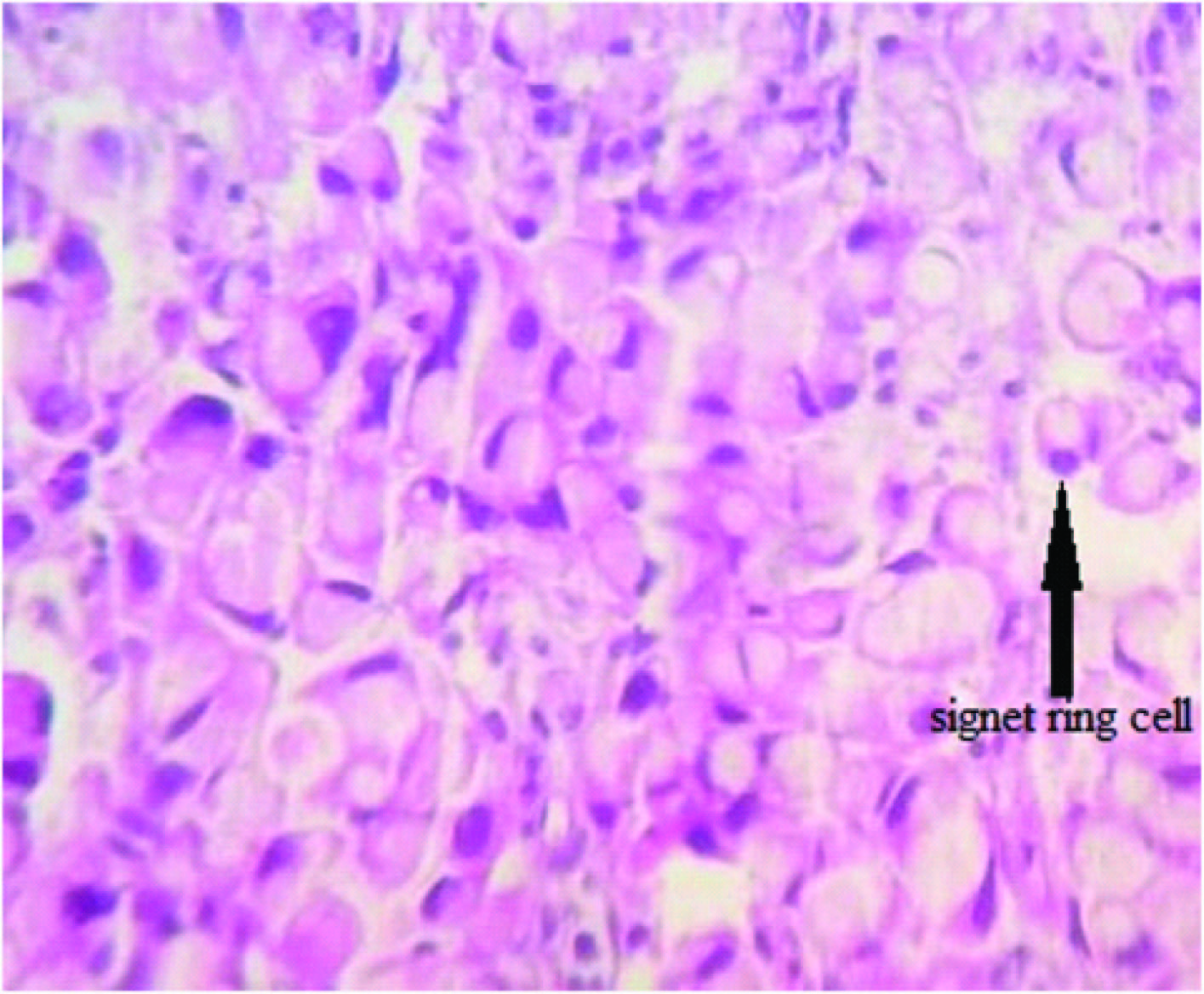
The patient underwent cystoscopic examination, which showed a mass on the dome and anterior wall of the urinary bladder. A biopsy was taken from the mass which showed signet ring cell carcinoma [Table/Fig-2].
Histopathological findings of the biopsy showing the tumour cells containing intracellular mucin-filled vacuole displacing the hyperchromatic nucleus to one side suggestive of signet ring cell carcinoma.
