Sternal masses present a unique diagnostic challenge in clinical practice. A wide array of differential diagnosis of a sternal mass includes osteomyelitis, tuberculosis, eosinophilic granuloma, sarcoma and lymphoma (usually Non-Hodgkin’s) amongst others. Sternum is a rare site of Hodgkin’s lymphoma and is usually misdiagnosed as tuberculosis or eosinophilic granuloma on routine histopathology. This delayed diagnosis culminates in death of patients. We report a 30-year-old lady who presented with swelling in upper part of chest wall since 1 month. Past history was significant for a similar swelling 2 years back, which was diagnosed as hodgkin’s lymphoma and treated with 4 cycles of chemotherapy at another centre (which led to resolution of the swelling). Examination revealed a 6x6.5cm firm swelling originating from the upper part of sternum. There was no lymphadenopathy or organomegaly. Histopathological examination (with immunohistochemistry) of the trucut biopsy from the swelling confirmed the diagnosis of Hodgkin’s lymphoma (nodular sclerosis). Patient was diagnosed as a late relapse of primary sternal Hodgkin’s lymphoma (stage IBE) and was administered 4 cycles of ABVD followed by local radiotherapy to the involved site which led to complete resolution of the disease as assessed by PET scan. We present this unusual case of primary sternal Hodgkin’s lymphoma. Rarity of this entity, with diagnostic challenges encountered and treatment options available are highlighted in the current report. A pubmed search revealed 18 cases of sternal involvement in Hodgkin’s lymphoma which have been tabulated.
Chemo-radiotherapy, Immunohistochemistry, Tuberculosis
Case Report
A 30-year-old lady of Indian origin presented to our haematology clinic with complaints of swelling over the anterior chest wall of 1 month duration, associated with low grade fever (1000F) and significant weight loss (5kg over 1 month). She denied swelling in any other part of body, night sweats, cough or evening rise of temperature. Past history was significant for a similar swelling 2 years back which was diagnosed at a different centre as Hodgkin’s lymphoma (nodular sclerosis) after an open biopsy from the upper part of sternum. Patient was administered chemotherapy every 15 days, for a total of 8 courses (or 4 cycles, 2 courses per cycle). Records of staging and details of chemotherapy regimen were not available. No local radiotherapy was administered after chemotherapy. Swelling subsided following 4 cycles of chemotherapy and patient remained asymptomatic till the current presentation. She didn’t report back to the initial treatment centre in between.
On examination, the blood pressure was 120/76 mmHg and pulse was 74/minutes. General examination was not remarkable and there was no palpable lymphadenopathy. Chest examination revealed a midline swelling of approximately 6x 6.5cm in size originating from the upper part of the sternum. On palpation, swelling was fixed, firm and non-tender with smooth margins without any overlying erythaema or fistula. An old surgical scar mark of 3cm (from previous open biopsy) was visible. Per abdomen examination revealed no organomegaly and rest of the systemic examination was unremarkable. Patient’s blood test’s were as follows - Hb-100gm/L, white cell count- 12x109/L, differential counts- 70% neutrophils, 25% lymphocytes, 5% eosinophils, platelet count- 350 x 109/L, ESR -20mm/hour and LDH - 250U/L.
