The Effects of Diclofenac Suppository and Intravenous Acetaminophen and their Combination on the Severity of Postoperative Pain in Patients Undergoing Spinal Anaesthesia During Cesarean Section
Fozieh Bakhsha1, Alireza Seyedi Niaki2, Seyed Yaghoub Jafari3, Zahra Yousefi4, Mohammad Aryaie5
1 Lecturer, Department of Anesthesia, Laboratory Sciences Research Center, Golestan University of Medical Sciences, Gorgan, Iran.
2 Anesthesiologist, Department of Anesthesia, Sayad Shirazi Medical & Education Center, Golestan Unaiversity of Medical Sciences, Gorgan, IR Iran.
3 Lecturer, Department of Anesthesia, Laboratory Sciences Research Center, Golestan University of Medical Sciences, Gorgan, Iran.
4 Lecturer, Department of Nursing, Laboratory Sciences Research Center, Golestan University of Medical Sciences, Gorgan, Iran.
5 Lecturer, Department of Epidemiology, Health Management and Social Development Research Center, Golestan University of Medical Sciences, Gorgan, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Fozieh Bakhsha, Lecturer, Department of Anesthesia, Laboratory Sciences Research Center, Golestan University of Medical Sciences, Gorgan, Iran.
E-mail: stu.yousefi@yahoo.com
Introduction
The main tasks of postoperative care are postoperative pain and complications control which play an important role in accelerating the recovery of patient’s general condition.
Aim
This study was performed in order to compare the effects of diclofenac suppository, intravenous acetaminophen and their combination on the severity of postoperative pain in patients undergoing spinal anaesthesia for cesarean section in Sayyad Shirazi teaching Hospital, Gorgon, Iran.
Materials and Methods
This was a double-blind clinical trial on 90 patients undergoing cesarean section. The patients were randomly divided into three groups, group A: 100 mg diclofenac suppository, group B: 1000 mg intravenous acetaminophen, group C: 100 mg diclofenac suppository and 500 mg intravenous acetaminophen. The same spinal anaesthesia circumstances were applied for all the participants. At the end of surgery, pain severity was assessed according to VAS scale at different times. Data were then analysed by SPSS 18 statistical software.
Results
The mean age of participants was (28.27±6.07). There was significant difference between the mean pain scores of the three groups before the intervention (p=0.018), which was considered as co-variate. This difference was more notable between the combination of acetaminophen – diclofenac group and diclofenac alone. After the intervention, significant difference was observed in mean pain severity between acetaminophen group and the combination group and also between diclofenac and the combination group. During the study, the least mean pain severity was found in the combination group and the highest was observed in the diclofenac group.
Conclusion
Results of this study indicates a significant effect of concomitant use of intravenous acetaminophen and diclofenac suppository on pain severity reduction and reducing the need for repeated doses of narcotics and prolonging the postoperative analgesia.
Pain management, Pain relief, Paracetamol, Postoperative complications
Introduction
Pain management is one of the most important aspects of postoperative care. According to previous studies, 80% of patients experience moderate to severe postoperative pain [1,2]. The pain causes unpleasant experiences such as prolongation of postoperative recovery and development of stress reactions. Pain-induced hypoxia by stimulating the sympathetic nervous system in body organs may lead to respiratory, gastrointestinal and renal disorders and consequently result in patient’s inability to perform activities, prolonged hospitalization, incapability of self-care and increase in healthcare costs [3]. Pain management has also been important in prevention of mortality, postoperative complications and is considered as the fifth vital sign [4].
