In a developing country like India, the versatile technique of spinal anaesthesia has got a definitive and useful role. As the duration of spinal anaesthesia is relatively short lived, postoperative analgesia becomes an area of concern for the practicing anaesthesiologists. Postoperative pain has significant impact on the surgery outcome due to many adverse effects like tachycardia, hypertension, ischemia, reduced alveolar ventilation, poor wound healing and patient discomfort [1]. Hence, the alleviation of pain has been the priority of the medical profession and health authorities since time immemorial. Currently a multimodal approach is followed for treating postoperative pain which includes NSAIDs and opioids. A better understanding of the pain pathways and physiology led to the emergence of a new regimen known as preemptive analgesia. Preemptive analgesia was a concept developed by Crile and is a method of administration of medications before surgery in order to prevent the establishment of central sensitization of pain, thus reducing the intensity and duration of postoperative pain [2].
GABA analogues like pregabalin and its developmental precursor gabapentin are being used as preemptive analgesics [3–5]. As the orthopedic surgeries involve the manipulation of the bones, it can be really painful for the patients. Not many studies are available with pregabalin being used as a preemptive analgesic for lower limb orthopedic surgeries.
Hence, this study was undertaken to compare the efficacy of pregabalin in a dose of 150 mg with a placebo as preemptive analgesic in patients undergoing lower limb orthopedic surgeries under spinal anaesthesia.
Materials and Methods
The present interventional study was done in the Department of Anaesthesia, Sri Devaraj Urs Medical College, Tamaka, Kolar, India for duration of three months during June 2015 to September 2015. After obtaining Institutional Ethical Committee clearance, this prospective randomized double blinded comparative study was initiated. Ninety patients with ASA physical status I, II, aged between 18 – 50 years who were scheduled for elective lower limb orthopedic surgeries under spinal anaesthesia were enrolled in the study. The exclusion criteria were patients with known drug allergy to pregabalin or gabapentin, uncontrolled hypertension, diabetes mellitus, ischemic heart disease, cerebrovascular disease, renal and hepatic disease, history of alcohol and drug abuse. Patients with any general contraindications for spinal anaesthesia were also excluded from the study. Patients with chronic pain, neurological disorders and patients on NSAID’s and on other analgesics were excluded from study.
A detailed preanaesthetic assessment was done one day prior to the scheduled surgery. All the patients were provided with written information sheet about the drug and the anaesthesia technique. After obtaining written informed consent from the patient, they were educated about 0-10 centimeters of VAS (Visual Analogue Scale) which was to be used for pain assessment in the postoperative period [6]. All patients were kept nil per oral (NPO) for ten hours prior to the surgery. They were premedicated with Tab. Ranitidine 150mg and Tab. Alprazolam 0.25mg at night on the day before surgery. The patients were randomly allocated into two groups based on computer generated random number table. The patients were unaware as to which group they belonged to.
One hour prior to spinal anaesthesia: Group C - received colour matched empty capsules.
Group P - received 150mg of oral pregabalin.
The anaesthesia technique was standardized for both the groups. Baseline Heart Rate (HR), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), mean Arterial Blood Pressure (MAP) and SpO2 were recorded. All the patients were preloaded with Ringer Lactate 15 mL/kg iv and Inj. Ondansetron 50μg/kg i.v. was administered. Spinal anaesthesia was administered in sitting position in L3-L4 space with Inj. Bupivacaine heavy (0.5%) at a dose of 0.3mg/kg body weight with 20mg being the maximum dose using 25 gauge spinal needle. All the patients were catheterized with appropriate sized Foley’s urine catheter to monitor the urine output. All patients were administered oxygen via facemask at 4 liters/min. The study follow-up was done by another resident anaesthetist who was unaware as to which group the patient belonged to.
The patients were monitored during the course of the study for any incidence of:
Bradycardia (HR < 50bpm) which was treated with a dose of Inj. Atropine 0.6 mg iv.
Fall in the blood pressure (SBP < 20% of baseline), requiring bolus doses of Inj. Mephentermine 3mg iv.
Any adverse effects like nausea, vomiting, dizziness, sedation and blurred vision.
Sedation was assessed preoperatively by using Ramsay’s sedation score.
Postoperatively the patients were shifted to Post Anaesthesia Care Unit (PACU) for monitoring and observation. All patients were given Inj. Diclofenac 1.5mg/kg intramuscular as rescue analgesic once VAS exceeded 3. The patients were subsequently shifted to ward. Postoperatively one resident anaesthetist who was unaware as to which group the patient belonged to recorded the following data.