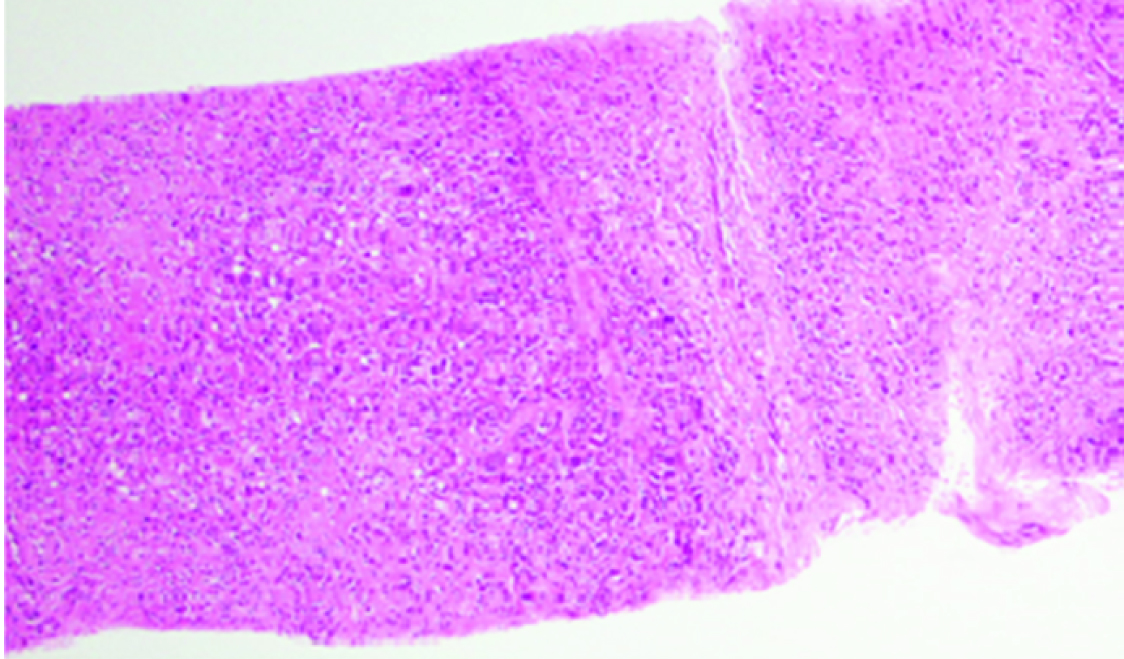
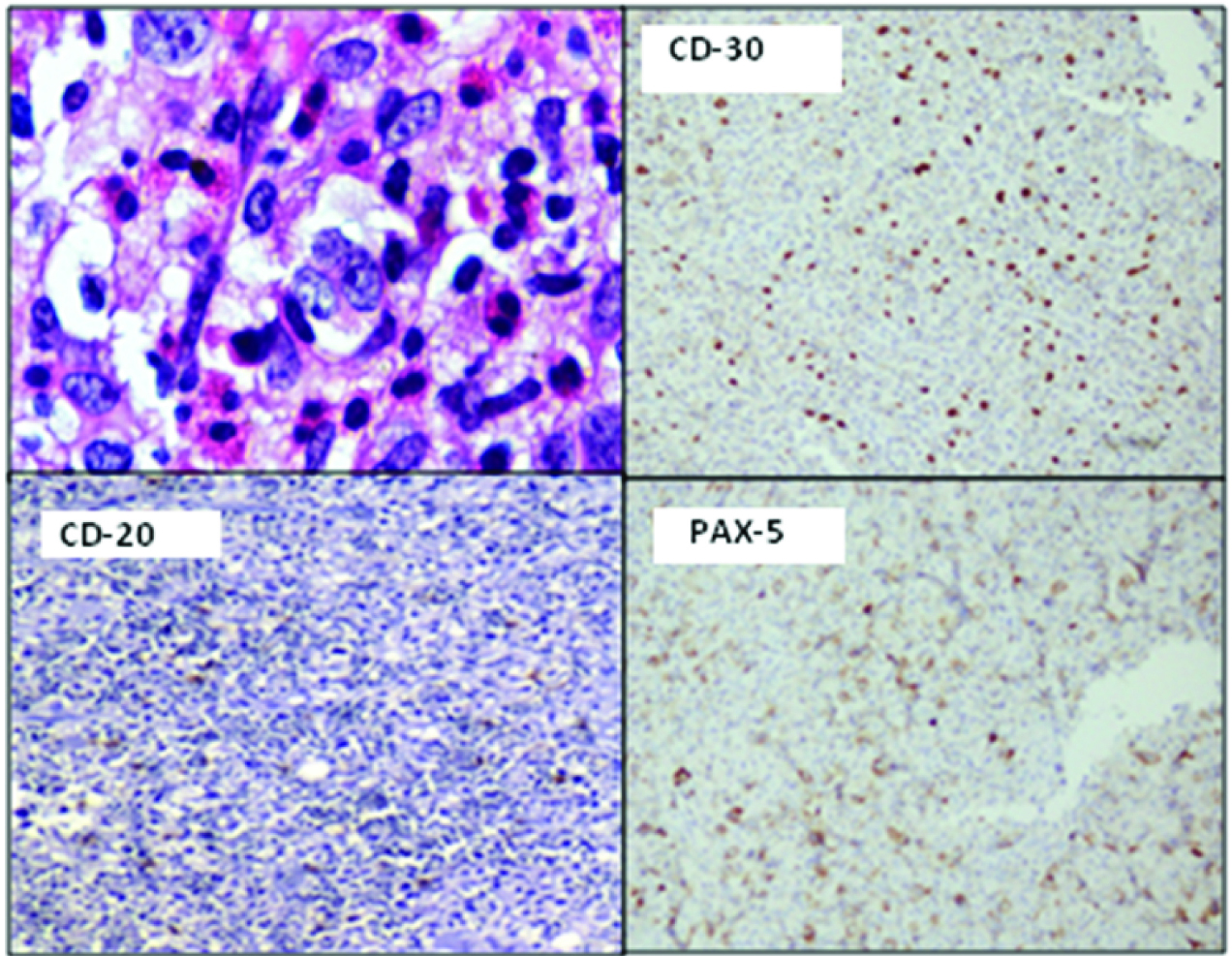
Trucut biopsy from the swelling revealed fibrous bands with lacunar variant of Reed Sternberg cells in a background of polymorphs, lymphocytes, eosinophils and plasma cells, a picture consistent with nodular Sclerosis Hodgkin’s lymphoma [Table/Fig-1]. On immunohistochemistry, the atypical Reed Sternberg cells were positive for CD-15, CD-30 and PAX-5 and negative for CD-45, ALK, BCL-2 and CD-20, a pattern typical of classical Hodgkin’s lymphoma [Table/Fig-2].
Low magnification view (X 100, Haematoxylin and eosin) of the sternal biopsy showing lymphoid aggregates (consisting of atypical Reed Sternberg cells and a reactive background) separated by fibrous bands.
High power magnification (x400, Haematoxylin and eosin) of the sternal biopsy showing characteristic Reed Sternberg cells (upper left). Immunohistochemistry of these atypical cells reveals positivity for CD-30 (upper right), PAX-5 (lower right) and negativity for CD-20 (lower left).
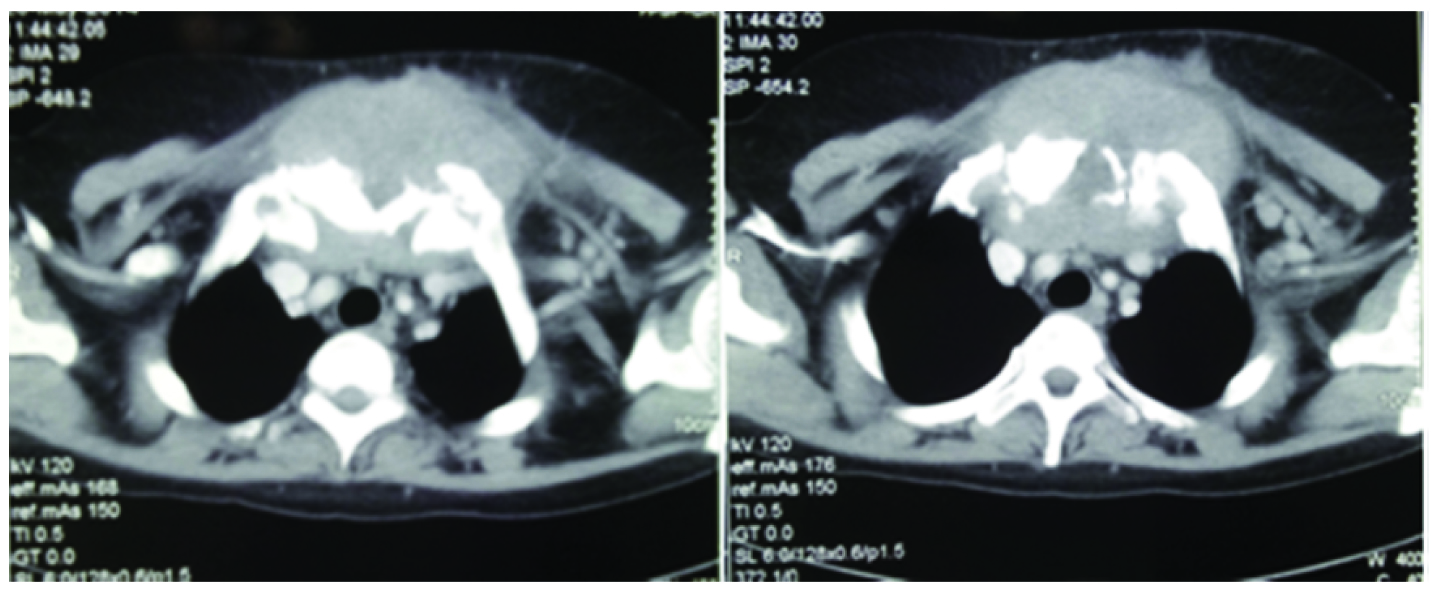
Contrast Enhanced CT scan (CECT) of chest, abdomen and pelvis revealed a large lobulated heterogeneously enhancing soft tissue mass measuring about 8x8cm in size involving the sternum, causing its destruction and extending into the anterior mediastinum with encasement of the left brachiocephalic vein [Table/Fig-3]. There was no