Chronic low back pain with or without sciatica due to prolapsed lumbar intervertebral disc is a common problem faced by the orthopaedic surgeons [1,2]. Damian Hoy and Christopher Bain, in their study, reported the global mean overall prevalence of low back pain to be 31.0% [2] with women and age group of 40-80 years having highest prevalence. It causes considerable disability and loss of work resulting in significant individual, social and economic burden worldwide.
All kind of conservative and surgical treatments have been used with varying success. Non-surgical treatment of chronic low back pain covers a wide range of alternatives including conventional physiotherapy, manipulations and other manual methods of traction. These conservative methods throw a considerable burden on general practitioners, surgeons and hospital outpatient department [3,4]. Surgical treatment in the form of excision has it’s own disadvantages like persistence of back pain, infection, postoperative adhesions and mechanical instability. Solberg et al., in their study, reported a 4% risk of worsening of symptoms after a lumbar discectomy [5].
The purpose of this study was to assess the functional efficacy of steroids via caudal, transforaminal and interlaminar epidural route and to compare their results. This will probably help to suggest most effective route of drug administration in alteration of pain and to establish treatment protocol for definitive or intermediary use.
Materials and Methods
A prospective study was done on patients suffering from back pain with or without radiation to lower limbs from December 2009 to March 2011. All patients were subjected to detailed clinical history and examination. X-ray and MRI of lumbosacral spine were done in every case. Those having a prolapsed lumbar disc as the cause of back pain were selected for the study. All selected patients were informed about the study. The patients who agreed were included in the study after signing a written consent. Thus, 152 patients were enrolled for the study.
The inclusion criteria for the selection of patients were: 1) Single or multiple level disc herniation diagnosed by MRI; 2) Signs and symptoms consistent with the nerve root irritation; 3) Failure after a minimum of 8 weeks of conservative treatment; 4) No history of lumbar surgery.