Time taken to two segment regression from the highest dermatomal level of sensory block (in minutes) was assessed by pin prick method.
Time to VAS >3 (time to rescue analgesics in minutes).
Total number of times VAS >3 in 24 hours duration.
Total dose of Inj. Diclofenac administered in 24 hours (in mg).
The patients were assessed fourth hourly for VAS score and for adverse effects like dizziness, sedation, blurred vision in the first 24 hours of postoperative period. The assessment was done by Resident Anaesthetist who was not aware of the study process.
At 24 hours postoperative period, a patient satisfaction score as adopted by Wichai Ittichaikulthol et al., was assessed. This is a numerical score ranging from 1-4 [7].
Poor
Fair
Good
Very good
Sample size was estimated based on the difference between proportions between placebo and study group from previous study [8]. At 0.01 alpha error and 99% power, sample size required was 39 in each group. Considering 10% dropout rate, final sample size needed = 39 + 4 = 43 subjects in each group. Thus we decided upon 45 subjects in each group.
Statistical Analysis
Data was entered into Microsoft Excel data sheet and analysed using SPSS 22 version software. Categorical data was represented in the form of frequencies and proportions. Continuous data was represented as mean and standard deviation. Independent ‘t’-test is the test of significance to identify the mean difference between two groups. The p-value <0.05 was considered as statistically significant.
Results
The groups were comparable with each other with respect to the demographic details and dose of bupivacaine (p >0.05) [Table/Fig-1].
Demographic details and dose of bupivacaine.
| Group P | Group C | p-value |
|---|
| Mean Age (in years) | 31.56 ± 9.41 | 32.49 ± 10.73 | 0.747 |
| Gender |
| Male | 36 | 37 | 0.788 |
| Female | 9 | 8 |
| Weight (in Kg) | 61.78 ± 6.32 | 62.49 ± 4.31 | 0.535 |
| Dose (in mg) | 18.31 ± 1.62 | 18.67 ± 1.22 | 0.244 |
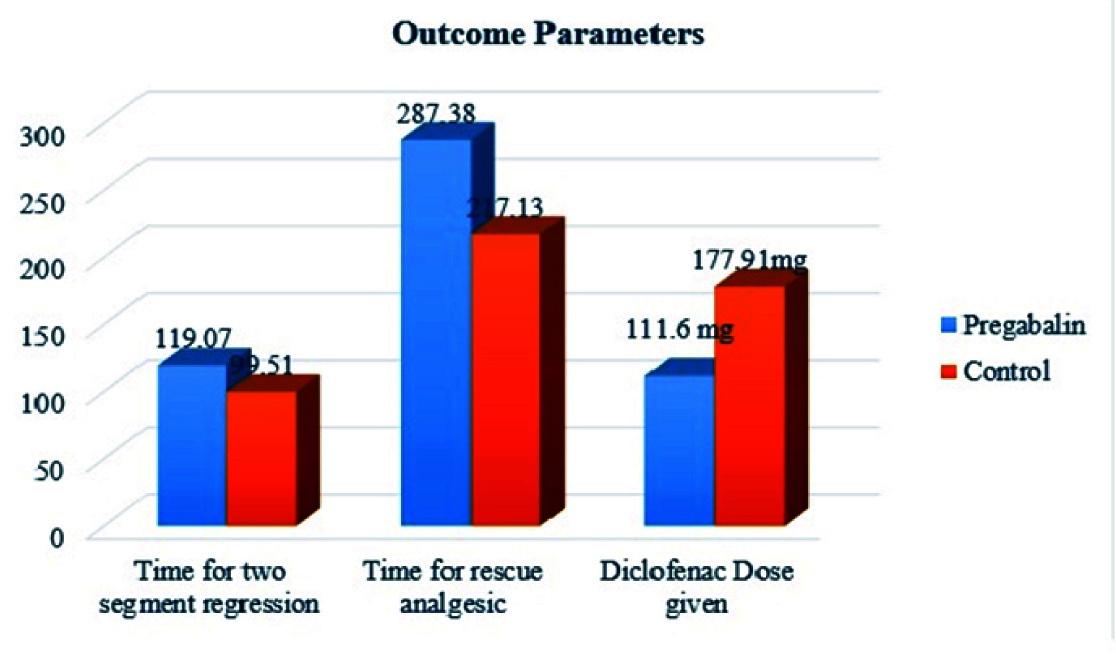
The mean time for two segment regression of sensory block was significantly increased in Group P (119.07± 5.81 min) when compared to Group C (99.51 ± 5.36 min). The mean time for rescue analgesic was significantly longer for group P compared to group C. The average diclofenac dose given to Group P and Group C for the first 24 hours post operatively was 111.60 ± 36.615 mg and 177.91 ± 39.694 mg respectively. There was a significant reduction in the total dose of diclofenac required in the Group P (p < 0.05) [Table/Fig-2].
