Ultrasonography and serial estimations of serum Beta Human Chorionic Gonadotropin (hCG) are used to detect or exclude an Ectopic Pregnancy (EP) in women presenting with vaginal bleeding or abdominal pain in the first trimester. In more than two-third of EPs, serial hCG levels done 48 hours apart demonstrate either a suboptimal rise than in normal Intrauterine Pregnancy (IUP) or a fall in titres less than in a spontaneous miscarriage [1]. However, there are exceptions to the rules [1,2] and this has been our experience too in our day-to-day clinical practice.
Once diagnosed, the therapeutic approach to EP is dictated by several factors such as clinical condition, sonographic features, serum hCG, parity, desire for future fertility and willingness to return for regular follow-up. The treatment modalities include expectant, medical and surgical options; once commenced the decision to persist with expectant/medical management or resort to surgery subsequently is governed mainly by the patient’s symptoms and the serum hCG levels during the treatment phase. Of all the predictors of failure of medical management, hCG is the most important contributor [1].
The present study aimed to determine the trends of hCG levels in EP and to explore the role of hCG in decisions related to management and follow-up of EPs at an advanced tertiary care perinatal centre in southern India.
Materials and Methods
The study protocol adhered to the tenets of the Declaration at Helsinki. This was a retrospective review of case records. Women with serum hCG level >25 mIU/ml were identified from the laboratory database in the time period from January 2006 to December 2012 at Fernandez Hospital, Hyderabad, India. Those diagnosed with EPs or (persistent) pregnancies of unknown location were included in the study. Women with IUP, heterotopic pregnancy or gestational trophoblastic disease were excluded. A serum hCG level of 1,500 mIU/ml was considered as the Discriminatory Zone (DZ) with transvaginal sonography. Information on demographics and prior obstetric history, ultrasonographic features, laboratory investigations and surgical findings were accessed from the electronic database of medical records and entered into an MS Excel sheet. The trends of serial hCG values prior to diagnosis and during treatment were determined.
Management of EPs at the Study Institute
Asymptomatic women with serum hCG <5,000 mIU/ml, adnexal mass <3.5cm in size and absence of cardiac activity in the ectopic gestation were considered for medical management. Medical management was also offered to women who did not fulfil these criteria but insisted on this option after discussing risks and benefits. During the initial part of the study period up to mid-2009, medical management was administered in the form of intramuscular injection of methotrexate in a dose of 1 mg/kg body weight. Subsequently, the protocol was changed to intramuscular methotrexate 50 mg/m2 with or without oral mifepristone 600 mg. A second dose of methotrexate was considered if the fall in serum hCG was <15% between days 4 and 7 of the initial dose after ensuring that blood counts, liver and renal functions were normal. Once a satisfactory drop in hCG titres was recorded, the levels were checked every week until negative.
Expectant management (watchful waiting) was followed for asymptomatic women who had initial serum hCG <1,500 mIU/ml in whom the titres declined by >15% after 48 hours. Subsequently, serum hCG titres were assayed every week until negative. Surgical intervention was advised to those women with features suggestive of ruptured EP or those who did not meet the aforementioned criteria for medical management. Women receiving expectant or medical management who developed severe persistent abdominal pain or haemoperitoneum or showed no decline in hCG levels were also advised surgical intervention.
Results
There were a total of 337 patients in the study period and 37.4% were primigravidae. The mean (SD) age was 27.7 (±4.4) years. Thirty-seven (11.0%) women reported history of EP in the past and 38 (11.3%) conceived after undergoing treatment for subfertility. Eight cases (2.4%) resulted from failure of tubectomy.
