Unusual Variation in the Branching Pattern of the Celiac Trunk and Its Embryological and Clinical Perspective
Shilpi Agarwal1, Babita Pangtey2, Neelam Vasudeva3
1 Senior Resident, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
2 Assistant Professor, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
3 Director Professor and Head of Department, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shilpi Agarwal, C2 /186, First Floor, Janakpuri, New Delhi-110058, India.
E-mail: drshilpiagg@gmail.com
Knowledge of variations in the branching pattern of Celiac Trunk (CT) is important for surgeries of stomach, duodenum, pancreas and hepatobiliary region, for abdominal aortic aneurysm, for liver transplant and chaemoembolization of hepatic tumours. An unusual variation in the branching pattern of CT was observed in 50-year-old male cadaver of Indian origin. CT divided into six branches out of which right & left inferior phrenic arteries originated as first two branches and left gastric artery as the third branch. CT ended into three terminal branches as common hepatic artery, splenic artery & dorsal pancreatic artery. Right gastric artery originated from left hepatic artery instead of common hepatic artery. A variant hepatic artery to the left lobe of liver was also observed which originated from right gastric artery. Anatomical variations in the branching pattern of CT are due to developmental changes in ventral splanchnic artery.
Dorsal pancreatic artery, Inferior phrenic artery, Splanchnic artery
Case Report
An unusual variation in Celiac Trunk (CT) branching pattern was observed in formalin fixed 50-year-old male cadaver of Indian origin during the routine dissection classes of the abdominal region at Maulana Azad Medical College, New Delhi. In the present case, six branches originated from CT in contrast to its normal trifurcation. All the branches of CT were carefully dissected to trace their origin and course and then photographed.
The CT was observed to arise as first branch from the ventral surface of the abdominal aorta at the level of intervertebral disc between T12 and L1 vertebra. It was 2.3cm long and had an external diameter of 1.8cm and traversed horizontally forwards. On further dissection while tracing the course of CT, we observed an unusual branching pattern of CT as compared to its usual trifurcation. We observed that CT divided into six branches as Right & Left Inferior Phrenic Arteries (RIPA & LIPA), Left Gastric Artery (LGA), Splenic Artery (SA), Common Hepatic Artery (CHA) & Dorsal Pancreatic Artery (DPA) [Table/Fig-1].