Use of opioid analgesics for postoperative pain relief, is a base treatment, but it can also lead to frequent complications including respiratory depression, excessive sleepiness, decreased gastrointestinal motility, nausea, vomiting and spasm of the bile ducts [5]. Regarding the maternal care of caesarean section deliveries in the early hours after birth, pain management is necessary for communicating with the newborn and initiation of breastfeeding [6,7]. Due to the complications of opioids, recently physicians have focused on non-steroidal anti-inflammatory drugs (NSAID) for pain control [8,9]. Diclofenac is among the said category of drugs, effective in postoperative pain management and reducing postoperative narcotic demands [10–14]. Paracetamol is another NSAID which can be effective primarily in central nervous system through inhibition of cyclooxygenase and probably by indirect effects on serotoninergic system. It readily crosses the brain barrier and causes effective pain relief [14]. The results of previous studies have been variable regarding the degree of postoperative pain reduction through use of diclofenac and acetaminophen. Munishankar et al., studied 60 patient sanalgesics receiving who underwent abdominal gynaecological surgery, were divided into three groups of paracetamol, diclofenac and their combination were investigated, the results showed that demand for opioids in the paracetamol group was significantly higher than the other two groups while patients in the combination group experienced more effective analgesic. In terms of side effects there was no significant difference between the tested groups [15]. Akhvan Akbari studied, 120 patients undergoing elective cesarean section were investigated and the results showed that in terms of pain severity and opioid consumption, both groups of diclofenac and acetaminophen were significantly different from the control group while less morphine was used in patients receiving the combination of diclofenac and paracetamol compared to paracetamol-only [6]. Another study on the efficacy of diclofenac and paracetamol on postoperative pain after cesarean section indicated that diclofenac effectively improves postoperative pain and significantly reduces morphine consumption [16]. Pain relief is of great importance in patients with cesarean section deliveries by relaxing the mother, enhancing the ability of self-care, resulting into early discharge and subsequently reduces nosocomial infections and hospitalization costs. Due to disparities on the reported conclusions regarding the efficacy of acetaminophen and diclofenac and the mentioned importance of postoperative pain relief, this study aimed to investigate the effects of suppository diclofenac and intravenous acetaminophen administration and their combination on the severity of postoperative pain in patients undergoing spinal anaesthesia during cesarean section in Sayyad Shirazi teaching Hospital, Gorgan, Iran.
Materials and Methods
This study was a randomized, double-blind, clinical trial. Patient and drug injected was blinded (Patients were unaware of the existence of other groups and each suppository was placed in separate envelopes, uncoated surface for drug injected). After being approved by the Research Ethics Committee of the University and obtaining the written informed consent from participants the study was performed on 90 patients scheduled for caesarean section in Sayyad Shirazi teaching Hospital in city of Gorgan, North of Iran. (October 2014–August 2015).
Inclusion criteria included: 1) Age between 17 to 40 years; 2) Class I and II of American Society of Anaesthesiologists (ASA=1, 2); 3) Term pregnancy; 4) Lack of chronic diseases such as cardiovascular, hepatic and renal diseases; 5) Lack of drug addiction.
Exclusion criteria included: 1) Having an allergic history to a medicine like acetaminophen or local anaesthetics; 2) liver and renal disease; 3) Diabetes; 4) History of drug addiction; 5) Use of analgesic drugs (opioid, NSAID, corticosteroid) within the last 8-12 hours.
Intervention
Patients were randomly divided into three groups. Group A (30 patients) received 100 mg diclofenac suppository, Group B (30 patients) received 1000 mg acetaminophen through Intravenous injection of infusion in 200 ml 0.9% saline and Group C (30 patients) received 100 mg diclofenac suppository and 500 mg intravenous acetaminophen.
At the baseline, all participants were injected 5ml /kg of intravenous crystalloid fluids. The patients underwent spinal anaesthesia with the same technique and medicine, Marcaine (Bupivacaine % 0.5) without receiving any sedation, using No. 27 spinal needle in sitting position at L3-L4 and L3-L2 space by an anaesthesiologist. During the surgery, heart rate, oxygen saturation, systolic and diastolic blood pressures were monitored continuously for all patients. In the post-anaesthesia care unit, patients’ postoperative pain was evaluated by Visual Analogue Score (VAS) [17] and for all participants with moderate pain, medication interventions were performed according to the group classification. Intensity and duration of analgesia for patients were evaluated by VAS score in 0, 2, 4, 6, 12 and 24 hours after the surgery.
Ethical Considerations
This study received ethical approval from the institutional review board and the research ethics committee of Golestan University of Medical Sciences. All the participants signed a written informed consent before participation and were assured of the confidentiality of their personal information. They all also had the right to withdraw from the study at any time.
Statistical Analysis
The obtained data was analysed using SPSS version 18 and Chi-square and Fisher’s-exact tests were used to measure the differences between nominal demographic variables of the both groups. ANOVA, Bonferroni post-hoc statistical tests were then performed and p-value of <0.05 was considered as statistical significance.
Results
This study was performed on 90 eligible female candidates for cesarean section with a mean age of 28.27 ± 6.07. In terms of age, weight and duration of surgery, all the three study groups were similar and the ANOVA indicated no statistically significant difference [Table/Fig-1].