The patients excluded from the study were: 1) Migrated or sequestrated Herniation on imaging; 2) Motor deficit; 3) Cauda Equina syndrome; 4) Segmental instability; 5) Medical problems that contraindicated the procedure; 6) History of allergic reaction to local anaesthetic or corticosteroids; 7) Psychogenic disorders, tumours, malformation deformities, post traumatic root compression or infectious aetiologies. After selection for the study, 12 patients did not turn up for any treatment and hence were excluded from the study.
An approval of the ethics committee was taken and the procedures were in accordance of the standards mentioned in Helsinki declaration of 1975 and revised in 2000.
All patients were analysed according to the Japanese Orthopaedic Association Score [22] [Table/Fig-1,2] and were assigned a pre-injection score. Patients were then injected randomly in the epidural space by either caudal, transforaminal or interlaminar route [Table/Fig-3].
Japanese Orthopaedic Association (JOA) Score. A normal person has JOA Score of 29.
1. Subjective symptoms (9 points)
Low back pain None (3), occasional mild pain (2), frequent mild or occasional severe pain (1), frequent or continuous severe pain (0) Leg pain and/or tingling None (3), occasional slight symptom (2), frequent slight or occasional severe symptom (1), frequent or continuous severe symptom (0) Walking capacity Normal (3), Able to walk more than 500 metres although it results in pain, tingling and /or muscle weakness (2), Unable to walk more than 500 metres owing to leg pain, tingling and/or muscle weakness (1), Unable to walk more than 100 metres owing to leg pain, tingling and/or muscle weakness (0)
|
2. Objective findings (6 points)
SLR test Normal (2), 30° to 70° (1), < 30° (0) Sensory disturbance None (2), slight disturbance (1), marked disturbance (0) Motor disturbance Normal (grade 5) (2), slight weakness (grade 4) (1), marked weakness (grade 3) (0)
|
| 3. Restriction of ADL (14 points)Turn over while lying, standing, washing the face, leaning forwards, sitting (about one hour), lifting or holding heavy objects, walking:No restriction (2), moderate restriction (1), severe restriction (0) for each item |
| 4.Bladder function (-6 points)Normal (0), mild dysuria (-3), severe dysuria (-6) |
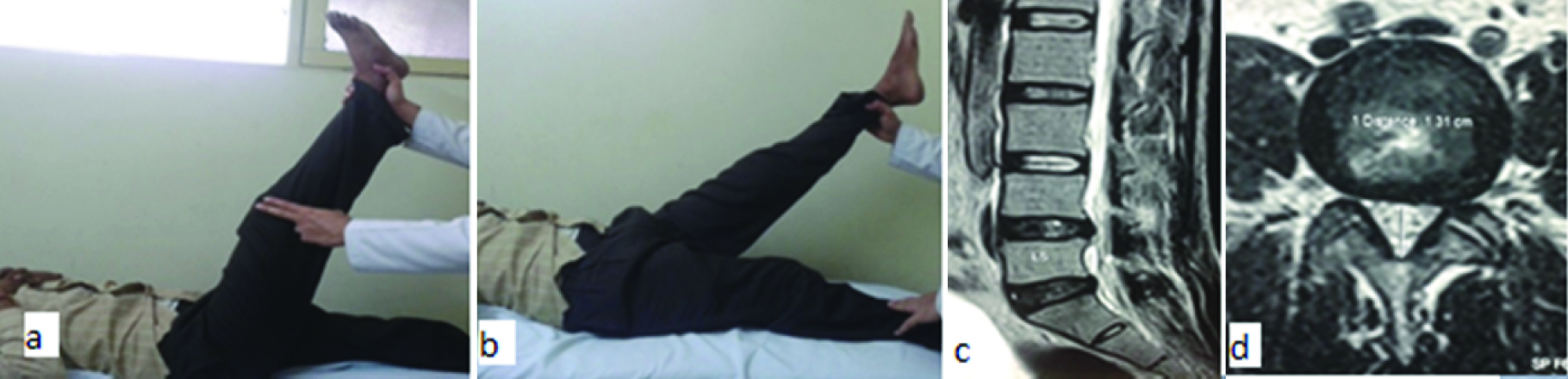
(a,b) Clinical picture of a patient showing SLR of 30 degree on left side; (c,d) MRI of the same patient, showing prolapse of L4-L5 disc and compression of L5 nerve root on left side.
Medication used in different injection techniques.
| Route of injection | Medication |
|---|
| Caudal route | Normal saline (26ml) + 2% xylocaine (2 ml) + methyl Prednisolone 80mg (2ml). |
| Interlaminar | 2% xylocaine (4 ml) + methyl prednisolone 80 mg (2ml). |
