An Innovative Technique for Columellar Reconstruction using ‘Flip-Over’ Buccal Mucosa Flap
Kapil S. Agrawal1, Raghav Shrotriya2, Mansi Pabari3
1 Additional Professor, Department of Plastic Surgery, KEM Hospital, Mumbai, Maharashtra, India.
2 Senior Registrar, Department of Plastic Surgery, KEM Hospital, Mumbai, Maharashtra, India.
3 House Officer, Department of Plastic Surgery, KEM Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghav Shrotriya, Senior Registrar, Department of Plastic Surgery, Gynecology Wing, 2nd Floor, KEM Hospital, Parel, Mumbai- 400012, Maharashtra, India.
E-mail: dr.raghav.s@gmail.com
Loss of columella is a significant deformity and its reconstruction proves to be quite difficult. An 18-year-old lady had loss of columella due to burn while steam inhalation at a young age and required reconstruction for the same. Labial mucosa has been used as a source of tissue for columellar reconstruction since long. We describe a modification of the buccal mucosal flap to manage a difficult case of columellar deficiency. The buccal mucosa flap was used to cover the columellar defect in the usual manner in the first stage and in second stage, along with division of the base, the residual length of the mucosal flap was used to add to the thickness of columella by doubling it on itself.
Columella, Nasal reconstruction, Rhinoplasty
Case Report
An 18-year-old female presented with right nostril stenosis, loss of columella and severe scarring on both alar facial groove and base of nose [Table/Fig-1,2] which she developed after columellar reconstruction was attempted in another hospital 2 years earlier, probably using perialar flaps (as suggested by operative scars). She had a history of loss of columella due to burn while steam inhalation at the age of 7 days. Subsequently, she required contracture release with chondro-cutaneous graft placement. As the patient still had severe deficiency of tissue in columella and starved of other options, authors chose to use a ‘flip over’ upper vestibular flap [Table/Fig-3].
Preoperative photograph (frontal view).

Preoperative photograph (basal view), showing right nostril stenosis, loss of columella and severe scarring on both alar facial groove and the base of nose.

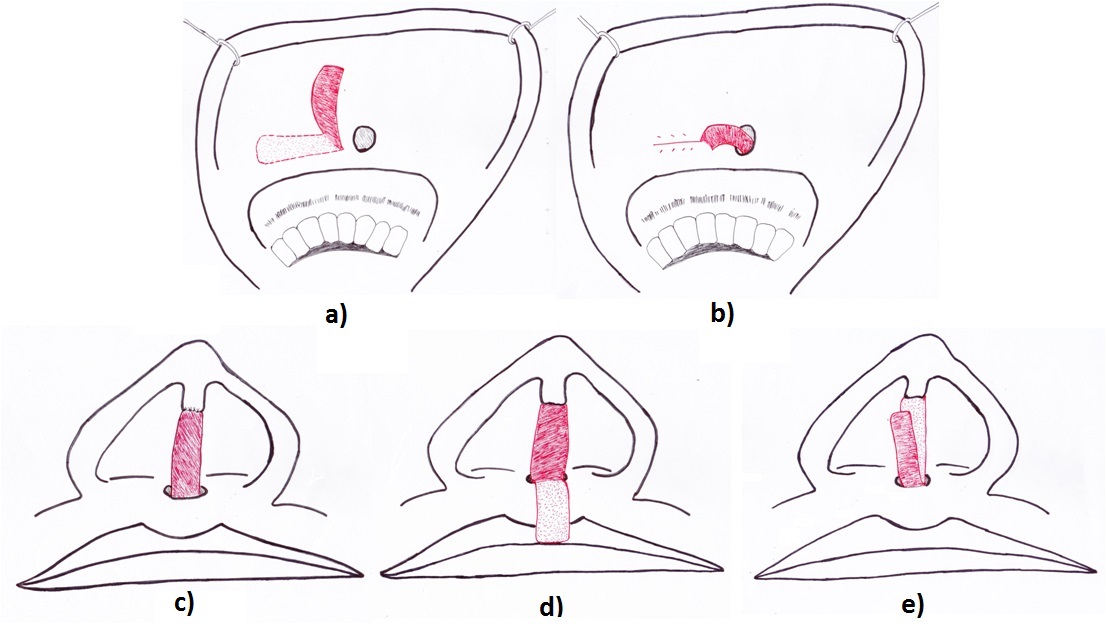
Schematic diagram of the technique (a): harvesting of buccal mucosal flap; (b): flap tunnelled at the base of columella; (c): flap inset over the columella; (d): upper mucosal flap divided at base and brought out of the tunnel by flipping over; (e): under surface of the doubled up flap de-epithelialized and inset over previous flap.
In the first stage, an upper vestibular mucosal flap was raised with base at the midline, tunnelled and transposed to the columella after being brought out through its base. The deficient lower part of the columella was de-epithelialized and the tunnelled buccal mucosal flap was inset over it [Table/Fig-4]. At second stage, after 4 weeks, instead of dividing at the junction of lip and columella, the flap was divided at the base in buccal sulcus by which about 1.5cm length of flap could be obtained. Raw area thus created in the upper sulcus was closed using vicryl 4-0.
The tunnelled buccal mucosal flap was inset over the deficient lower part of columella.

The flap was brought out through the same tunnel [Table/Fig-5]. It was de-epithelialized using a dermabrasion burr and the ‘flip over’ flap was sutured over the de epithelialized mucosa using vicryl 5-0. The flap healed well but had to be covered with a thin split thickness skin graft after 2 weeks when it developed healthy granulation [Table/Fig-6]. Presently, the patient has gained good columellar bulk and an appropriate length [Table/Fig-7,8] and will be posted for rhinoplasty soon for placement of columellar strut, alar reconstruction, tip plasty, and dorsal augmentation using author’s technique [1] for costal cartilage grafts.
The flap was brought out through the same tunnel.