Demographic information and variables of three groups of study.
| Groups | AcetaminophenN= 30 | DiclofenacN = 30 | Aceta/DicloN= 30 | p-value |
|---|
| Mean Variables |
|---|
| Age(year) | 26.66±5.18 | 29.5±6.52 | 28.66±4.85 | 0.31 |
| Weight(kilogram) | 80.7±12.77 | 79.2±11.26 | 78.33±11.64 | 0.62 |
| Duration ofsurgery (minute) | 61.0±5.47 | 58.83±6.75 | 61.21±5.16 | 0.43 |
| Pain scoresafter anaesthesia(before) | 5.83±1.36 | 5.36±1.58 | 6.3±0.74 | 0.001 |
| Duration ofanalgesia(minute) | 407.5±56.18 | 209.34±45.31 | 988.0±96.71 | 0.001 |
| Times of additionalDose of analgesics | 1.43±0.16 | 3.13±0.21 | 0.56±0.13 | 0.001 |
Pain severity, duration of analgesia and frequency of analgesics intake of patients were studied and a significant difference between the mean pain intensity scores in the tested groups before the intervention was observed (p-value = 0.001). Bonferroni post-hoc tests also showed a difference between the combination of acetaminophen-diclofenac and diclofenac group (p-value = 0.018). Furthermore, there was a statistically significant difference between the acetaminophen and diclofenac with their combination of acetaminophen-diclofenac and diclofenac group, after intervention and controlling the confounding effects using variance test.
(Pain severity before the intervention and the additional number of received analgesic) (p-value = 0.002). However, there was no notable difference between the diclofenac and acetaminophen group.
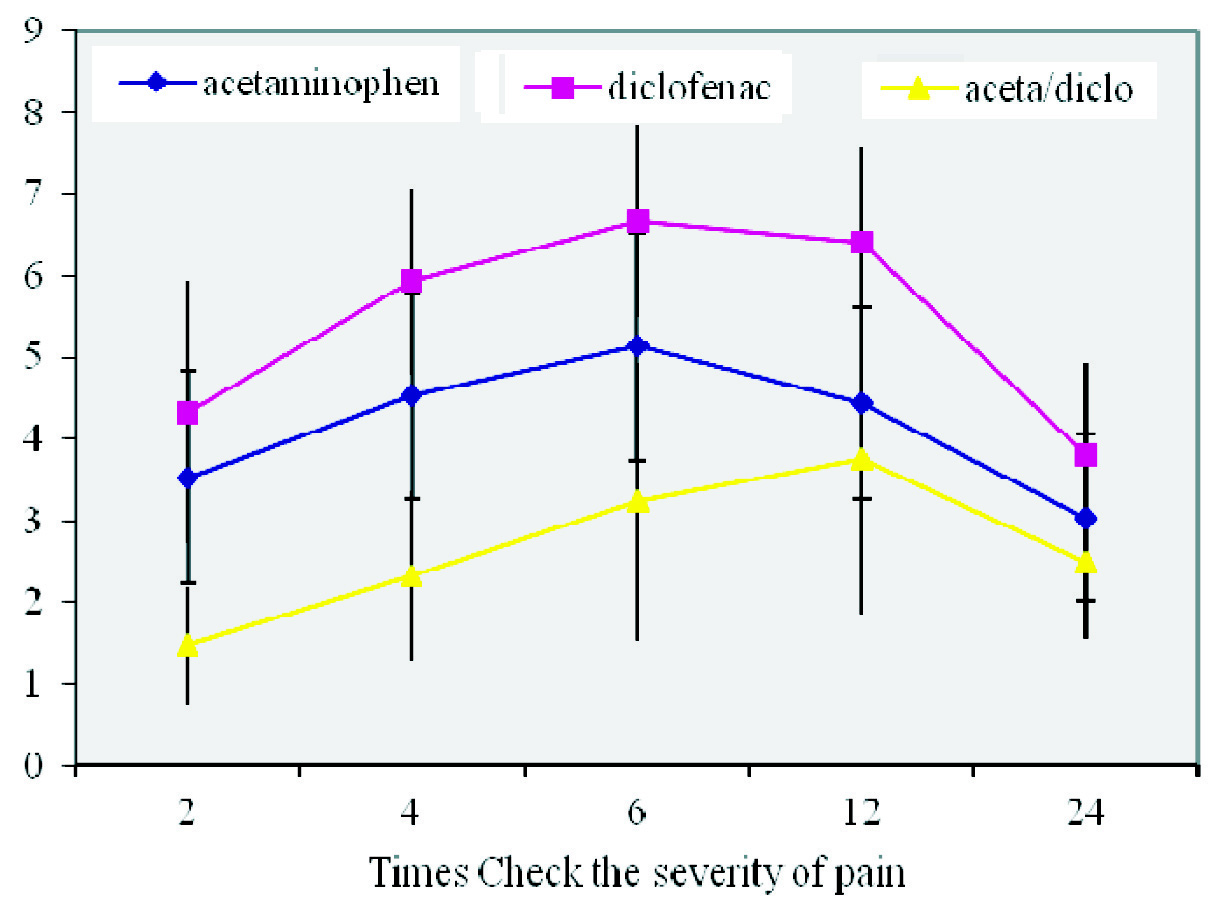
In terms of mean pain severity scores during the study, combined acetaminophen-diclofenac group had the lowest mean score and the highest mean score was found in the diclofenac group. Nevertheless, pain severity scores during 2, 4, 6, 12, 24 hours showed no statistically significant differences between the three tested groups.