Variant branching pattern of the celiac trunk in the present case report. Ct-Celiac trunck, LGA-Left Gastric Artery, SA-Splenic Artery, CHA-Common hepatic artery, RIPA-Right inferior phrenic artery, LIPA-Left inferior phrenic artery, DPA-dorsal pancreatic artery, SMA-Superior mesenteric artery, IPDA-Inferior pancreaticoduodenal artery.
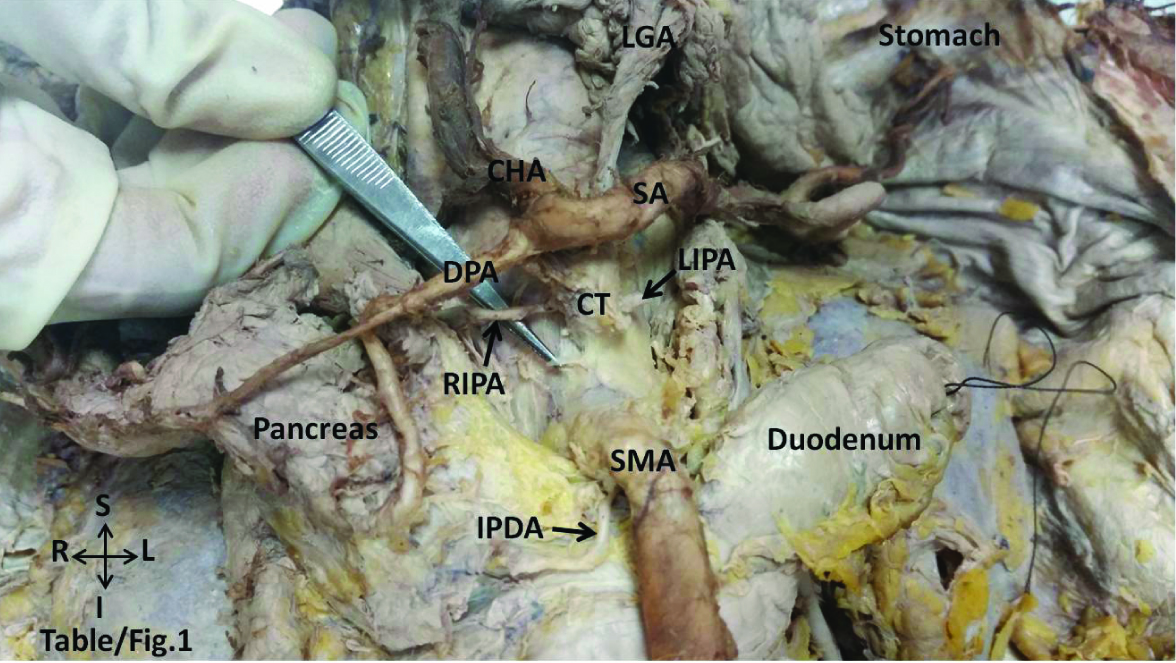
RIPA & LIPA originated as the first two branches of CT from its respective lateral aspect. Both arose at 0.5cm from the origin of CT and had external diameter of 0.2cm. They were not found to originate directly from the abdominal aorta or any other artery. Both the arteries ascended upwards and laterally, anterior to the crura of the diaphragm and terminated on the abdominal surface of the respective domes of the diaphragm.
A third branch was observed to arise 2cm distal to the origin of CT as LGA with diameter of 0.45 cm. It ascended forwards and to the left of midline into the superior part of the lesser omentum. It then turned anteroinferiorly along the lesser curvature and anastomosed with Right Gastric Artery (RGA) in the region of incisura angularis. It followed the normal course and had normal branching pattern.
Finally, the CT ended into three terminal branches as CHA, SA & DPA having external diameters of 0.9cm, 1.8cm & 0.7cm respectively.
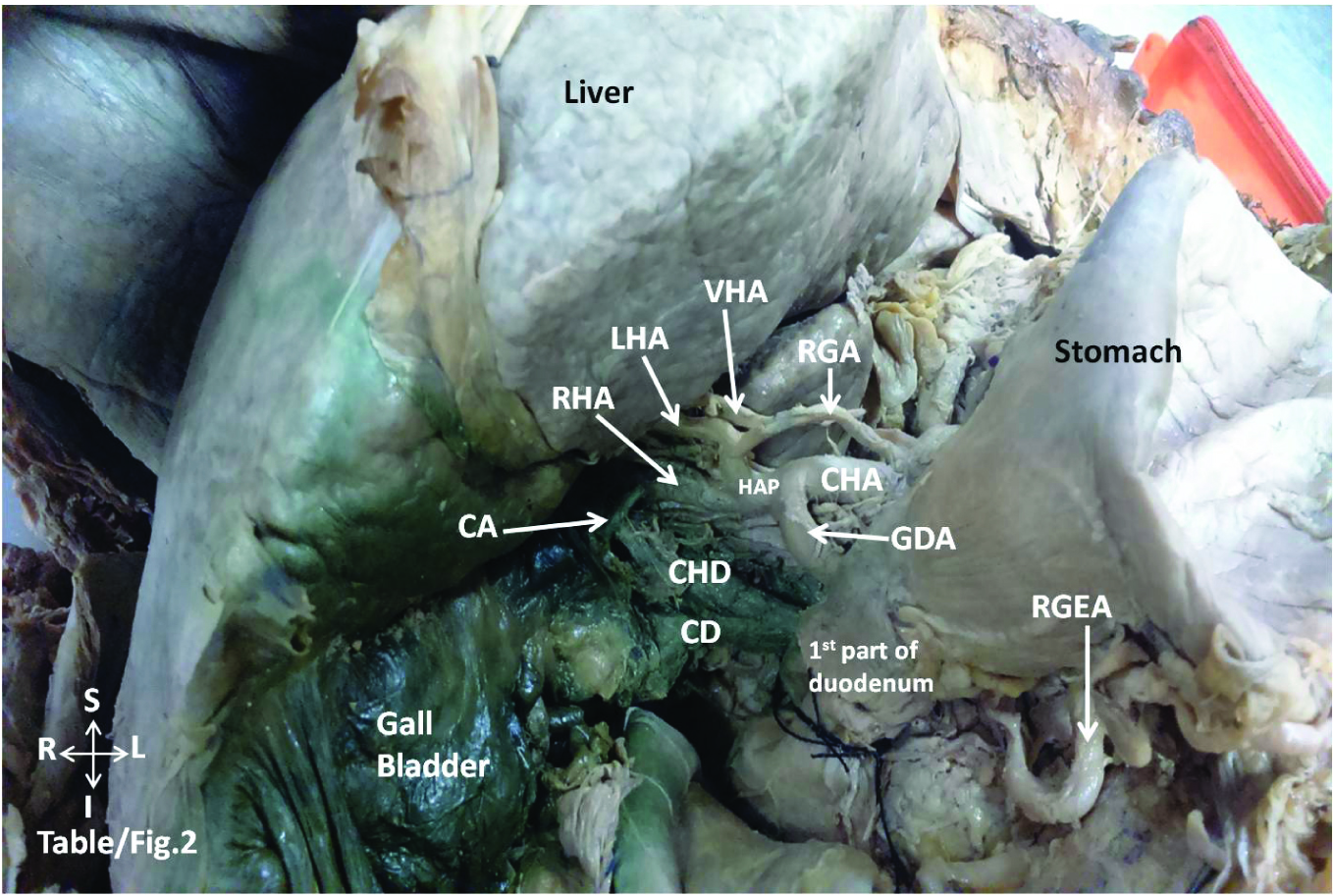
CHA, fourth branch of CT, coursed anteriorly and to the right along the upper surface of the first part of duodenum. Here it divided into gastroduodenal artery and hepatic artery proper (HAP). HAP traversed anterior to the portal vein and medial to the bile duct within the layers of lesser omentum along its free border. It terminated into right and left hepatic arteries (RHA & LHA). Right Gastric Artery (RGA) originated from LHA instead of arising from CHA and then ascended along the lesser curvature of stomach to anastomose with LGA. On further dissection, another variation was observed in the form of a variant hepatic artery to the left lobe of liver which originated from RGA. It ran parallel to LHA and further coursed into porta hepatis and was observed to enter into the left lobe of the liver. The origin and course of cystic artery was normal [Table/Fig-2].