Trends in Serum hCG
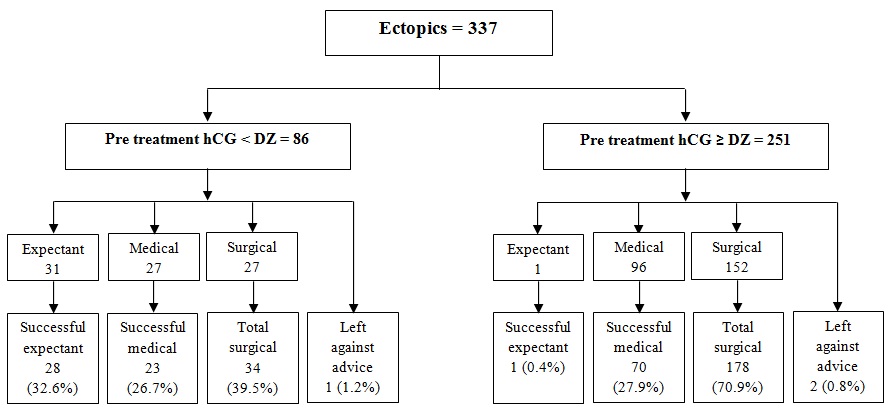
In 233 (69.1%) women, serum hCG was estimated only once; in the remaining 104, serial estimation of hCG with at least one set of values 48 hours apart was available for 71 (21.1%) women [Table/Fig-1]. In 23.9% of these women, there was a rise >53% similar to intrauterine pregnancy and 16.9% had a rapid fall >35%. Considering 1,500 mIU/ml as our DZ, 86 (25.5%) cases of EPs or pregnancies of unknown location had hCG levels below the DZ; the outcomes based on hCG are summarized in [Table/Fig-2].
Trends in serum Beta hCG estimations 48 hours apart in EP (n=71).
| Trend | Number (%) |
|---|
| Plateau (difference <15%) | 16 (22.5) |
| Decrease (>15%) | 19 (26.8) |
| Decrease followed by increase | 2 (2.8) |
| Increase (>15%) | 34 (47.9) |
Outcomes of ectopics based on hCG level in relation to discriminatory zone (DZ).
Role of Serum hCG in Management
[Table/Fig-3,4] depict the details of management. The average initial serum hCG among those that received medical management and had successful resolution was 3,351.1 mIU/ml versus 5,730.0 mIU/ml in those who subsequently went on to have surgery. Majority (n=201, 94.8%) of patients who underwent surgery were managed laparoscopically. Ten (4.7%) patients had laparotomy for scar/interstitial EPs or for haemorrhagic shock. One woman had hysteroscopic removal of cornual pregnancy.
Management of EP (n=337).
| ManagementNumber (%) | hCG pretreatment(mIU/ml) | Lost tofollow-up | Subsequentsurgery | Resolved | Resolutionof hCG(weeks) |
|---|
| Expectant32 (9.5) | 429.8 | 12 | 3 | 17 | 3.5 |
| Medical123 (36.5) | 3,866.2 | 27 | 30 | 66 | 4.5 |
| Direct surgical179 (53.1) | 12,961.5 | 8* | NA | NA | NA |
| Declined treatment3 (0.9)† | 3,408.0 | NA | NA | NA | NA |
* These were following conservative surgery
† Left against advice
Treatment of EP with relative contraindications for medical management (n=170).
| Management details | Serum BetahCG ≥5,000 =127 (37.7%)* | Adnexal mass≥3.5 cm = 55(16.3%) | Cardiacactivity = 40(11.9%) |
|---|
| Expectant management | 0 | 4 (falling trend of Beta hCG) | 0 |
| Direct surgery | 100 (78.7%) | 37 (67.3%) | 29 (72.5%) |
| Medical management | 26 (20.5%) | 14 (25.5%) | 11 (27.5%) |
| Surgery after medical management | 9 | 4 | 7 |
| Lost to follow-up after medical management | 6 | 3 | 3 |
| Success of medical management | 11/26 (42.3%) | 7/14 (50.0%) | 1/11 (9.1%) |
| Average time in weeks for resolution of Beta hCG | 5.5 | 3.1 | 8.0 |
*One patient left against medical advice.
In 170 (50.4%) women, the criteria for medical management were not fulfilled. However, upon patient’s choice, 43 of them were medically managed and success rates were 40% to 50% amongst those with hCG ≥5,000 mIU/ml and/or adnexal mass ≥3.5 cm. In women with cardiac activity, the success rates were low (9.1%) but the numbers were too low to draw conclusions.
Discussion
With the advent of high resolution transvaginal sonography and sensitive hCG assays, many EPs are diagnosed early [3]. DZ is the level of hCG above which an imaging scan should reliably visualize a gestational sac within the uterus in a normal IUP. EP is suspected if transvaginal sonography does not show an IUP and the hCG level is >1,500 mIU/ml [4]. However, EPs can be identified at lower hCG titres as was the case in 31 (9.2%) surgically confirmed EPs in our study, the lowest level being 122 mIU/ml. A considerable number of EPs can resolve spontaneously and treatment is not always necessary [3].