The mean frequency of analgesic intake between the three groups was significantly different with the lowest frequency reported in combination group (0.56 ± 0.13) and the highest frequency of intake observed in the diclofenac group (3.13 ± 0.21) [Table/Fig-1].
Among all the study subjects, 28 patients in acetaminophen group (83.3%), 29 patients in diclofenac group (86.7%) and 13 patients in the combination of intravenous acetaminophen- diclofenac group received additional doses of analgesics. In this study, the duration of analgesia for the combination group was 4.7 times more than the diclofenac group and 2.4 times more than the acetaminophen group. While there was a significant difference between the acetaminophen/diclofenac group with the diclofenac and acetaminophen group (p-value = 0.001), no significant difference between diclofenac group and acetaminophen group was observed [Table/Fig-2,3].
Mean and standard deviation of pain severity scores in the study groups at different times post cesarean section after controlling for confounding (pain severity after anaesthesia or pain before intervention and opioid intake during surgery).
| Groups | AcetaminophenN=30 | DiclofenacN=30 | Aceta/dicloN=30 |
|---|
| Pain hours |
|---|
| 2th | 3.53±1.3 | 4.33±1.6 | 1.47±0.71 |
| 4th | 4.53±1.27 | 5.93±1.14 | 2.33±1.03 |
| 6th | 5.13±1.4 | 6.67±1.18 | 3.23±1.71 |
| 12th | 4.43±1.17 | 6.4±1.19 | 3.76±1.9 |
| 24th | 3.03±1.02 | 3.8±1.13 | 2.5±0.94 |
The pain score of the three tested drug groups at different times
Discussion
The study findings showed that among all the three studied groups, those who received the combination of acetaminophen and diclofenac experienced less pain, prolonged analgesia and less demand for repeated doses of analgesics. Combined intravenous acetaminophen and diclofenac suppository after cesarean section resulted in longer analgesia and better pain control compared with the other two study groups.
Study of Romsing et al., showed that the combination of acetaminophen and an NSAID has better analgesia than acetaminophen alone and the effect of NSAIDs combination is not better than a single type of NSAID [18]. Ong et al., also showed that using a combination of acetaminophen with an NSAID analgesic compared to the separate use of each drug is more effective [19]. Results of other similar studies also demonstrated the effectiveness of acetaminophen-diclofenac combination for reducing postoperative pain in patients after surgery compared to sole administration of acetaminophen [20ȃ22] which is in accordance to our results.
In Munishankar study patients receiving the combination of paracetamol and diclofenac required less morphine for pain control compared to the group that was administered paracetamol or diclofenac alone [15]. Results of a study showed postoperative intravenous paracetamol for tonsillectomy in adults with moderate to severe pain can improve it quickly [23].
In the meanwhile there are some studies indicating that the use of diclofenac alone is more effective to control postoperative pain in comparison with acetaminophen alone. Results of Sidik et al., done on 80 patients undergoing scheduled cesarean section in 4 groups, placebo, rectal diclofenac, intravenous paracetamol and paracetamol–diclofenac combination, showed less pain severity score and need for narcotics in patients receiving diclofenac while acetaminophen was less effective than the combination of diclofenac-acetaminophen [16].
Our findings showed the highest analgesia effect and the lowest need for analgesics was achieved through administration of acetaminophen and suppository diclofenac combination, while the shortest analgesia duration and highest need for analgesics was observed in the diclofenac group. Duration of analgesia in the combination group is 4.7 times more than the diclofenac group and 2.4 times more than the acetaminophen group. This difference can be due to the early onset and prolonged duration of analgesia with acetaminophen-diclofenac combination compared to acetaminophen or diclofenac alone.