| Transforaminal | 2% xylocaine (1 ml) + methyl prednisolone 40 mg (1 ml). |
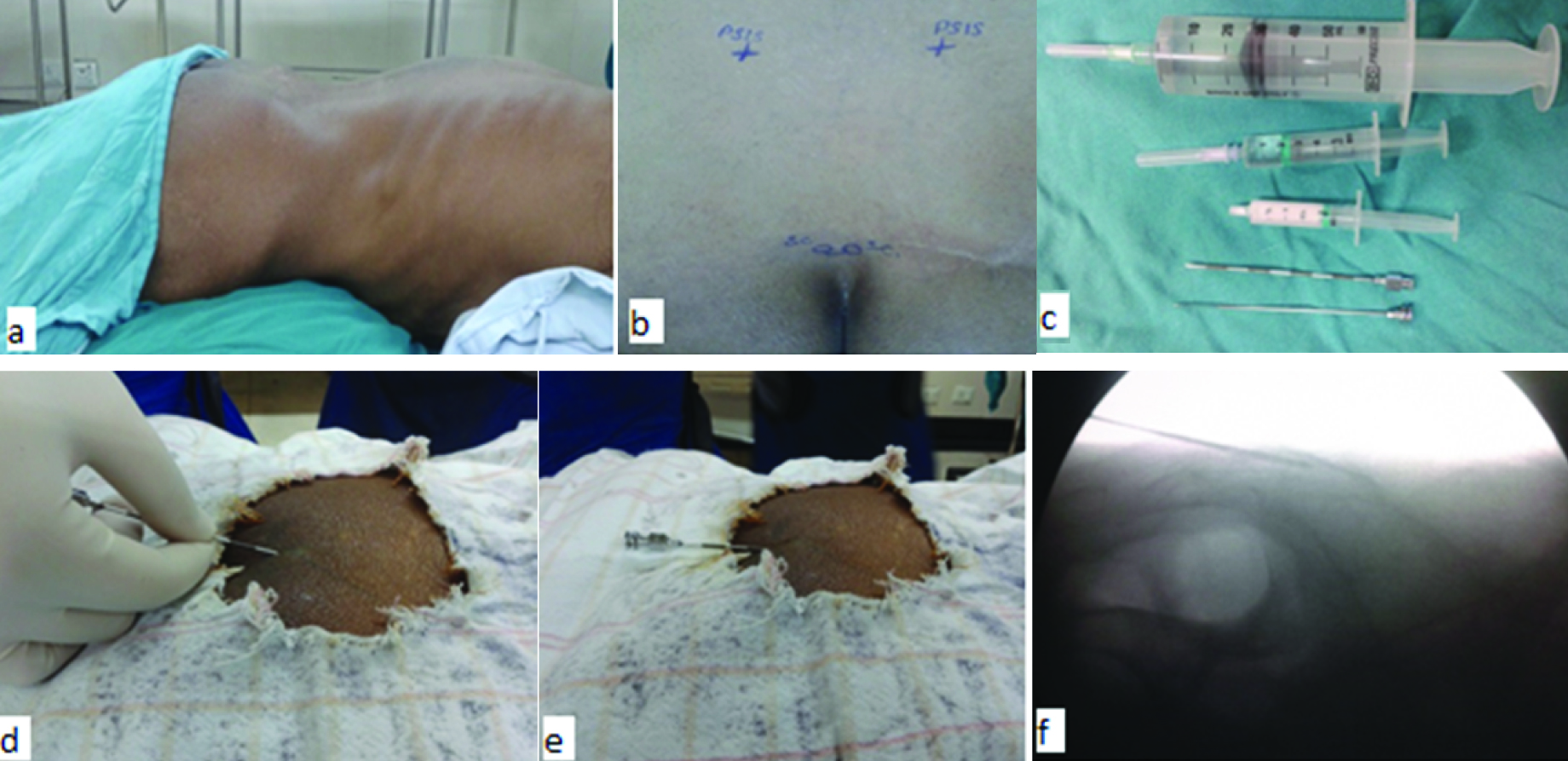
Caudal epidural injection [Table/Fig-4]: The patient was laid prone on the table and the sacral cornua were identified as two bony prominences on either side of midline of fourth sacral vertebrae. The gap between them indicates the position of sacral hiatus. After cleaning the area and superficial sterilization of the skin and subcutaneous tissue over the hiatus, the patient was injected with 1 ml of 2% lignocaine to produce local anaesthesia. The ordinary lumbar puncture needle, equipped with a stylet was then thirsted in just below the hiatus with an angulation of 45 degree to the surface until it reached the bone. It was then slightly withdrawn and made parallel to the surface and advanced further to enter the sacral canal. The position of the tip of needle in the canal was confirmed fluoroscopically by an image intensifier. The stylet was then withdrawn and care was taken that neither the cerebrospinal fluid nor blood escaped. Solution was injected at the rate of 5 to 10 ml/min. If blood vessel was punctured, the needle was withdrawn few mm and then the solution was injected. As the solution runs in, most patients feel some lower sacral aching, sometimes referred to back of both thighs. A sufferer of lumbosciatic syndrome nearly always states that the pain in the limb is reproduced first in the buttocks then in the thigh and leg. If the dural puncture occurred, the needle was withdrawn and the procedure was postponed for the next day.
Technique of caudal epidural injection: a) Prone position, b) Landmarks to find the sacral hiatus, c) 18 gauge Tuohy needle and medication, d) and e) Needle insertion, f) C-arm image showing the needle in sacral canal.
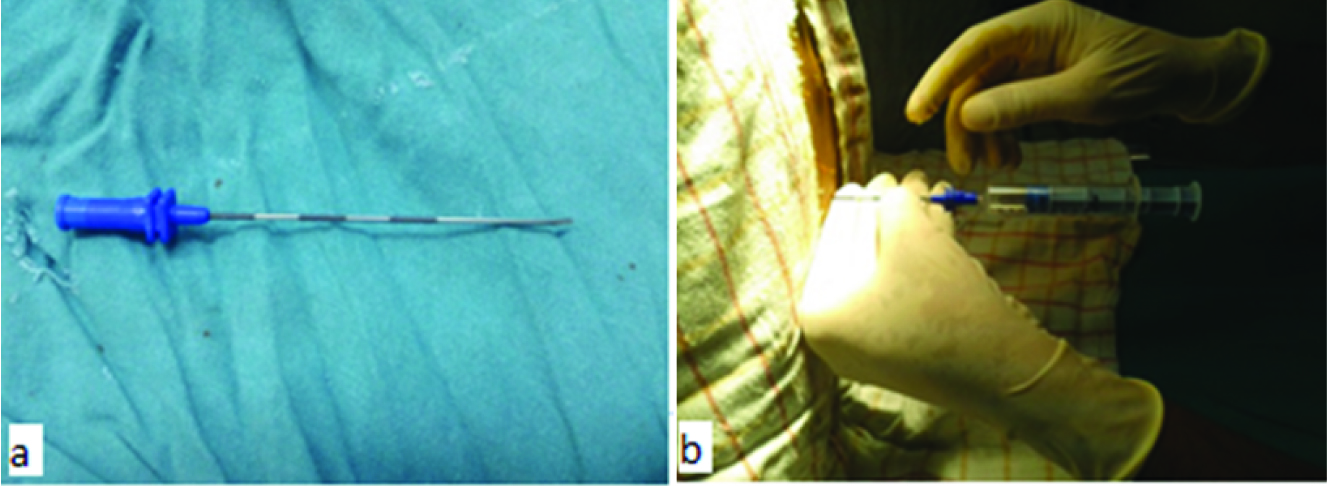
Interlaminar epidural injection [Table/Fig-5]: Interlaminar epidural injection was given in sitting position. The help of the anaesthetists in our institution was taken for this procedure. The local area was cleaned and sterilized. Spinous processes of the superior and inferior lumbar vertebrae were identified and the Tuohy needle was advanced through the ligaments, with the opening facing laterally. Confirmation of the space was made by the loss of resistance sign followed by confirmation by contrast medium injection. While injecting the solution, the needle was rotated through 90 degree either upwards or downwards depending on the area to be blocked.