Variant origin of Right Gastric Artery (RGA) & A Variant Heptic Artery to the left lobe of liver (VHA) in the present case report. CHA-Common Hepatic artery, GDA-Gastro-Duodenal Artery, HAP-Hepatic artery proper, LHA-Left hepatic artery, RHA-Right hepatic artery, CA-Cystic artery, RGEA-Right Gastroepiploic artery, CHD-Common hepatic duct, CD-Cystic duct.
The fifth branch from CT i.e., splenic artery coursed horizontally to the left along the superior border of body of the pancreas. Its course and branching pattern was normal.
The last i.e., sixth branch from the CT was dorsal pancreatic artery which was observed to course downwards behind the body of pancreas. Here it divided into two branches which supplied the inferior border and lower part of head of pancreas. Apart from this accessory branch, pancreas received superior and inferior pancreaticoduodenal arteries, which originated from gastroduodenal artery and superior mesenteric artery respectively, as usual and had a normal course.
Discussion
Knowledge of variations in the branching pattern of CT is important for surgeries of stomach, duodenum, pancreas and hepatobiliary region, for abdominal aortic aneurysm, penetrating injuries of abdomen, in patients undergoing celiac arteriography for gastrointestinal bleeding, for liver transplant and chaemoembolization of hepatic and pancreatic tumours [1]. Risk of vascular injury is more common during laparoscopic procedures as the operative field is limited and there are increased chances of ligation or division of the wrong vessel, which may lead to bleeding, necrosis, gas embolism and hypovolaemic shock [2]. Thus, surgeons, oncologists and radiologists should be aware of such variations to avoid iatrogenic injuries and to prevent complications after various procedures.
The present variant branching pattern has been compared with previously reported variations in [Table/Fig-3] [1,3–9]. The combination of vascular variations found in the present case has been rarely reported earlier.