In the matter of the side effects, some studies have shown that intravenous paracetamol activates the endogenous opioids pathway and thus has less adverse effects on the gastrointestinal tract, inhibition of platelet function and reaches to an effective concentration in a shorter time [24]. Clinically speaking, paracetamol is well-tolerated compared to other NSAIDs [25]. Due to its minimal side effects, NSAIDs are suitable for the treatment of moderate pain while for the reduction of postoperative pain paracetamol can be replaced by narcotics and reduce the postoperative need for opioids [26]. Although the mechanism of synergistic effects of this combination is still unknown, it is a suitable alternative for clinical pain management [22].
Diclofenac is one of the most potent cyclooxygenase enzyme inhibitors and by inhibiting the synthesis of prostaglandins it reduces inflammation and promotes peripheral analgesic effect [27–29]. It seems that the combination of these two together will cause better analgesic effects than using them separately and will have longer and more effective analgesia.
Conclusion
The combination of Acetaminophen and Diclofenac has better and longer analgesic effects than sole use administration of each drugs. Based on our study findings and previous similar studies, it can be concluded that this combination is able to provide a prolonged and effective analgesia for postoperative pain management of cesarean section with less side effects and stronger synergistic effects compared to other opioids, thus reduces the need for additional doses.
Funding/Support
This study was a research project funded by the Deputy of Research, Golestan University of Medical Sciences with the grant number of 35/3476. The registration ID in IRCT was IRCT201205099697N1.
[1]. Dahl JL, Gordon D, Ward S, Skemp M, Wochos S, Schurr M, Institutionalizing pain management: The post-operative pain management quality improvement projectJ Pain 2003 4(7):361-71. [Google Scholar]
[2]. Apfelbaum JL, Chen C, Mehta SS, Gan TJ, Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanagedAnaesthesia & Analgesia 2003 97(2):534-40. [Google Scholar]
[3]. Lee SY, Lee WH, Lee EH, Han KC, Ko YK, The effects of paracetamol, ketorolac, and paracetamol plus morphine on pain control after thyroidectomyKorean J Pain 2010 23(2):124-30. [Google Scholar]
[4]. Neugebauer EA, Althaus A, Simanski C, Acute pain managementRural Surgery 2011 Springer:67-75. [Google Scholar]
[5]. Cattabriga I, Pacini D, Lamazza G, Talarico F, Di Bartolomeo R, Grillone G, Intravenous paracetamol as adjunctive treatment for postoperative pain after cardiac surgery: a double blind randomized controlled trialEur J Cardiothorac Surg 2007 32(3):527-31. [Google Scholar]
[6]. Akhavanakbari G, Entezariasl M, Isazadehfar K, Kahnamoyiagdam F, The effects of indomethacin, diclofenac, and acetaminophen suppository on pain and opioids consumption after cesarean sectionPICR 2013 4(2):136 [Google Scholar]
[7]. Pakartadbiri S, Rahimi E, Comparison of morphine and piroxicam in decreasing post cesarean painSJKUMS 2001 5(3):3-10. [Google Scholar]
[8]. Banik D, Hye MA, Akhtaruzzaman A, Aziz L, Yeasmeen S, Iqbal K, Effect of small dose intermittent IV pethidine in combination with diclofenac for post operative pain reliefBangla JOL 2014 22(2):40-47. [Google Scholar]
[9]. Barkhori A, Drodian MR, Norozi M, Hashemi Shadmehri M, Shabani M, A comparative study of the effect of diclofenac, indomethacin, naproxen, and acetaminophen rectal suppositories on post-cesarean painJournal of Birjand University of Medical Sciences 2014 20(4):338-45. [Google Scholar]
[10]. Irer B, Gulcu A, Aslan G, Goktay Y, Celebi I, Diclofenac suppository administration in conjunction with lidocaine gel during transrectal ultrasound-guided prostate biopsy: prospective, randomized, placebo-controlled studyUrology 2005 66(4):799-802. [Google Scholar]
