Penile Circular Fasciocutaneous (McAninch) Flap as an Option for Complex Anterior Urethral Stricture in Case of Non-Viable Buccal Mucosal Graft
Sundaramoorthy Vijayganapathy1, Ashwin Mallya2, Vilvapathy Senguttuvan Karthikeyan3, Jayaram Sreenivas4
1 Senior Resident, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
2 Senior Resident, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
3 Senior Resident, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
4 Assistant Professor, Department of Urology, Institute of Nephro Urology, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vilvapathy Senguttuvan Karthikeyan, 35-Second Cross, Thirumal Nagar, Pondicherry-605013, India.
E-mail: sengkarthik@yahoo.co.in
The penile circular fasciocutaneous flap (FCF) is employed in the successful single stage reconstruction of long segment complex anterior urethral strictures especially when buccal mucosa is unavailable due to various reasons. A 65-year-old gentleman, chronic smoker and tobacco chewer, hypertensive on treatment, presented with obstructive lower urinary tract symptoms for 8 months. He had no prior urethral catheterization. On examination, he had circumcised penis, with stenosis of the external urethral meatus. Glans had no changes suggesting balanitis xerotica obliterans. Suprapubic cystostomy was done as he developed acute urinary retention during evaluation. Retrograde urethrogram (RGU) showed pan-anterior urethral stricture. He was planned for substitution urethroplasty. On oral cavity examination, he had moderate trismus with oral submucous fibrosis. As buccal mucosal graft was unavailable, he was planned for FCF. A ventral onlay tubularization FCF urethroplasty from meatus to bulbar urethra based on dartos dorsal pedicle was done. His postoperative recovery was uneventful. Pericatheter RGU did not show extravastion and he voided well with Qmax 14 ml/second. He is doing well at follow-up.
Oral submucous fibrosis, Suprapubic cystostomy, Urethroplasty
Case Report
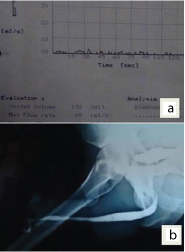
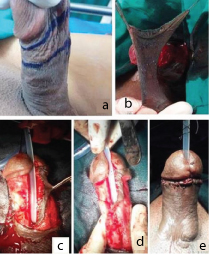
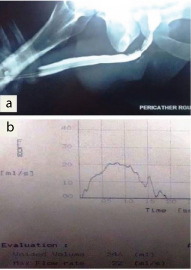
A 65-year-old male presented with the symptoms of lower urinary tract obstruction for 8 months. He was circumcised in infancy. He developed acute urinary retention and suprapubic cystostomy was done. Local examination revealed post circumcision status with stenosis of external urethral meatus. There was no evidence of lichen sclerosus et atrophicus. He was a chronic smoker and tobacco chewer, hypertensive on treatment. Oral cavity showed grade II trismus and submucosal fibrosis with tobacco staining. His blood urea was 31 mg/dl, serum creatinine 0.9 mg/dl and hemoglobin was 12 g/dl. His urine culture was sterile, ultrasound (US) showed no hydroureteronephrosis or prostatomegaly and uroflowmetry showed a flat pattern with Qmax of 3 ml/sec. Retrograde urethrogram (RGU) showed distal penile urethral stricture [Table/Fig-1a,b]. Patient was taken up for penile circular fasciocutaneous flap urethroplasty as his donor site for buccal mucosa was not available due to trismus and submucous fibrosis. Patient was placed in dorsal lithotomy under central neuraxial blockade. Circular penile skin flap was marked and a 1.4cm wide circumferential dartos based fasciocutaneous flap was harvested. The flap was 12cm in length after splitting dorsally. A ventral urethrotomy was made over the distal tip of the catheter and extended proximally until the normal caliber urethra is encountered. The most proximal and distal portions of the flap are secured to the normal urethra using interrupted 4-0 vicryl and flap suturing was completed [Table/Fig-2a-e]. Pericatheter RGU was done after 3 weeks and uroflowmetry showed a good flow [Table/Fig-3].
Preoperative uroflowmetry and retrograde urethrogram (RUG) showing long segment distal penile urethral stricture.
(a) Marking of skin flap; (b) Harvest of flap; (c&d) Flap suturing; (e) Final picture.
Postoperative pericatheter retrograde urethrogram and uroflowmetry.
Discussion
Penile skin flaps are of immense value in complex anterior urethral strictures as well as congenital conditions like hypospadias especially when surgical options are limited due to the complex nature of the disease, unfavorable conditions of the recipient site such as infection or precarious blood supply due to extensive fibrosis or lack of donor sites like oral submucous fibrosis [1–4].
Substitution urethroplasty has remained one of the standard methods for urethral reconstruction especially in difficult urethral strictures or when other modalities of treatment fail. Buccal mucsoal graft urethroplasty is usually employed in penile urethral stricture [5,6]. But, when buccal mucosal graft cannot be harvested due to disease or trismus as in our case, penile flaps come to rescue. A better understanding of the vascularity of penile flaps, broad and robust dartos-based flap, such as distal circum-penile flap, can be used with good short term and long term success [4,7].