Flap developed granulation.

Postoperative photograph (frontal view).

Postoperative photograph (basal view) showing good columellar bulk.

Discussion
From a surgical point of view, the nasal columella is an important aesthetic entity in the midface. A severe aesthetic deformity results from its loss or congenital absence. Though the size of skin flap needed to reconstruct columella is really small (1-1.5cm), it is a herculean feat to reconstitute the same without inflicting additional scars on face.
The need for tissue to place a graft for correction of cosmetic deformity is of paramount importance. Such patients may have a history of multiple procedures, which may finally leave the rhinoplasty surgeon with very few options. Multiple techniques have been described over the years for reconstruction of columella, though none has emerged as the treatment of choice [2].
Few procedures described for the reconstruction of columella are- The Ivy modification of the Blair procedure, the Dingman technique, V-Y advancement flap, the Brauer-Foerster technique, Ferris-Smith technique (use of full thickness skin graft (FTSG) buried below the upper lip skin), and the Cronin procedure. The use of composite conchal cartilage graft for columellar and alar rim reconstruction has also been reported [3,4]. Authors have reported occasional inferior aesthetic outcomes owing to the graft shrinkage resulting from central ischemic fat necrosis in subcutaneous layer [5]. FTSG has also been used for lengthening of shortened columella in cases of bilateral cleft lip patients, although skin grafts could produce several problems related to colour mismatch, depression, stepping, and unpredictable results [6].
Few other techniques, most of which have been described for columellar shortening as a part of secondary cleft lip nasal deformity are- forehead flap, tube pedicled flaps, upper lip flaps, forehead flaps, alar margin flaps, internal nasal vestibular flaps, labial mucosa flaps, nasolabial flaps, nasomalar flaps, nasal septal flaps, Abbé flaps and composite grafts from the earlobe. Recently microvascular composite free tissue transfer from ear has also emerged as a good option for reconstruction but requires microsurgical expertise [7]. Sherris et al., and Lejour et al., described the use of naso-facial sulcus flaps and prolabial flaps respectively for columellar lengthening [8,9]. All these procedures suffer from the bane of producing unsightly additional scars over the face.
In our patient, as there was paucity of usable tissue in the surrounding region owing to pre-existing surgical scars, we decided to use the buccal mucosal flap. Although this flap is not the first choice for columella reconstruction, it is easy to harvest and provide well-vascularised tissue.
Labial mucosa has been used as a source of tissue for columellar reconstruction since long. Tunnelled buccal mucosal flap has been described by Millard in his magnum opus, ‘Cleft Craft’. In 1931, Lexer described the use of labial mucosa flap which was tubed and brought out through an opening in the upper lip [10]. We raised a similar flap in the first stage and tunnelled it through the base of the nose. But the columellar defect being quite substantial, it was not enough. After 4 weeks, the patient was operated for flap division and rest of the flap was flipped over to add into the bulk of columella.
Conclusion
This modification of the standard upper buccal mucosa flap appears to be a useful choice in patients having significant columellar defect which is not amenable to reconstruction only by single layer of buccal mucosa flap, without inflicting additional scars over the face.
[1]. Agrawal KS, Bachhav M, Shrotriya R, Namaste (counterbalancing) technique: Overcoming warping in costal cartilageIndian J Plast Surg 2015 48:123-28. [Google Scholar]
[2]. Koh KS, Ock JJ, Columellar lengthening using the interdigitation of triangular flapsAesthetic Plast Surg 2002 26(2):78-80. [Google Scholar]
[3]. Son D, Kwak M, Yun S, Yeo H, Kim J, Han K, Large auricular chondro-cutaneous composite graft for nasal alar and columellar reconstructionArch Plast Surg 2012 39:323-28. [Google Scholar]
[4]. Cheon YW, Park BY, Long-term evaluation of elongating columella using conchal composite graft in bilateral secondary cleft lip and nose deformityPlast Reconstr Surg 2010 126:543-53. [Google Scholar]
[5]. Ahuja RB, Gupta R, Chatterjee P, Srivastava P, Securing aesthetic outcomes for composite grafts to alar margin and columellar defects: A long term experienceIndian J Plast Surg 2014 47:333-39. [Google Scholar]
[6]. Lee YS, Shin DH, Choi HG, Kim JN, Lee MC, Kim SH, Columella lengthening with a full-thickness skin graft for secondary bilateral cleft lip and nose repairArch of Plast Surgery 2015 42(6):704-08. [Google Scholar]
[7]. Mavili M E, Akyürek M, Congenital Isolated absence of the nasal columella: reconstruction with an internal nasal vestibular skin flap and bilateral labial mucosa flapsPlast Reconstr Surg 2000 106(2):393-99. [Google Scholar]
[8]. Sherris DA, Fuerstenberg J, Danahey D, Hilger PA, Reconstruction of the nasal columellaArch Facial Plast Surg 2002 4:42-46. [Google Scholar]
[9]. Lejour M, De Mey A, Primary lengthening of the columella in bilateral clefts of the lipCleft Palate Journ 1982 19(2):113-18. [Google Scholar]
[10]. Millard DR, Cleft craft: the evolution of its surgery in bilateral and rare deformities 1977 Vol IIBoston, MALittle, Brown:539-542. [Google Scholar]