Picture depicting the outcome parameters.
p <0.001 - time for two segment regression.
p<0.001 - time for rescue analgesic
p<0.001 - total diclofenac dose given
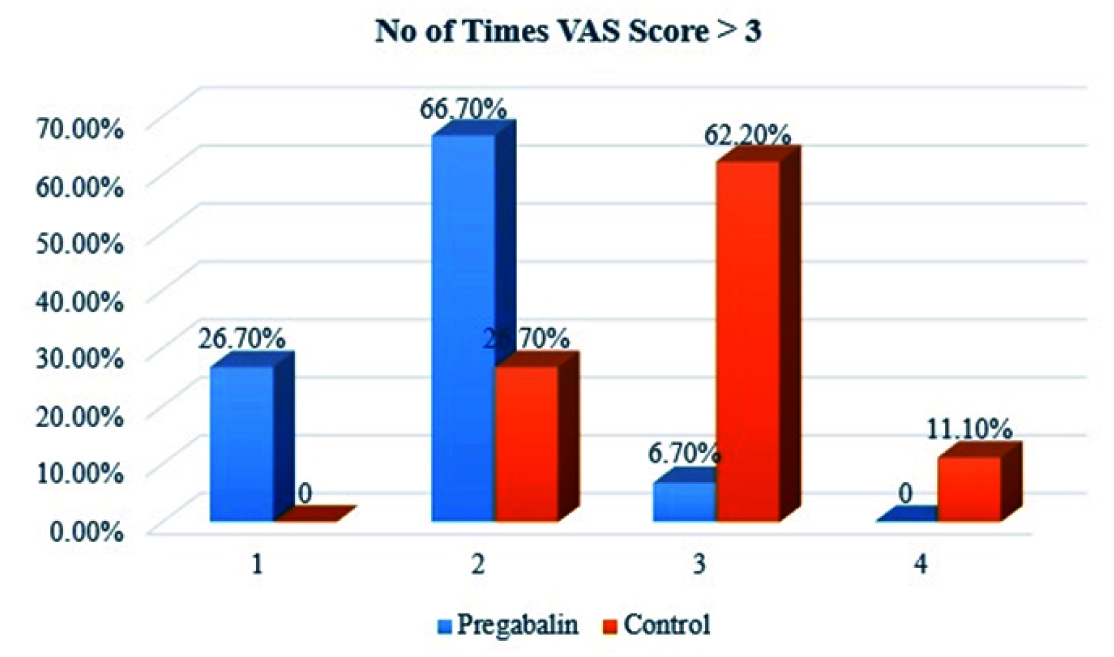
Majority of the patients of Group P had a VAS score > 3 only twice in the 24 hours of postoperative period (66.67%). On three occasions the VAS score was >3 in 62.2% of patients in Group C. Only 11.1% of Group C experienced a VAS score > 3 four times. Based on proportions, Group P patients experienced less number of times a VAS score > 3 than Group C [Table/Fig-3].
Bar diagram showing no of times VAS Score >3 between two groups.