Technique of interlaminar injection: a) Tuohy needle used for injection; b) confirmation of needle in the epidural space by loss of resistance sign.
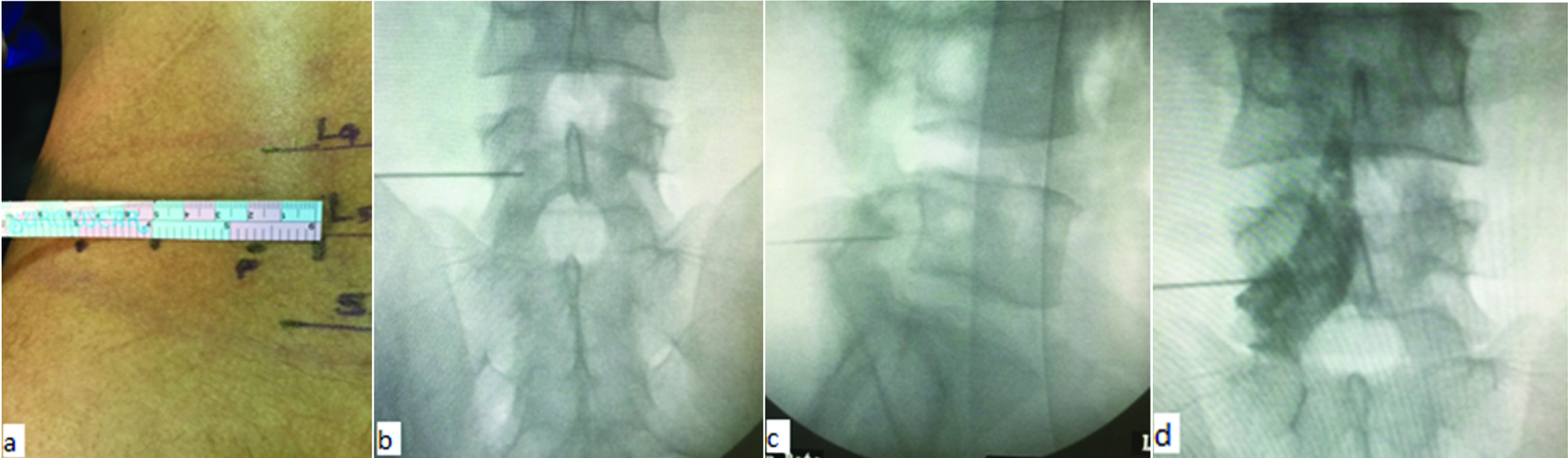
Transforaminal injection [Table/Fig-6]: The patient was laid in prone position on a radiolucent table. The involved neural foramen on the symptomatic side was approached by the posterolateral extrapedicular approach using an 18 gauge spinal needle. Under fluoroscopic guidance, the target site was located and the entry site was marked on the skin at a point between 5 to 8cm from the midline. After sterile preparation, draping and local anaesthesia, the spinal needle was inserted and the correct position of the tip of needle underneath the pedicle in the superior part of the foramina was confirmed on both AP and lateral fluoroscopic projections. A 1 to 2ml of isovist-300 was injected to visualize the posterior annular boundary and the corresponding nerve root. After an adequate flow of contrast medium to the target area has occurred and no blood or CSF was aspirated, the solution was injected.