The advantages of penile FCF are that they are well-vascularized, hairless, flexible up to 15 cm, can reach all parts of the urethra, cosmetic, not destroying sexual functions, possibility to do in single stage and can be done even in circumcised men [8]. Flaps have an obvious advantage over grafts because it does not depend on the blood supply of the recipient tissue which may be non-dependable in some situation because of associated severe spongiofibrosis and precarious blood supply [8,9]. Penile skin flap harvesting is technically more demanding and requires longer operating time. It is associated with more complications, such as penile skin loss, disturbed penile sensation, and less patient satisfaction [8].
Whitson et al., reported success rates of 95%, 89%, 84% and 79% at 1, 3, 5, and 10 years respectively in non-balanitis xerotica obliterans anterior urethral stricture [10]. In a series by Kim et al., the overall success rate was reported to be 55.6% in 20 cases operated using penile FCF [11]. The median follow-up was 19 months with a median flap length of 11.5 cm. In six patients, recurrence was identified at the junction of the FCF needing further surgical procedures like buccal mucosal graft urethroplasty, visual internal urethrotomy and urethral dilatation [11].
Long-segment anterior urethral stricture is difficult surgical challenge. Iatrogenic causes are commoner in the industrialized world while lichen sclerosus is the most common aetiology in India [12]. Our patient did not have lichen sclerosus. Single-stage, single perineal incision urethroplasty is gaining popularity due to its efficacy and reproducibility. The average stricture length in McAninch’s series was 24 cm and FCF was used as a tubularised on lay flap. The success rate with FCF alone was 79% and it was up to 95% successful when combined with tissue transfer or proximal graft placement. The major advantage is that it can be utilized from the membranous urethra to the external urethral meatus and recurrent strictures developed at proximal and distal anastomotic sites. The disadvantage was longer operating time leading to compartment syndrome in two cases [12]. We could complete the surgery in 129 minutes in our patient.
Conclusion
Circular penile fasciocutaneous flap urethroplasty has good and durable success in the treatment of complex anterior urethral strictures. It can be used from the membranous urethra to external urethral meatus up to 12-15 cm. This can be employed even in circumcised men.
[1]. Carney KJ, McAninch JW, Penile circular fasciocutaneous flaps to reconstruct complex anterior urethral stricturesUrol Clin North Am 2002 29(2):397-409. [Google Scholar]
[2]. McAninch JW, Reconstruction of extensive urethral strictures: circular fasciocutaneous penile flapJ Urol 1993 149(3):488-91. [Google Scholar]
[3]. Buckley J, McAninch J, Distal penile circular fasciocutaneous flap for complex anterior urethral stricturesBJU Int 2007 100(1):221-31. [Google Scholar]
[4]. McAninch JW, Morey AF, Penile circular fasciocutaneous skin flap in 1-stage reconstruction of complex anterior urethral stricturesJ Urol 1998 159(4):1209-13. [Google Scholar]
[5]. Dubey D, Kumar A, Mandhani A, Srivastava A, Kapoor R, Bhandari M, Buccal mucosal urethroplasty: a versatile technique for all urethral segmentsBJU Int 2005 95(4):625-29. [Google Scholar]
[6]. Dubey D, Vijjan V, Kapoor R, Srivastava A, Mandhani A, Kumar A, Dorsal onlay buccal mucosa versus penile skin flap urethroplasty for anterior urethral strictures: results from a randomized prospective trialJ Urol 2007 178(6):2466-69. [Google Scholar]
[7]. Gupta NP, Ansari MS, Dogra PN, Tandon S, Dorsal buccal mucosal graft urethroplasty by a ventral sagittal urethrotomy and minimal-access perineal approach for anterior urethral strictureBJU Int 2004 93(9):1287-90. [Google Scholar]
[8]. Morey AF, Tran LK, Zinman LM, Q-flap reconstruction of panurethral stricturesBJU Int 2000 86(9):1039-42. [Google Scholar]
[9]. Wessells H, McAninch JW, Use of free grafts in urethral stricture reconstructionJ Urol 1996 155(6):1912-15. [Google Scholar]
[10]. Whitson JM, McAninch JW, Elliott SP, Alsikafi NF, Long-term efficacy of distal penile circular fasciocutaneous flaps for single stage reconstruction of complex anterior urethral stricture diseaseJ Urol 2008 179(6):2259-64. [Google Scholar]
[11]. Kim KR, Suh JG, Paick JS, Kim SW, Surgical outcome of urethroplasty using penile circular fasciocutaneous flap for anterior urethral strictureWorld J Mens Health 2014 32(2):87-92. [Google Scholar]
[12]. Martins FE, Kulkarni SB, Joshi P, Warner J, Martins N, Management of Long-Segment and Panurethral Stricture DiseaseAdv Urol 2015 2015:853914 [Google Scholar]