mediastinal or abdominal lymphadenopathy and hepato-splenomegaly. Bone marrow examination was normal. Patient was diagnosed as a case of late relapse of nodular sclerosis Hodgkin’s lymphoma (Ann Arbor stage IBE). Australia antigen, Hepatitis C serology and HIV-1 and 2 were negative. Baseline 2D-echocardiogram revealed an ejection fraction (EF) of 60%. Pulmonary function test was normal.
Contrast enhanced CT (CECT) chest of the patient showing a lobulated heterogeneously enhancing soft tissue mass involving the sternum and extending into anterior mediastinum causing destruction of the sternum.
In view of late relapse and a localized disease, patient was planned for 4 cycles of ABVD followed by Involved Field Radiotherapy (IFRT) to the residual mass. After an informed and written consent, she was administered 4 cycles of ABVD regimen (Adriamycin-25mg/m2, Bleomycin-10U/m2, Vinblastine-6mg/m2 and Dacarbazine-375mg/m2 q2 weekly every 28 days) followed by IFRT (30 Gy over 18 fractions) to the local site .
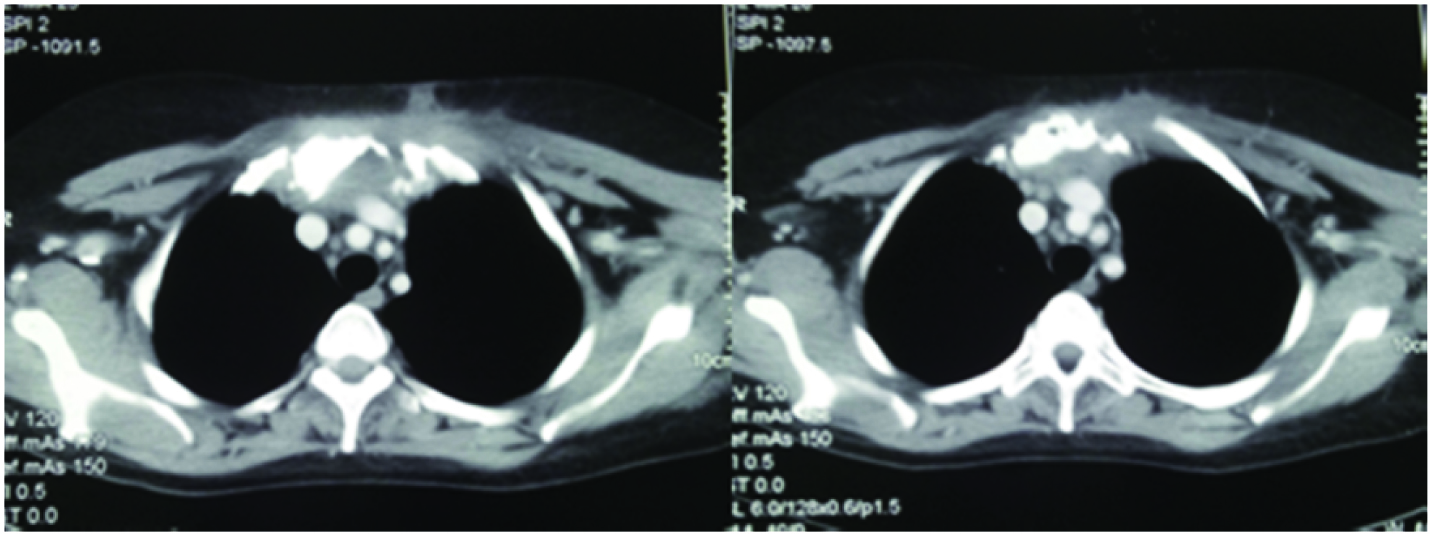
Patient’s swelling subsided after 4 cycles of chemotherapy. Repeat CECT chest done at the end of treatment revealed 95% reduction in the size of the mass lesion. However, a small residual mass was detected in the anterior mediastinum abutting the left brachiocephalic vein [Table/Fig-4]. FDG PET-CT further characterized the residual mass as sclerotic