Endodontic Management of Type III Dens Invaginatus with an Open Apex
Kinjal Mahesh Gathani1, Srinidhi Surya Raghavendra2, Swati Wadekar3
1 Post Graduate Student, Department of Conservative Dentistry and Endodontics, Sinhgad Dental College and Hospital, Pune, Maharashtra, India.
2 Professor and Head, Department of Conservative Dentistry and Endodontics, Sinhgad Dental College and Hospital, Pune, Maharashtra, India.
3 Post Graduate Student, Department of Conservative Dentistry and Endodontics, Sinhgad Dental College and Hospital, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Srinidhi Surya Raghavendra, Professor and Head, Department of Conservative Dentistry and Endodontics, Sinhgad Dental College and Hospital, 44/1, Vadgaon Budruk, Pune, Maharashtra- 411041, India.
E-mail: srinidhi73@gmail.com
Apexification, Dens in dente, Dens invaginatus, Maxillary lateral incisor
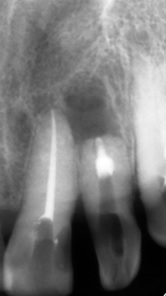
A 65-year-female reported to the Department of Conservative Dentistry and Endodontics for replacement of missing teeth. On complete oral examination, maxillary left lateral incisor was observed to be discolored with varied patterns on the enamel surface [Table/Fig-1]. Sensibility testing using an electric pulp tester confirmed the loss of vitality with the maxillary lateral incisor. A radiographic examination revealed the presence of a well defined radio-opacity extending from the enamel to the apex of the tooth with a diffuse radiolucency seen periapical to the immature apex [Table/Fig-2]. The enamel lined invagination extended till the middle third of the tooth while dentinal lining extended upto the apex. A diagnosis of type IIIB Dens Invaginatus (DI) along with an open apex and a periapical cyst was established.
Clinical pre-operative view.

Pre-operative radiograph showing the extent of the invagination.

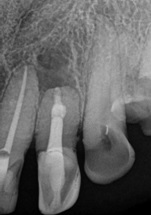
After explaining the treatment protocol and obtaining consent of the patient, the decision to eliminate the DI and carry out apexification for the tooth was made. After conventional access opening under rubber dam isolation, the white enamel lining of the DI was seen mesial and distal to the main canal. A #10 K file (Mani, Japan) was inserted to reach the apex from the canal space between the DI. The working length was determined using an electronic apex locator (Root ZX, J Morita, Japan) and confirmed with radiographs. Following this, an apical enlargement was done till #80 K file with 3% sodium hypochlorite (Prime Dental, Mumbai, India) as irrigant. However, the DI was not completely eliminated in this process. Hence, a Peeso reamer #3 (Mani, Japan) was used to remove the DI from the circumferential aspect [Table/Fig-3]. After radiographic confirmation of its complete elimination, calcium hydroxide dressing (RC Cal, Prime Dental, Mumbai) was given for a period of seven days following which apexification was carried out with an orthograde Mineral Trioxide Aggregate (MTA) (Angelus Soluções Odontológicas, Brazil) plug [Table/Fig-4]. Backfill was carried out with thermoplasticised gutta-percha using Obtura II (Obtura Spartan, Fenton, MO, USA) [Table/Fig-5]. On one year follow-up, satisfactory healing of the periapical lesion was seen [Table/Fig-6].
Elimination of dens invaginatus using peeso reamer.

MTA plug placement for apical barrier.
Post obturation radiograph.

Discussion
Clinically, the patients may be devoid of any clinical signs of the anomaly. However, important hints like atypical crown morphology (peg shaped or barrel shaped) or a deep foramen caecum may be present. Since coronal invaginations are most commonly found in maxillary lateral incisors they should be checked carefully, especially in all cases with a deep pit at the foramen caecum. If one tooth in a patient is affected, the contralateral tooth should be investigated. Early diagnosis is important to provide a prompt preventive treatment since teeth with coronal invagination have rapid pulpal involvement shortly after eruption, sometimes even before root end formation [1].
The DI acts like a portal for entry of irritants which may either be in communication with the pulp tissue or with a thin layer of enamel and dentin in between. Channels may exist between the invagination and the pulp, therefore early necrosis of pulp occurs within a few years of eruption, sometimes even before root end closure. In this case the invagination was removed to minimize the chances of re-infection from remnants of pulp tissue. In most cases, detection of DI is an incidental finding on the radiograph. Abscess formation, cysts or internal resorption are the other sequelae of undiagnosed and untreated coronal invaginations [1].
Different treatment options may be selected depending on the morphological complexity of the affected tooth. These include non-surgical endodontic treatment of the root canal and the invagination, a combined endodontic and surgical treatment, intentional replantation, or extraction. The first line of treatment with DI should always be nonsurgical. An unpredictable internal anatomy makes endodontic treatment of DI type II and III complicated [2].
A complete disinfection of the canal is essential to promote healing of affected periradicular tissues. In this case, sodium hypochlorite for irrigation and calcium hydroxide as intracanal medication, in between appointments, were used to obtain this result.
MTA has been proposed as a material for immediate closure of the apical opening instead of waiting for a natural healing process. This will create an apical barrier in the canal preventing the extrusion of root filling material into the periapical tissues. MTA induces the formation of a calcified matrix in the periapical tissue and regeneration of new cementum, possibly associated with its high sealing capacity, biocompatibility, alkaline pH, and liberation of substances activating the cementoblasts, which in turn will deposit a matrix for the cementogenesis [3].
The wide root canal space which resulted due to removal of invagination necessitated the obturation with a plastic filling material. In the present case, the thermoplasticizing technique facilitated this procedure and provided a more efficient sealing [4]. Knowledge of the existence, diagnosis and treatment options of teeth with developmental anomalies is very important for successful endodontic management. This case report shows that a type III B DI with an immature apex and a periapical lesion can be successfully treated by orthograde elimination and apexification.
[1]. Hülsmann M, Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerationsInt Endod J 1997 30:79-90. [Google Scholar]
[2]. Jaramillo A, Fernández R, Villa P, Endodontic treatment of dens invaginatus: a 5-year follow-up. OralOral Surg Oral Med Oral Pathol Oral Radiol Endod 2006 101(1):e15-21. [Google Scholar]
[3]. Torabinejad M, Pitt Ford TR, McKendry DJ, Abedi HR, Miller DA, Kariyawasam SP, Histological assessment of mineral trioxide aggregate as a root-end filling in monkeysJ Endod 1997 23:225-28. [Google Scholar]
[4]. Steffen H, Splieth C, Conventional treatment of dens invaginatus in maxillary lateral incisor with sinus tract: one year follow-upJ Endod 2005 31(2):130-33. [Google Scholar]