Comparison of the previously reported variations in the branching pattern of celiac trunk with the present case report. LGA-Left Gastric artery. SA-Splenic Artery, CHA-Common hepatic artery. RIPA-Right inferior phrenic artery, LIPA-Left inferior phrenic artery, GDA-Gastro-Duodenal artery, DPA-Dorsal pancreatic artery, AHA-Accessory hepatic artery.
| S. No. | Author name and year | Year | Branching pattern of the coeliac trunk |
|---|
| 1 | Cicekcibasi et al., [3] | 2005 | LGA + SA + CHA + LIPA + RIPA + Left gastroepipolic artery |
| 2 | Nayak et al., [4] | 2008 | LGA + SA + LIPA + GDA |
| 3 | Mahajan et al., [5] | 2009 | LGA + SA + CHA + AHA + Retroportal Artery |
| 4 | Astik & Dave [1] | 2011 | LGA + SA + CHA + RIPA + GDA + Left Superior Suprarenal Artery + Left Middle Suprarenal Artery |
| 5 | Kalthur et al., [6] | 2011 | LGA + SA + CHA + DPA |
| 6 | D’Souza et al., [7] | 2012 | LGA + SA + CHA + AHA + APA |
| 7 | Nayak et al., [8] | 2012 | LGA + SA + CHA + LIPA |
| 8 | Sathidevi & Rahul [9] | 2013 | LGA + SA + CHA + GDA |
| 9 | Present Case Report | 2016 | LGA + SA + CHA + LIPA + RIPA + DPA |
In the present case, both IPA arose directly from CT which was similarly observed in 7.86% by Petrella, in 3.125% by Pulakunta, in 4% by Tiwari and Jeyanthi in cadaveric studies and in 0.8% by Rawat in angiographic study [10–13]. Knowledge of variant origin of IPA is of importance to surgeons to prevent sectioning of these small calibre arteries during treatment of compression syndrome of CT. In addition, oncologist and interventional radiologists should also be aware of such variations as IPA can be used to treat unresectable hepatocellular carcinoma by transcatheter oily chaemoembolization therapy [10].
DPA arose as one of the branches of CT in the current case which was also reported by Kalthur et al., and Sawant et al., [6,14]. Kadir has reported that DPA can arise from superior mesenteric (40%), celiac trunk (22%), CHA (20%) or aorta (14%) [15]. Knowledge of such variant branches is significant during pancreatic surgeries to prevent inadvertent ligation or injury.
RGA originated from LHA in the present case which has also been reported by Sawant et al., and Nayak et al., previously [14,16]. In such variants, catheter may be passed though RGA for embolization of LHA, when required [16].
Variant arterial anatomy near the hepatobiliary region is of great importance during laparoscopic or open cholecystectomy and liver transplants. The present case reported the presence of a variant hepatic artery to the left lobe of liver which originated from RGA. Sawant et al., had reported an aberrant hepatic artery entering the right lobe of liver which arose from superior mesenteric artery [14].
During fetal development, each dorsal aorta gives origin to paired ventral splanchnic arteries which supply the primitive gut and its derivatives. Soon, the dorsal aorta fuse leading to fusion of ventral splanchnic arteries which then form a series of unpaired segmental vessels in the dorsal mesentery of the primitive gut. These vessels further divide into ascending and descending branches which anastomose to form dorsal and ventral splanchnic longitudinal anastomotic channels along the dorsal and ventral aspects of the primitive gut. Subsequently, ventral splanchnic arteries reduce in number by disappearance of most of the stems of origin and by the fusion of some of those which persist to form single midline vessels in the dorsal mesentery. These midline vessels are represented in later stages by three arterial trunks, the celiac trunk, superior mesenteric artery and inferior mesenteric artery, which are distributed to foregut, midgut and hindgut respectively. Celiac trunk initially originates from the dorsal aorta at the seventh cervical level which subsequently migrates caudally to the twelfth thoracic level by differential growth and due to descent of viscera supplied in the abdomen [17]. Vascular variations may occur due to persistence of some parts of the longitudinal channels between primitive vessels that normally disappear or due to disappearance of parts that normally persist. Others factors which may contribute to such vascular variations include the rotation of the midgut, physiological herniation, leftward migration of the spleen and haemodynamic changes in the abdominal viscera [18].