[11]. Ragavan N, Philip J, Balasubramanian S, Desouza J, Marr C, Javle P, A randomized, controlled trial comparing lidocaine periprostatic nerve block, diclofenac suppository and both for transrectal ultrasound guided biopsy of prostateJ Urol 2005 174(2):510-13. [Google Scholar]
[12]. Haq A, Patel H, Habib M, Donaldson P, Parry J, Diclofenac suppository analgesia for transrectal ultrasound guided biopsies of the prostate: a double-blind, randomized controlled trialJ Urol 2004 171(4):1489-91. [Google Scholar]
[13]. Dodd JM, Hedayati H, Pearce E, Hotham N, Crowther CA, Rectal analgesia for the relief of perineal pain after childbirth: a randomised controlled trial of diclofenac suppositoriesBJOG 2004 111(10):1059-64. [Google Scholar]
[14]. Ng A, Parker J, Toogood L, Cotton B, Smith G, Does the opioid sparing effect of rectal diclofenac following total abdominal hysterectomy benefit the patient?Br J Anaesth 2002 88(5):714-16. [Google Scholar]
[15]. Munishankar B, Fettes P, Moore C, McLeod G, A double-blind randomised controlled trial of paracetamol, diclofenac or the combination for pain relief after caesarean sectionInternational Journal of Obstetric Anaesthesia 2008 17(1):9-14. [Google Scholar]
[16]. Siddik SM, Aouad MT, Jalbout MI, Rizk LB, Kamar GH, Baraka AS, Diclofenac and/or propacetamol for postoperative pain management after cesarean delivery in patients receiving patient controlled analgesia morphineRegional Anaesthesia and Pain Medicine 2001 26(4):310-15. [Google Scholar]
[17]. Hawker GA, Mian S, Kendzerska T, French M, Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap)Arthritis Care Res 2011 63(S11):S240-52. [Google Scholar]
[18]. Rømsing J, Møiniche S, Dahl JB, Rectal and parenteral paracetamol, and paracetamol in combination with NSAIDs, for postoperative analgesiaBritish Journal of Anaesthesia 2002 88(2):215-26. [Google Scholar]
[19]. Ong CK, Seymour RA, Lirk P, Merry AF, Combining paracetamol (acetaminophen) with nonsteroidal antiinflammatory drugs: a qualitative systematic review of analgesic efficacy for acute postoperative painAnaesthesia & Analgesia 2010 110(4):1170-79. [Google Scholar]
[20]. Rahimi R, Abdollahi M, A systematic review of the topical drugs for post hemorrhoidectomy painInternational Journal of Pharmacology 2012 8(7) [Google Scholar]
[21]. Hyllested M, Jones S, Pedersen J, Kehlet H, Comparative effect of paracetamol, NSAIDs or their combination in postoperative pain management: a qualitative reviewBr J Anaesth 2002 88(2):199-214. [Google Scholar]
[22]. Miranda HF, Puig MM, Prieto JC, Pinardi G, Synergism between paracetamol and nonsteroidal anti-inflammatory drugs in experimental acute painPain 2006 121(1):22-28. [Google Scholar]
[23]. Atef A, Fawaz AA, Intravenous paracetamol is highly effective in pain treatment after tonsillectomy in adultsEur Arch Otorhinolaryngol 2008 265(3):351-55. [Google Scholar]
[24]. Ward B, Alexander-Williams JM, Paracetamol revisited: a review of the pharmacokinetics and pharmacodynamicsAcute Pain 1999 2(3):139-49. [Google Scholar]
[25]. Scharbert G, Gebhardt K, Sow Z, Duris M, Deusch E, Kozek-Langenecker S, Point-of-care platelet function tests: detection of platelet inhibition induced by nonopioid analgesic drugsBlood Coagul Fibrinolysis 2007 18(8):775-80. [Google Scholar]
[26]. Öncül AMT, Çimen E, Küçükyavuz Z, Cambazoğlu M, Postoperative analgesia in orthognathic surgery patients: diclofenac sodium or paracetamol?Br J Oral Maxillofac Surg 2011 49(2):138-41. [Google Scholar]
[27]. Lavand’homme P, Improving postoperative pain management: Continuous wound infusion and postoperative painEur J Pain Suppl 2011 5(S2):357-63. [Google Scholar]
[28]. Standing JF, Tibboel D, Korpela R, Olkkola KT, Diclofenac pharmacokinetic meta-analysis and dose recommendations for surgical pain in children aged 1–12 yearsPediatric Anaesthesia 2011 21(3):316-24. [Google Scholar]
[29]. Gan TJ, Diclofenac: an update on its mechanism of action and safety profileCurr Med Res Opin 2010 26(7):1715-31. [Google Scholar]