on the basis of its faint FDG avidity. Patient achieved complete remission after therapy and is in our regular follow-up since 1 year without any recurrence of sternal swelling or any clinically palpable lymphadenopathy.
CECT chest of the same patient showing a significant reduction in the size of the lesion after 4 cycles of ABVD regimen with a small residual fibrotic mass.
Discussion
Hodgkin’s lymphoma (HL) is a nodal B-cell neoplasm which characteristically presents as painless cervical lymphadenopathy. Extranodal presentation of HL is rare in an immunocompetent patient. Most commonly involved sites are gastrointestinal tract, pulmonary system, thyroid, skin, genitourinary tract and central nervous system [1]. Skeleton constitutes an unusual extranodal site in HL. Bone involvement is a feature of advanced HL and occurs in about 10-20% cases at some time during the course of disease (30-50% at the time of autopsy) [2]. Osseous HL at initial presentation is extremely rare (1-4%) [3]. Although thought to be only osseous at initial presentation, such cases are generally found to have non-osseous involvement as well during evaluation. Therefore, true ‘primary’ osseous HL is an exception [2]. Primary osseous HL therefore represents a distinct and extremely rare subset of cases whereby bone is the only site of involvement. Primary bone lymphoma is defined as being limited to bone with or without associated soft tissue component and no regional lymphadenopathy at diagnosis and for 6 months of follow-up. In a study of 442 cases of primary bone lymphomas, HL represented only 13 such cases [4]. It is important to remember that ‘bone marrow’ involvement which occurs in 5-10% of HL patients is not synonymous with ‘primary osseous HL’ [2]. Bone marrow involvement is classified as stage IV HL whereas ‘primary solitary osseous HL’ is stage IE according to Ann Arbor staging [1]. Bone involvement in HL may be due to primary growth into bone or secondary to haematogenous spread or involvement by an adjacent lymph node mass [5]. In case of osseous HL due to an adjacent lymph nodal invasion, suffix ‘E’ is added to the staging. However, if bone is involved due to advanced systemic disease, patient is classified as stage IV [6]. Osseous HL therefore, is of four subtypes: 1) Primary solitary HL; 2) primary multifocal HL; 3) osseous and non-osseous HL; and 4) osseous HL at recurrence [1]. Spine (thoracolumbar), pelvis, ribs, femur, sternum, clavicle and skull are the most commonly involved skeletal sites in HL (in descending order) [5]. Sternal involvement in HL is distinctly uncommon and has not been reviewed separately in the literature. Out of all the reported cases of osseous HL in the English literature, we selectively reviewed the data of ‘sternal HL’ [Table/Fig-5] [2,3,5–17].