Technique of Transforaminal injection: a) entry point marked between 5-8 cm from midline; b) and c) position of needle confirmed in AP and lateral views; d) radio-opaque dye spreading in the epidural space and staining the exiting nerve root.
Statistical Analysis
After the injection, patients were assessed at 1, 2 and 4week, 3 month, 6 month and 1 year. Results after injections were assessed according to the rate of improvement.
Rate of improvement (RI) = Post-injection score – pre-injection score / 29 – Pre-injection score × 100.
Accordingly, the results were classified as; Excellent (Rate of improvement 90% and above), Good (Rate of improvement of 75 – 89%), Fair (Rate of improvement of 50% - 74%) and Poor (Rate of improvement ≤ 49%). The cases with good, fair and excellent results were considered to be effective in relieving the pain by that route of medication. The patients who showed atleast 50% of improvement were injected again by the same route after 2 weeks. The total score was analysed by LSD and ANOVA method. The p-value was assessed in that particular group of epidural medication to know the efficacy in relieving the pain and to compare the effectiveness with other routes.
Results
A total of 152 patients were included in the study of which, 12 patients did not turn up for the procedure due to unknown reasons and hence 140 patients were considered for the interpretation of the findings of which 95 were males and 45 were females. The maximum patients were in the age group of 30 to 40 years. The patients were divided into three groups to receive epidural steroid injection by either caudal, transforaminal or interlaminar route, by the method of simple randomization (they were asked to pick a card from three labeled as C, T and I for caudal, transforaminal and interlaminar respectively). A total of 82 (58.5%) patients received steroid by the caudal route, 40 (28.5%) patients by transforaminal route and 18 (12.8%) patients by the interlaminar route. Because of the busy work schedule of the anaesthetists in our institution and hence their unavailability for the procedure, less number of patients received steroid through the interlaminar route. The average JOA score before injection and at successive visits is shown in [Table/Fig-7]. The highest average score was noted at 6 month after injection for all three groups.
Improvement in JOA score.
| Average JOA Score |
|---|
| Pre-injection | At 1 month | At 6 month | At 1 year |
|---|
| Caudal | 15.39 | 23.08 | 24.30 | 24.02 |
| Transforaminal | 15.57 | 24.42 | 26.65 | 26.55 |
| Interlaminar | 15.33 | 22.61 | 25 | 24.72 |
Response to the therapy in aspect of Rate of Improvement (RI) in JOA score at one year after injection is shown in [Table/Fig-8]. The transforaminal group gave the best results with 15 (37.5%) patients showing excellent, 16 (40.0%) showing good, 5 (12.5%) showing fair and only 4 (10%) showing poor rate of improvement.
Improvement in JOA score after one year in different groups of patients.
| Rate of improvement | Caudal | Interlaminar | Transforaminal |
|---|
| < 49% (poor) | 21(25.61%) | 4 (22.22%) | 4 (10.00%) |
| 50-74% (fair) | 31(37.80%) | 6 (33.33%) | 5 (12.50%) |
| 75-89% (good) | 22(26.83%) | 5 (27.78%) | 16 (40.00%) |
| 90-100% (excellent) | 08 (9.76%) | 3 (16.67%) | 15 (37.50%) |
The efficacy of the different routes of injection in relieving the pain was calculated accordingly [Table/Fig-9]. Transforaminal group showed the maximum improvement (90% of percentile improvement) followed by interlaminar group (77.7% of percentile improvement). Caudal group showed least percentile improvement of 74.3%.
Efficacy of improving JOA score after one year for different routes of epidural injection.
| Sr No | Route of injection | Effective | Not Effective |
|---|
| 1. | Caudal | 61 (74.39%) | 21 (25.60%) |
| 2. | Interlaminar | 14 (77.78%) | 4 (22.22%) |
| 3. | Transforaminal | 36 (90%) | 4 (1%) |
This data was subjected to statistical analysis using ANOVA and LSD technique. At 6 months, ANOVA method showed a significant difference in the rate of improvement of JOA score by all three different routes of injection with probability value (p-value) of 0.00 [Table/Fig-10,11]. When subjected to LSD, the analysis showed a significant difference in rate of improvement of JOA score between caudal and transforaminal route of injection having p-value of 0.00. It also showed significant difference between interlaminar and transforaminal routes with a p-value of 0.04. However, difference between caudal and interlaminar routes was shown to be insignificant with a p-value of 0.34.