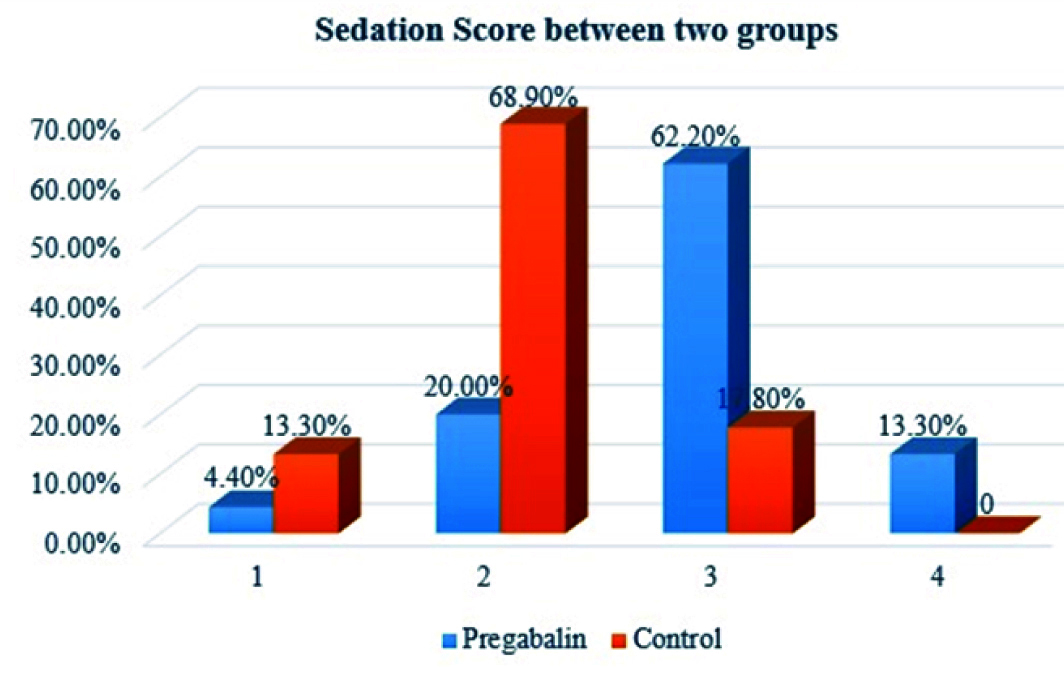
There was increased sedation scores in the Group P when compared to Group C in terms of the proportion of patients having a higher Ramsay sedation score [Table/Fig-4] 12 patients of Group P had dizziness (26.66%) while 1 patient in Group C had dizziness (2.2%). Fifteen patients of Group P (33.33%) had intraoperative hypotension which required Inj. mephenteramine 3 mg. 4 patients of Group C (8.88%) had fall in blood pressure which required treatment. No other complications were encountered in our study.
Bar diagram showing sedation score between two groups.
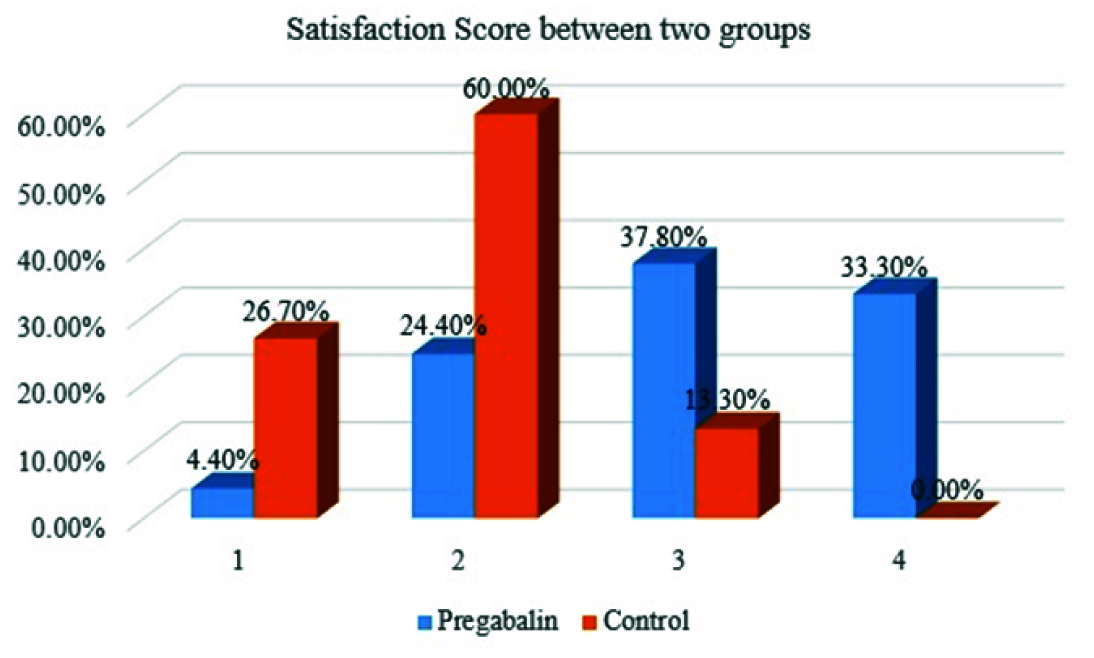
There was higher satisfaction score in Group P than in Group C as evidenced by the higher proportions of patients in Group P having scores of 3 and 4 (37.8% and 33.3% respectively) when compared to patients in Group C which has predominantly a score of 2 (60%) [Table/Fig-5].
