Where is the Blood Leaking From?
Chetan Devendra Rathi1, Nikita Lalitkumar Kabra2, Nirav Madhukant Pipaliya3, Meghraj Ananda Ingle4, Prabha Dilip Sawant5
1 Senior Resident, Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India.
2 Senior Resident, Department of Radiodiagnosis, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India.
3 Senior Resident, Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India.
4 Associate Professor, Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India.
5 Professor and Head, Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Chetan Devendra Rathi, Senior Resident, Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai-400022, India.
E-mail: cdrathi@gmail.com
Aorto-oesophageal fistula, Hematemesis, Pseudoaneurysm
A 50-year-old male patient was brought to emergency department with history of massive hematemesis associated with bleeding per rectum. He also gave history of progressive mechanical dysphagia since last 3 months. He had significant anorexia and weight loss during this illness. No other past surgical or medical history was present.
On examination, he had pallor with cold extremities and shock. Patient was transfused whole blood and resuscitated. Oesophago-gastro-duodenal endoscopy revealed a malignant appearing growth in the mid oesophagus [Table/Fig-1] and altered blood in fundus of the stomach. However, obvious source of bleeding could not be identified. Contrast enhanced computed tomography of the chest revealed a malignant thickening involving mid-part of the oesophagus and encasing descending thoracic aorta with a pseudoaneurysm arising from anterior wall of descending thoracic aorta leading to an aorto-oesophageal fistula [Table/Fig-23,4 and 5]. An immediate therapeutic vascular intervention was planned. However, patient had another bout of hematemesis and succumbed prior to any intervention.
Oesophago-gastro-duodenal endoscopy revealed a malignant appearing growth in the mid oesophagus.

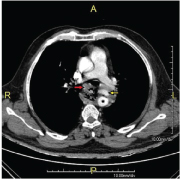
Contrast enhanced computed tomography of chest(axial image) showing malignant oesophageal thickening (red arrow), descending thoracic aorta (asterisk), and pseudo aneurysm (yellow arrow).
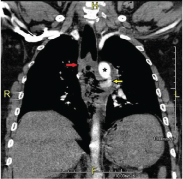
Contrast enhanced computed tomography of chest (coronal image)showing malignant oesophageal thickening (red arrow), descending thoracic aorta (asterisk) and pseudoaneurysm (yellow arrow).
Contrast enhanced computed tomography of chest (curved reconstructed image) showing descending thoracic aorta (asterisk) and pseudoaneurysm (yellow arrow).

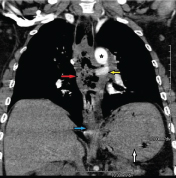
Contrast enhanced computed tomography of chest (curved reconstructedimage)showing malignant oesophageal thickening (red arrow), descending thoracic aorta (asterisk), pseudoaneurysm (yellow arrow), gastroesophageal junction(blue arrow) and stomach (white arrow).
Discussion
Aortoesophageal Fistula (AEF) is a rare but an important cause of life threatening massive bleeding with high mortality. The common causes are aortic aneurysm (54.2%), foreign body (19.2), malignancy (17%) and postoperative complication [1,2]. Endoscopy, contrast enhanced computed topography and conventional angiography have important role in diagnosis of AEF, its aetiology, localization of lesion and its relation with adjacent important mediastinal structures to plan surgical management [2].
Oesophageal malignancy is a rare cause of upper gastrointestinal bleeding with formation AEF as one of the cause for upper gastrointestinal bleeding in these patients. The probable mechanisms for AEF in oesophageal malignancies are thrombosis of vasa vasorum, invasion of adventitia by the tumour, bacterial infection or ulceration as tumour disintegrates [3]. Surgery is the ultimate modality of treatment for AEF, although associated with high mortality (25 to 90%). Endoscopic and endovascular treatment are other attractive options, however they should only be considered as a temporary measure to achieve short-term haemostasis and as a bridge to definitive treatment using conventional surgery within a few hours or days [2,4].
[1]. Ikeda Y, Morita N, Kurihara H, Niimi M, Okinaga K, A primary aortoesophageal fistula due to oesophageal carcinoma successfully treated with endoluminal aortic. stent graftingJ Thorac Cardiovasc Surg 2006 131(2):486-87. [Google Scholar]
[2]. Akin M, Yalcinkaya T, Alkan E, Arslan G, Tuna Y, Yildirim B, A cause of mortal massive upper gastrointestinal bleeding: aortoesophageal fistulaMed Arch 2016 70(1):79-81. [Google Scholar]
[3]. Lee RY, Flaherty L, Khushalani NI, Aorto-oesophageal fistula: a rare fatal case caused by oesophageal malignancyJ Gastrointest Oncol 2010 1:64-65. [Google Scholar]
[4]. Burks JA, Faries PL, Gravereaux EC, Hollier LH, Marin ML, Endovascular repair of bleeding aortoenteric fistulas: a 5-year experienceJ Vasc Surg 2001 34(6):1055-593. [Google Scholar]