Table showing clinical details of all the cases of sternal Hodgkin’s lymphoma reported in the English literature from 1966-2015.
| S. No | Author | year | age | sex | sternal involvement-primary/relapse | initial diagnosis | sternal involvement at initial diagnosis | treatment given for initial diagnosis | site of involvement along with sternal mass | stage | subtype | treatment given | Outcome |
|---|
| 1 | Arnold et al., [7] | 1966 | 21 | F | primary | Chondrosarcoma | Y | resection of the sternal mass | Sternum (15x15 cm) and mammary nodes | NA | NA | resection followed by post-operative RT | Alive at 24 months |
| 2 | Manoli et al., [8] | 1986 | 14 | M | primary | eosinophilic granuloma | Y | - | Sternum only | NA | NA | RT only due to incorrect diagnosis of eosinophilic granuloma | Died |
| 3 | 19 | F | primary | HL | Y | - | Sternum (3x4 cm) and bilateral supraclavicular lymphadenopathy | IIAE | NS | 4000 rads mantle field and peri-aortic RT with 1000 rads boost to the sternum | Alive at 3 years after presentation |
| 4 | Sullivan et al., [6] | 1987 | 22 | F | primary | HL | Y | - | Sternum (6 cm) with axillary LN | NA | NS | Mantle cell RT | Alive |
| 5 | Miano et al., [9] | 1990 | 9 | M | primary | HL | Y | - | Sternum (4 cm), inguinal LN | IIIAE | NS | 6XMOPP/ABVD followed by RT | Alive at 32 months |
| 6 | Borg et al., [10] | 1993 | 23 | M | NA | HL | NA | NA | Thoracic spine, pelvis, femur, sternum, skull | IIA | NS | Chemo + radiotherapy | Died |
| 7 | Ostrowski et al., [2] | 1998 | 50 | M | primary | HL | Y | | Sternum and bilateral axillary LN | NA | NA | RT | Died |
| 8 | 58 | M | primary | HL | Yy | | Anterior chest wall soft tissue | NA | NA | RT | Died |
| 9 | 20 | M | Relapse | HL | N | NA | Sternum and clavicle | NA | NA | RT | Died |
| 10 | Karimi et al., [11] | 2001 | 82 | F | primary | HL | Y | - | Two masses outside chest wall, one at middle of thoracic inlet, another at right side of sternum (5x5cm) | NA | NA | no treatment received due to poor PS | died 2 weeks after diagnosis |
| 11 | Petkov et al., [12] | 2006 | 33 | M | Relapse | HL | N | 6xCOPP/ABV followed by RT | Sternum only | IIB | NS | high dose CT followed by Auto-SCT | Not available |
| 12 | Priola et al., [3] | 2006 | 20 | M | primary | eosinophilic granuloma, IHC revealed HL | Y | - | Sternum, left supraclavicular LN | NA | NS | 6XABVD followed by RT | Alive at 32 months |
| 13 | Daizyreena et al., [13] | 2006 | 18 | M | primary | HL | Y | - | Sternum and supraclavicular LN | | | chemotherapy | Alive (on treatment) |
| 14 | Langley et al., [14] | 2008 | 7 | M | primary | TB | Y | ATT | Sternum (3 cm), L1 Vertebra, left sacroiliac joint, right acetabulum | IV | NA | chemotherapy (UKCCSG guidelines) | Alive |
| 15 | Biswas et al., [5] | 2008 | 21 | M | primary | TB | Y | 6 months ATT | Sternum (10x8 cm), left cervical LN, liver, spleen, abdominal LN | IVB | NS | 6XABVD followed by RT | Progressive disease managed by 3xICE regimenAlive at 3 months |
| 16 | Oshikawa et al., [15] | 2009 | 28 | M | primary | HL | y | | Sternum, right ilium, rib, left scapula | IV | MC | 6XABVD followed by RT to the ilium | Alive |
| 17 | Goyal et al., [16] | 2015 | 25 | F | primary | LCH | Y | RT with Vinblastine | Sternum (5x5 cm) with axillary, supraclavicular, pre-vascular, anterior diaphragmatic LN and splenic involvement | IIIBS | NS | initially received RT with vinblastine for LCH, later received 8x ABCD for stage IIIBS HL | Alive at 1.5 years |
| 18 | Singh et al., [17] | 2015 | 30 | F | primary | TB | Y | 5 months ATT | Sternum, cervical LN, pleural effusion, HSM, ascites, pre and para-aortic LN | NA | MC | 1XABVD | Died after 1 cycle of chemotherapy |
*M-male, F-female, HL-Hodgkin’s lymphoma, TB-tuberculosis, LCH-Langerhan cell histiocytosis, Y-yes, NS-Nodular sclerosis, MC-Mixed cellularity, RT-radiotherapy, LN-lymph node, NA-not available, ATT- anti-tubercular therapy, COPP- Cyclophosphamide/ vincristine/ procarbazine/ prednisolone, ABVD- adriamycin/bleomycin/vinblastine/dacarbazine, PS-performance status, ICE- Ifosphamide/carboplatin/etoposide, CT-chemotherapy, SCT-stem cell transplantation.