Comparison at 6 months by ANOVA. (ANOVA – Analysis of Variance, df – Degree of freedom, F – Frequency, Sig – Significance).
| ANOVA |
|---|
| SCO_6M | Sum of squares | df | Mean square | F | p-value |
|---|
| Between groups | 147.943 | 2 | 73.972 | 9.159 | .000 |
| Within groups | 1106.478 | 137 | 8.076 | | |
| Total | 1254.421 | 139 | | | |
Comparison at 6 months: 1- Caudal group, 2- Interlaminar group, 3- Transforaminal group. LSD – Least Significant Difference.
| Multiple Comparisons |
|---|
| Dependent variable: SCO_6MLSD | 95% confidenceinterval |
|---|
| (I) GR | (J) GR | Meandifference(I-J) | Std. Error | p-value | LowerBound | UpperBound |
|---|
| 1 | 2 | –70 | .74 | .349 | –2.16 | .77 |
| 3 | –2.35* | .55 | .000 | –3.43 | –1.26 |
| 2 | 1 | –70 | .74 | .349 | –7.7 | 2.16 |
| 3 | –1.65* | .81 | .043 | –3.24 | –5.50E–02 |
| 3 | 1 | 2.35* | .55 | .000 | 1.26 | 3.43 |
| 2 | 1.65* | .81 | .043 | 5.50E–02 | 3.24 |
*The mean difference is significant at the .05 level.
At one year follow-up [Table/Fig-12,13], Once again, ANOVA showed a statistically significant difference between the JOA score of all three groups. LSD showed a significant difference in rate of improvement of JOA score between caudal and transforaminal route of injection having p-value of 0.00. It also showed significant difference between interlaminar and transforaminal routes with a p-value of 0.03. However difference between caudal and interlaminar routes was shown to be insignificant with a p-value of 0.36 [Table/Fig-14].
Comparison at one year by ANOVA (df – Degree of freedom, F – Frequency, Sig – Significance. ANOVA – Analysis of Variance).
| ANOVA |
|---|
| SCO_1Y | Sum ofsquares | df | Meansquare | F | p-value |
|---|
| Between groups | 171.59 | 2 | 85.880 | 9.992 | .000 |
| Within groups | 1177.462 | 137 | 8.595 | | |
| Total | 1349.221 | 139 | | | |
Comparison at one year. 1- Caudal group, 2- Interlaminar group, 3- Transforaminal group. LSD – Least Significant Difference.
| Multiple Comparisons |
|---|
| Dependent variable: SCO_1YLSD | 95% confidenceinterval |
|---|
| (I) GR | (J) GR | Meandifference(I-J) | Std. Error | p-value | LowerBound | UpperBound |
|---|
| 1 | 2 | –70 | .76 | .362 | –2.21 | .81 |
| 3 | –2.35* | .57 | .000 | –3.64 | –1.41 |
| 2 | 1 | –70 | .76 | .362 | –8.1 | 2.21 |
| 3 | –1.83* | .83 | .030 | –3.47 | –.18 |
| 3 | 1 | 2.53* | .57 | .000 | 1.41 | 3.64 |
| 2 | 1.83* | .83 | .030 | .18 | 3.47 |
*The mean difference is significant at the .05 level.
Significance (P-value), df – degree of freedom.
| StatisticalMethod | Comparison of the methods ofinjection | Mean difference | Standard error | p-value |
|---|
| 6 months | 1 year | 6 months | 1 year | 6 month | 1 year |
|---|
| LSD | Transforaminal and Caudal | 2.35 | 2.53 | 0.55 | 0.57 | 0.000 | 0.000 |
| Transforaminal and Interlaminar | 1.65 | 1.83 | 0.81 | 0.83 | 0.043 | 0.030 |
| Caudal and Interlaminar | -0.70 | -0.70 | 0.74 | 0.76 | 0.349 | 0.362 |
| ANOVA | Efficacy of steroid in improving JOA(Between all three methods. | Mean square | df | p-value |
| 6 months | 1 year | 6 month | 1 year | 6 month | 1 year |
| 73.972 | 85.880 | 2 | 2 | 0.000 | 0.000 |
Discussion
Initially, prolapsed disc was believed to cause back and leg pain by mechanically compressing the nerve roots. Now, it’s well known that leakage of the contents of the nucleus pulposus, causes pain producing an inflammatory reaction in the disc itself, around the facet joint and a chemical neuroradiculitis due to the synthesis of various inflammatory mediators [23]. Epidural steroids are believed to act by inhibiting the synthesis or release of the inflammatory substances thereby, reducing the intraneural oedema and venous congestion. The current literature reports conflicting results about their effectiveness in relieving sciatic pain. Abdi S, in his systematic review, found strong evidence for short term pain relief and moderate evidence for long term pain relief by use of epidural steroids [15]. Boswell et al., in their review found strong evidence for effectiveness of transforaminal epidural steroids while moderate evidence for caudal epidural steroids in reducing pain due to lumbar disc prolapsed [24]. Similar results were reported by many other studies [25,26]. However, some recent studies including some systematic reviews suggest conflicting results about their efficacy, leading to confusion among the treating physicians [27–30].