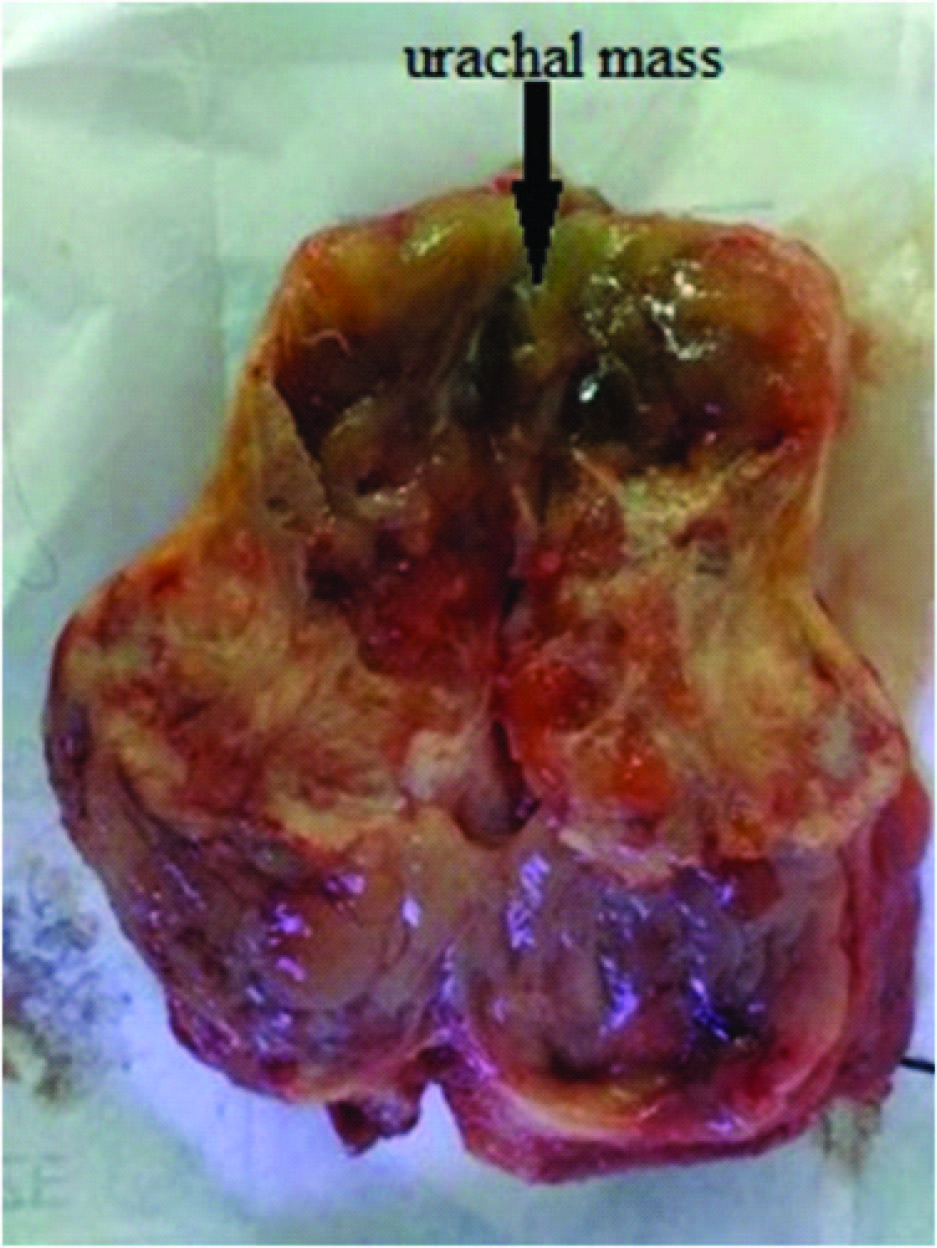
The patient underwent surgical exploration and a urachal mass extending up to the dome of urinary bladder and superiorly just below umbilicus was found. Radical cystectomy with en bloc excision of the urachal mass was done [Table/Fig-3] and orthotopic ileal neobladder was reconstructed. The patient is now doing well on regular follow-up.
Excised enbloc specimen of radical cystectomy (cut open) showing urachal mass (arrow).
Discussion
The urachus is a tubular structure connecting urinary bladder and the umbilicus. It has its origin from the regression of allantois during embryogenesis. After the third trimester, the urachus usually involutes as a fibrous cord [1]. However, a urachal remnant in the form of a tubular or cystic muscular structure can persist. It is most commonly found attaching the umbilicus to the bladder at the dome.