Bar diagram showing satisfaction score between two groups.
Discussion
The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” [9]. Postoperative pain is a severe nociceptive stimulus associated hyperalgesia and allodynia which can exacerbate the existing pain by wind up phenomenon in dorsal column of spinal cord. Pregabalin is a lipophilic GABA analogue approved by FDA for clinical use. It is superior to other routinely used analgesics in that it reduces the anxiousness of the patient, is effective against neuropathic component of pain and is available at a reasonable cost. Pregabalin binds to the α2-δ subunit of voltage-gated calcium channels and modulate the release of several excitatory neurotransmitters such as glutamate, norepinephrine and substance P. Hence pregabalin reduces the hyperexcitability of the dorsal horn neurons of spinal cord that is induced by tissue damage and thereby decreases perception of acute postoperative pain [10]. Preemptive use of pregabalin helps in the control of postoperative pain by its anti allodynic and antihyperalgesic activity.
Pregabalin is being used for neuropathic pain conditions such as postherpetic neuralgia, painful diabetic neuropathy, central neuropathic pain and fibromyalgia. It has an additional use in partial seizures of temporal lobe epilepsy and generalized anxiety disorders in doses ranging from 75mg – 300 mg [10]. Few authors have noticed increased incidence of adverse effects when used in higher doses. Hence we limited the dose of pregabalin to 150 mg in our study.
Usha Bafna et al., did a study to compare the effect of oral gabapentin 600mg and pregabalin 150mg with control group for postoperative analgesia in patients undergoing elective gynecological surgeries. They concluded that preemptive use of gabapentin and pregabalin significantly reduces the postoperative rescue analgesic requirement with pregabalin being superior to gabapentin. They noted some adverse effects like nausea, hypotension and bradycardia associated with the drugs [11]. Our results were correlating with the above study in terms of reduced rescue analgesic requirement. The adverse effects noted were much less in our study.
Few authors compared pregabalin in a dose of 150mg and 225 mg for finding the optimal dose for patients undergoing abdominal hysterectomy. They found that though both were effective in prolonging postoperative analgesia. Pregabalin 225mg was associated with more adverse effects like dizziness. They arrived at a conclusion that pregabalin 150mg would be a better choice [8].
Few studies showed that a single preoperative oral dose of pregabalin 150mg is an effective method for reducing postoperative pain, opioid and NSAIDs consumption in patients undergoing orthopedic and abdominal hysterectomy surgeries [12–14]. These studies concentrated only on quantitative reduction of postoperative analgesic drugs. In our study extra effort was taken to assess the satisfaction of the patient as a whole which is of immense value to the anaesthetists in assessing the actual utility of such drugs in perioperative period.
Few authors studied pregabalin in various doses for gynaec laproscopic surgeries and laparoscopic cholecystectomy and found that preemptive oral pregabalin significantly decreases the postoperative pain as well as reduces analgesic requirement [15–17].
Another randomized study evaluating single preoperative dose of 100mg pregabalin concluded that it does not reduce acute pain nor improve recovery after minor surgery involving the uterus [18]. This showed that a preemptive oral pregabalin 100mg is insufficient in offering postoperative analgesia. In our study we used a dose of 150mg and it was effective in offering good postoperative analgesia.
Our study was correlating with the above studies in that pregabalin increases the time for rescue analgesia and reduces the total dose of analgesic requirement with better patient satisfaction and comfort. In our study we noted that the main complication was dizziness, hypotension and increased levels of sedation. These findings were in accordance with the side effects reported in previous studies.
In the present study, the sedative premedication given was Tab Alprazolam 0.25mg which has been used in both the groups to remove any confounding factors. Further, Alprazolam is a short acting with half life of 11 hours and drug was given 10 hours prior to study process. The dose used has been a very low dose which will not have any effect on the kinetics of the study drug being used. Hence it is unlikely to have any effect on the study drug being studied.
Limitation
There might be a limitation in our study, in that we used only one dose of oral pregabalin. But this was arrived at by analysing the observations of previous studies, in that increased doses had more adverse effects and lower doses were ineffective in offering analgesia.
Conclusion
Pregabalin administered preemptively offers effective postoperative analgesia reducing the analgesic requirement and yields higher patient satisfaction levels in patients undergoing lower limb orthopedic surgery without altering the intraoperative haemodynamics. Pregabalin can be an effective tool as a preemptive analgesic for the anaesthesiologist in the management of perioperative pain.