Controversy also exists regarding the most effective route of injecting the drug [Table/Fig-15]. Ackerman and Ahmed in their study reported the superiority of transforaminal route over caudal and interlaminar routes [31]. They also found that interlaminar route was better than caudal route. Contradictory to this, Laxmaiah Manchikanti and Vidyasagar Pampati [36] found no difference between the efficacy of these three routes.
Results of previous comparative studies.
| Study/year | Number ofpatients | Average age | Average follow-up | Results |
|---|
| William E Ackerman et al., 2007 [31] | 90 | 36.3 years | 6 months | The transforaminal route of epidural steroid placement is more effective than the caudal or interlaminar route. |
| Ivan Rados et al., 2009 [32] | 50 | 48.41 years | 6 months | Both interlaminar and transforaminal techniques are equally effective. |
| Sergio Mendoza-Lattes et al., 2009 [33] | 93 | 38.9 years | 24 months | Both caudal and transforaminal techniques are equally effective. |
| Babita Ghai et al., 2014 [34] | 62 | 44.4 years | 12 months | Both interlaminar and transforaminal techniques are equally effective. |
| Nayyaamat Sandhu et al., 2014 [35] | 40 | 42 years | 3 months | Both caudal and interlaminar techniques are equally effective. |
| Laxmaiah Manchikanti et al., 2015 [36] | 360 | 44.5 years | 24 months | caudal, interlaminar, and transforaminal routes are equally effective. |
| Rodrigo Rezende et al., 2015 [37] | 40 | 49 years | 3 months | Transforaminal technique is more effective than interlaminar technique. |
| Serbülent Gökhan Beyaz et al., 2016 [38] | 299 | 54.5 years | 12 months | Both interlaminar and transforaminal technique are equally effective. |
| Seyed Masoud Hashemi et al., 2015 [39] | 64 | 50 | 1 month | Both interlaminar and transforaminal technique are equally effective. |
| Present study | 140 | 35.37 years | 1 year | Transforaminal route was significantly more effective than caudal and interlaminar route. |
The current study was designed to measure the efficacy of epidural steroids in management of pain in patients with prolapse of lumbar intervertebral disc and to compare the effectiveness by three different routes of injection i.e. caudal, transforaminal and interlaminar. The drug was injected by the author through standard techniques mentioned in the literature under the guidance of an image intensifier.
In a recent study done by William E Ackerman and Mahmood Ahmad [31] on 90 cases of lumbar disc prolapse, 60 patients were male and 30 were female and average age of patient was 36.3 (18–60) years. Another study done by Hee Sun Jeong and Joon Woo Lee on 239 patients of lumbar disc prolapse was conducted consisting of 106 males and 133 females [13]. The average age of patient was 49.8 (13–82) years. Manchikanti et al., conducted a similar study on 360 patients in which 139 were male and 221 were female [36]. The average age of the patient was 44.5 ± 13.26 years. The average age of patient in our study was 35.37 (18–72) years. There were 95 male (67.85%) and 45 female patients (32.14%). The data showed that lumbar disc prolapse was more common in the age group of 30 to 40 years in both males as well as females with male to female ratio of 2:1. In other age groups male:female ratio was almost comparable.
The study of William E Ackerman and Mahmood Ahmad gave the following results after a follow-up of 1 year; Caudal group: complete pain relief in 3.33%, partial pain relief in 53.33%, no pain relief in 43.33% [31]. Interlaminar group: complete pain relief in 10%, partial pain relief in 50% and no pain relief in 40%. Transforaminal group: complete pain relief in 30%, partial pain relief in 53.33% and no pain relief in 16.66%. They concluded that transforaminal route was more effective than caudal or interlaminar route.
According to Manchikanti et al., 77% patients in caudal group, 72% patients in interlaminar group and 80% patients in transforaminal group showed significant improvement at the end of one year [36]. However, their analysis didn’t show any significant difference in efficacy of the three techniques of injection.