The urachal wall consists of the urothelium, subepithelial connective tissue and muscularis propria layers.
Urachal carcinomas are rare, accounting for less than 1% of all bladder cancers [2]. Although the urachal remnant has urothelium lining, most common carcinomas arising from it is adenocarcinoma. It has been postulated that the oncogenesis of urachal adenocarcinoma involve a metaplastic process, as the urachal urothelium often exhibits glandular metaplasia [3]. An alternative theory is that some urachal adenocarcinoma, particularly the enteric type, arises from the enteric rest left behind in the urachus from the cloaca during embryogenesis [4]. A small proportion of these tumours show signet ring cell type [5].
Hue and Jacquin in 1863 first described the urachal cancer [6]. Mostofi et al., in 1955 proposed the criteria that a malignant epithelial tumour situated in the dome or anterior wall of urinary bladder should be considered urachal if it is mostly intramural and is not a secondary carcinoma [7]. Since then various modifications for the diagnostic criteria of urachal carcinoma has been made. The most commonly used criteria are that of Johnson et al., which includes the following [8]:
Tumour in the dome or elsewhere in the midline of the bladder,
Sharp demarcation between the tumour and the surface epithelium, and
Absence of primary adenocarcinoma of another organ.
There had been very few case reports of urachal signet ring cell carcinoma in the literature. Morii et al., reported a case report of urachal signet ring cell carcinoma in a 65-year-old male whose chief complaint was haematuria [5]. Singh et al., reported 2 cases of urachal signet ring cell carcinoma and in both of them primary complaint of the patient was haematuria [9].
Haematuria or a suprapubic mass are the most common presenting complaints of the patients with urachal signet ring cell carcinoma [5]. When a patient presents with nonspecific symptoms like pain lower abdomen or irritative lower urinary tract symptoms as in our case, then a high index of suspicion is required because these symptoms are very common with benign conditions.
These tumours generally present as high grade, high stage tumours and have a uniformly poor prognosis and in the majority of cases there are regional or distant metastasis at the time of presentation [10]. But high index of suspicion and timely intervention as in our case can bring good outcome.
Conclusion
Signet ring cell carcinoma of urachus often presents as a high grade, high stage tumour and has a uniformly poor prognosis, but high index of suspicion and timely intervention as in our case can bring good outcome.
[1]. Dhillon J, Liang Y, Kamat AM, Siefker-Radtke A, Dinney CP, Czerniak B, Urachal carcinoma: a pathologic and clinical study of 46 casesHum Pathol 2015 46:1808-14. [Google Scholar]
[2]. Siefker-Radtke AO, Gee J, Shen Y, Wen S, Daliani D, Millikan RE, Multimodality management of urachal carcinoma: the M. D. Anderson Cancer Center experienceJ Urol 2003 169:1295-98. [Google Scholar]
[3]. Gopalan A, Sharp DS, Fine SW, Tickoo SK, Herr HW, Reuter VE, Urachal carcinoma: a clinicopathologic analysis of 24 cases with outcome correlationAm J Surg Pathol 2009 33:659-68. [Google Scholar]
[4]. Grignon DJ, Ro JY, Ayala AG, Johnson DE, Ordóñez NG, Primary adenocarcinoma of the urinary bladder: A clinicopathologic analysis of 72 casesCancer 1991 67:2165-72. [Google Scholar]
[5]. Morii A, Furuya Y, Fujiuchi Y, Akashi T, Ishizawa S, Fuse H, Urachal signet ring cell carcinomaInt J Urol 2007 14:360-61. [Google Scholar]
[6]. Hue L, Jacquin M, Colloid cancer of the anterior abdominal lombille and having invaded the bladder wallUnion Med de la Siene Inf Rouen 1863 6:418French [Google Scholar]
[7]. Mostofi FK, Thomson RV, Dean AL, Mucinous adenocarcinoma of urinary bladderCancer 1955 8:741 [Google Scholar]
[8]. Johnson DE, Hodge GB, Abdul-Karim FW, Ayala AG, Urachal carcinomaUrology 1985 26:218-21. [Google Scholar]
[9]. Singh D, Singh A, Jain S, Arora R, Hara GS, Garg L, Signet ring cell carcinoma of the urachusInt J Urol 2004 11:785-88. [Google Scholar]
[10]. Wood DP, Urothelial tumours of the bladder. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA. editorsCampbell Walsh Urology 2012 10th editionUSAElsevier:2309-34. [Google Scholar]