Traditionally, a doubling or rise in hCG level >66% has been regarded as indicative of a viable IUP and a suboptimal rise or static levels indicate possible EP. However, 15% of normal IUPs show a suboptimal increase and the minimum rise to predict normal viable IUP is 53% [5,6]. In fact, a rise in hCG as low as 35% can also indicate an IUP and it is prudent to repeat the test for the third time, particularly when the initial hCG levels are low [7]. A rapid decline in hCG levels is usually indicative of miscarriage, the minimum fall being 21-35% in 48 hours and if the fall is slower, the presence of an EP should be suspected [8]. In our series, 23.9% of women with EP presented with a rise (≥53%) similar to viable IUP and 3.0% had more than doubling of hCG levels; only 4.2% had a fall <21% while 16.9% had a rapid fall >35%. Silva et al., observed that 60% of women with EPs had an initial rise in hCG, 40% had an initial fall, 20.8% had a rise similar to viable IUP (similar to our findings) and 8% had a fall similar to complete miscarriage, and concluded that there is no single way to characterize the pattern of hCG for EPs [2]. Morse et al., demonstrated that the likelihood for misclassifying a pregnancy as abnormal based on serial hCG estimations was greater in the initial weeks of pregnancy when hCG titres were <500 mIU/ml [7].
Methotrexate treatment is successful in 78% to 96% of selected patients [9]. The relative contraindications for medical treatment, namely, adnexal fetal cardiac activity, adnexal mass size ≥3.5 (to 4)cm, initial hCG >5,000 mIU/ml as well as presence of haemoperitoneum, rapidly increasing hCG (>50% / 48 hours) before methotrexate and continued rapid rise in hCG concentrations during methotrexate therapy are all predictors of treatment failure [9–11]. The odds ratio of failure of treatment with initial hCG >5,000 mIU/ml is 5.45 (95% CI, 3.04-9.78) compared with values <5,000 mIU/ml [9]. We observed failure rates of 29.7% and 34.6% with hCG levels >4,000 and >5,000 mIU/ml respectively. The combination of mifepristone and methotrexate was effective in 58.3% of cases in comparison to 49.2% resolution rate with methotrexate alone. Our lower success rate of 53.7% with medical management could be due to inclusion of subjects (n=43) with relative contraindications and the proportion lost to follow-up (n=27, 22.0%). When these women were excluded, medical management was successful in 76.6% of the cases.
Expectant management is an option for clinically stable asymptomatic women with an ultrasound diagnosis of ectopic pregnancy and initial hCG of <1,000 mIU/ml with a decreasing trend subsequently [4,12]. We offered expectant management at hCG levels <1,500 mIU/ml and excluding those lost to follow-up, this was successful in 85.0% of them. A higher cutoff of 2,500 mIU/ml has also been used for expectant management in asymptomatic women, thereby avoiding unnecessary surgical interventions [3]. A falling trend of serum hCG may be indicative of resolution of an EP but by no means does it rule out the possibility of complications subsequently. Irvine and Padwick reported rupture of a tubal EP and haemoperitoneum following expectant management despite fall in hCG titres from 2,367 to 97 mIU/ml [13]. This emphasizes the importance of following up the hCG till it declines to a non-pregnant value.
Limitation
During the study, we identified some deviations from the protocol such as variable intervals between serial hCG estimations i.e. not equal to 48 hours (39, 11.6%), fixed 50 mg dose of parenteral methotrexate (12, 3.6%), <1 week interval between successive doses of methotrexate (15, 4.5%) and initiation of medical treatment with a single hCG value <1500 mIU/ml in asymptomatic women (14, 4.2%). The reasons for these aberrations were investigations performed elsewhere, inconclusive sonography and patient non-compliance. The other limitation of the study was the percentage lost to follow-up.
Conclusion
Modern management of ectopic pregnancy has resulted in new pitfalls and difficulties. Today, women with inconclusive initial scans are followed with algorithms involving serial hCGs, progesterone, follow-up scans and at times laparoscopy. No single level of serum hCG is diagnostic of an EP. Due to the frequent overlap of the hCG trends for IUP, EP and complete miscarriage, serial serum levels and sonographic examinations are necessary to differentiate between normal and abnormal pregnancies and to monitor resolution of EP once therapy has been initiated. Further, caution must be exercised before estimating hCGs too early on in the gestation as premature surveillance can lead to errors in management.