In our study, after a follow-up of 1 year, 74.39% patients in caudal group were relieved of pain while 25.61% still complained of significant pain. In the interlaminar group, 77.78% patients were relieved of pain while 22.22% showed no relief. In transforaminal group 90% patients were relieved of pain whereas only 10% patients didn’t show any improvement. A successful outcome was observed in 80% of the total patients enrolled. The JOA score improved in all three groups and highest score was achieved at 6 months after injection followed by a mild fall in score at one year. This study suggests that a transforaminal approach with an efficacy of 90%, offers benefit for increased analgesic efficacy when compared to the caudal or interlaminar approach. This may be due to increased ventral spread of steroid solution with better contact with the herniated disk and extruded contents. Caudal and interlaminar routes were found to be equally effective with no statistical difference between their outcomes with an efficacy of 74.3% and 77.7% respectively. The precise delivery of the medication at the exact site of pathology may be the reason for higher efficacy of the transforaminal route. With caudal and interlaminar technique, the solution spreads over entire epidural space with very less amount of steroid reaching the site of inflammation.
In addition to potentially differing efficacy, each method of doing a lumbar epidural steroid injection may have their own complication and hence maintaining a strict protocol during these procedures is mandatory. In addition to minor adverse reactions, major complications due to needle placement, steroid itself and other drugs used in the formulation has been reported. Dural puncture can cause headache and nausea after the procedure [25]. Also, subdural placement of the chemicals can lead to neurotoxicity [40]. Infection after the procedure although rare, is a possibility and strict asepsis should be maintained during the procedure. Histamine release from the contrast or steroid can cause sudden hypotension and hence an intravenous line should always be maintained prior to the procedure. For the caudal route, there may be an increased risk of needle tip placement anterior to the sacrum or into the rectum. However, the risk of puncturing the duramater is least with this method. The transforaminal method carries a risk of trauma to the nerve root during needle placement. This method also includes the risk of paraplegia if an inadvertent, intra-arterial injection of particulate steroid occurs into a radicular artery that reinforces the blood supply of the lower end of the spinal cord [41]. Furthermore, disk entry can be a complication of the transforaminal method as well as the interlaminar method.
Michel Benoist in his review study on efficacy and safety of epidural steroid injection has mentioned that epidural steroids are well tolerated and that most complications are due to a technical error [42]. Manchikanti et al., do not report any major adverse event in their study and assures the safety of the injection techniques [36].
In the current study, 15 patients from caudal group complained of sweating and transient drowsiness during the time of injection. Post injection hypotension was recorded in all these patients. These complaints were relieved by slowing down the speed of drug injection and by elevating the foot end of the operation table. None of the patients from interlaminar and transforaminal groups mentioned such complaint. None of the patients had an infection, headache or a reaction to contrast material and medication used. There was no incidence of an intravascular or a subarachnoid injection.
Patients in the current study had better improvement with repetitive injections. The reason for this observation is not known but it could be in part related to repetitive systemic steroid uptake from the epidural veins in the posterior epidural space as well as from blood vessels in the subarachnoid space after passive diffusion of steroid across the dura. Similar effect has been reported by previous studies (Machikanti et al., and Ackerman et al.,). Also, this result was obtained by giving only two injections as compared to older studies which mention an average of 3 to 4 injections [31,36].
Limitation
The limitation of this study was that, control group was not used in this study and both patient and physician were not blinded. Also, the results are in a small patient population (n=140) with a short follow-up period. A double-blind, placebo-controlled group was not used because the patients complained of severe pain, and a placebo injection would have been unethical in these circumstances. However, further studies on a larger population with a control group receiving placebo is recommended. Also, patients should be followed for a longer duration to see the long term clinical effects. The study could have targeted the affected nerve root as opposed to the site of the disk herniation, but our study design called for deposition of steroid in the epidural space as opposed to injecting the nerve root sheath. Another limitation of this study was that the volume of solution used was not identical for the three groups. However, because of the large volume of the epidural space in the sacral area, an increased volume in this anatomic area was chosen.
Conclusion
The management of low back pain and radicular pain due to a prolapsed lumbar intervertebral disk by injecting methyl prednisolone in epidural space is satisfactory in the current study. All three injection techniques are effective with the best results obtained by transforaminal route. The results obtained suggest a more rational use of the epidural steroid which should in turn give better results. It can be considered to be a good supportive and symptomatic treatment option and can avoid countless days of disability and unnecessary hospital stay. It is not a new technique but deserves a wider use and scientific assessment.
*The mean difference is significant at the .05 level.
*The mean difference is significant at the .05 level.