After an extensive search at PUBMED using the MESH terms ‘Hodgkin’s, sternum and osseous’, we could identify 18 cases of HL with sternal involvement (both primary and secondary, both initial presentation and at relapse) in the English literature from 1966-2015. Along with sternal involvement, 10 patients had an additional lymph node involvement, 5 had involvement of other skeletal sites and only 3 patients had isolated or ‘primary’ sternal involvement. Male were more commonly affected than females (M: F-2:1) and median age was 27.7 years (7-82 years). Three cases of paediatric sternal hodgkin’s lymphoma (case no.2, 5 and 14) were also identified. Histology was available in 10 cases for review. Amongst the available histological subtypes, nodular sclerosis was the most common subtype (80%) followed by mixed cellularity (20%). Seven cases (38.8%) were initially misdiagnosed (most commonly as tuberculosis and eosinophilic granuloma) based on histopathological examination. Eighty eight (88%) percent of the cases had sternum involvement at initial presentation and an additional 12% had it at relapse. Treatment included Radiotherapy (RT) alone in 7 (38.8%), combined chemo-radiotherapy in 6 (33.3%), chemotherapy alone in 3 (16.6%), Auto SCT in 1 (5.5%) patient. One patient couldn’t receive treatment due to poor performance status. Outcomes of 17 cases indicates that 10 (59%) were alive and 7 (41%) died of the disease.
Only 3 patients out of 18 (17%) had a ‘primary sternal’ hodgkin’s lymphoma. All 3 were males (mean age-35 years). Two of them had sternal involvement at initial presentation (treated by only RT and died) and one had it at relapse (treated by high dose chemotherapy followed by Auto SCT). Therefore, we summarize that isolated sternal involvement in HL is extremely rare and usually involves males in their third decade. Radiotherapy alone might not be an optimal therapy in these cases as evidenced by a high mortality rate (100%) in cases receiving it. Our case is the first reported case where sternum was the only site of Hodgkin’s disease both at initial presentation as well as at relapse. Disease recurred in our case probably because she didn’t receive RT after chemotherapy during initial treatment. Since late relapse remains chemosensitive to the initial therapy, combined chemo-radiotherapy brought complete remission in the patient.
Conclusion
Present case along with literature review highlights the fact that Hodgkin’s lymphoma should be kept in the differential diagnosis of a sternal mass and a high index of suspicion must be maintained in such cases due to approximately a 40% chance of misdiagnosis on histopathological examination. Use of immunohistochemistry as a tool for definitive diagnosis is strengthened here. Combined chemo-radiotherapy for treatment of ‘isolated sternal HL’ is strongly advocated.
*M-male, F-female, HL-Hodgkin’s lymphoma, TB-tuberculosis, LCH-Langerhan cell histiocytosis, Y-yes, NS-Nodular sclerosis, MC-Mixed cellularity, RT-radiotherapy, LN-lymph node, NA-not available, ATT- anti-tubercular therapy, COPP- Cyclophosphamide/ vincristine/ procarbazine/ prednisolone, ABVD- adriamycin/bleomycin/vinblastine/dacarbazine, PS-performance status, ICE- Ifosphamide/carboplatin/etoposide, CT-chemotherapy, SCT-stem cell transplantation.
[1]. Li Y, Wang XB, Tian XY, Li B, Li Z, Unusual primary osseous Hodgkin Lymphoma in rib with associated soft tissue mass: a case report and literature reviewDiagn pathol 2012 7:64 [Google Scholar]
[2]. Ostrowski ML, Inwards CY, Strickler JG, Witzig TE, Wenger DE, Unni KK, Osseous Hodgkin’s diseaseCancer 1999 85:1166-78. [Google Scholar]
[3]. Priola SM, Priola AM, Cataldi A, Fava C, Nodular sclerosing Hodgkin disease presenting as a sternal massBr J Haematol 2006 135:594 [Google Scholar]
[4]. Ostrowski ML, Unni KK, Banks PM, Shives TC, Evans RG, O’Connell MJ, Malignant lymphoma of boneCancer 1986 58:2646-55. [Google Scholar]
[5]. Biswas A, Puri T, Goyal S, Haresh KP, Gupta R, Julka PK, Osseous Hodgkin’s lymphoma—review of literature and report of an unusual case presenting as a large ulcerofungating sternal massBone 2008 43:636-40. [Google Scholar]
[6]. Sullivan WT, Solonick DM, Case report 414: Nodular sclerosing Hodgkin disease involving sternum and chest wallSkeletal Radiol 1987 16:166-69. [Google Scholar]
[7]. Arnold HS, Meese EH, D’Amato NA, Maughon JS, Localised Hodgkin’s disease presenting as a sternal tumor and treated by total sternectomyAnn Thorac Surg 1966 2:87-93. [Google Scholar]
[8]. Manoli A 2nd, Blaustein JC, Pedersen HE, Sternal Hodgkin’s disease: report of two casesClin Orthop Relat Res 1988 228:20-25. [Google Scholar]
[9]. Miano C, Lombardi A, Russo LA, Ceci A, Baronci C, Bonaldi U, Hodgkin’s lymphoma with nodular sclerosis. A report of a case with an unusual sternal location at the onsetPaediatr Med Chir 1991 13:639-40. [Google Scholar]
[10]. Borg MF, Chowdhury AD, Bhoopal S, Benjamin CS, Bone involvement in Hodgkin’s diseaseAustralas Radiol 1993 37:63-66. [Google Scholar]
[11]. Karimi S, Mohammadi F, Pejhan S, Zahirifard S, Azari PA, An unusual presentation of Hodgkin’s lymphoma as a chest wall abscess in association with old tuberculosisTanaffos 2007 6:71-74. [Google Scholar]
[12]. Petkov R, Nossikoff AV, Alexandrova K, Stanchev A, Ousheva R, Hadgiev E, A case of sternal involvement in an early relapse of hodgkin disease verified with ultrasound guided core needle biopsyEur J Radiol Extra 2006 60(2):75-78. [Google Scholar]
[13]. Daizyreena WJW, Mar@Salmah JW, Abdul K, Hodgkin lymphoma of sternum: a rare occurrenceMalaysian J Med Sci 2006 (Supp 13):120 [Google Scholar]
[14]. Langley CR, Garrett SJ, Urand J, Kohler J, Clarke NM, Primary multifocal osseous Hodgkin’s lymphomaWorld J Surg Oncol 2008 6:34 [Google Scholar]
[15]. Oshikawa G, Arai A, Sasaki K, Ichinohasama R, Miura O, Primary multifocal osseous Hodgkin lymphomaRinsho Ketsueki 2009 50:92-96. [Google Scholar]
[16]. Goyal S, Biswas A, Puri T, Gupta R, Julka PK, Osseous Hodgkin’s lymphoma with sternal involvement at presentation: Diagnostic challengesClin Cancer Investig J 2015 4:447-50. [Google Scholar]
[17]. Singh S, Jenaw RK, Jindal A, Bhandari C, Hodgkin’s lymphoma presenting as lytic sternal swellingLung India 2015 32:410-12. [Google Scholar]