Conclusion
Accurate and thorough knowledge of the vascular variations will be useful in surgical, oncological and interventional procedures and shall be kept in mind to prevent any inadvertent complications. Presence of accessory arteries may provide collateral circulation which may prove important during transplant surgeries. Variant vascular branching pattern may be attributable to errors in complex developmental stages of vascular pattern.
[1]. Astik RB, Dave UH, Uncommon branching pattern of the celiac trunk: origin of seven branchesInternational Journal of Anatomical Variations 2011 4:83-85. [Google Scholar]
[2]. Prakash Rajini T, Mokhasi V, Geethanjali BS, Sivacharan PV, Shashirekha M, Coeliac trunk and its branches: anatomical variations and clinical implicationsSingapore Medical Journal 2012 53(5):329-31. [Google Scholar]
[3]. Cicekcibasi AE, Uysal I, Seker M, Tuncer I, Buyukmcu M, Salbacak A, A rare variation of the coeliac trunkAnnals of Anatomy 2005 187:387-91. [Google Scholar]
[4]. Nayak SR, Prabhu LA, Krishnamurthy A, Kumar CG, Ramanathan LA, Acharya A, Additional branches of celiac trunk and its clinical significanceRomanian Journal of Morphology and Embryology 2008 49(2):247-49. [Google Scholar]
[5]. Mahajan A, Paul S, Das S, An anatomical variation in the branching pattern of the coeliac trunkArch Med Sci 2009 5(1):117-19. [Google Scholar]
[6]. Kalthur SG, Sarda R, Bankar M, Multiple vascular variations of abdominal vessels in a male cadaver: embryological perspective and clinical importanceJ Morphol Sci 2011 28(3):152-56. [Google Scholar]
[7]. D’Souza AS, Vijayalakshmi Hemalatha Pugazhandhi Mamatha H, Anatomical variations in the branches of the Coeliac trunkJournal of Cinical and Diagnostic Research 2012 6(3):333-35. [Google Scholar]
[8]. Nayak SB, Ashwini LS, Swamy Ravindra S, Abhinitha P, Marpalli S, Pant J, Surgically important accessory hepatic artery – a case reportJ Morphol Sci 2012 29(3):187-88. [Google Scholar]
[9]. Sathidevi VK, Rahul UR, Coeliac trunk variations- case reportInternational Journal of Scientific and Research Publications 2013 3(2):1-4. [Google Scholar]
[10]. Petrella S, Rodrigues CFS, Sgrott EA, Fernandez GJM, Marques SR, Prates JC, Origin of inferior phrenic arteries in the celiac trunkInt J Morphology 2006 24(2):275-78. [Google Scholar]
[11]. Pulakunta T, Potu BK, Gorantla VR, Rao MS, Madhyastha S, Vollala VR, The origin of inferior phrenic artery: a study in 32 South Indian cadavers with a review of literatureJ Vasc Bras 2007 6(3):225-30. [Google Scholar]
[12]. Tiwari S, Jeyanthi K, Study of origin of inferior phrenic arteries from the celiac trunkAnatomica Karnataka 2012 6(3):38-41. [Google Scholar]
[13]. Rawat KS, CTA in evaluation of vascular anatomy and prevalence of vascular variants in upper abdomen in cancer patientsInd J Radiol Imag 2006 16(4):457-61. [Google Scholar]
[14]. Sawant SU, Kolekar SM, Harichandana N, Anatomical variations in the celiac trunk and its branchesInternational Journal of Recent Trends in Science and Technology 2013 6(3):130-33. [Google Scholar]
[15]. Kadir S, Celiac, superior mesentric and inferior mesentric arteries - In Atlas of normal and variant angiographic anatomy 1991 WB Saunders:297-364. [Google Scholar]
[16]. Nayak BS, Sudarshan S, Madhav NV, Rao S, Unusual branching pattern of common hepatic artery: a case reportInternational Journal of Anatomical Variations 2012 5:126-27. [Google Scholar]
[17]. Standring S, Gray’s Anatomy: Anatomical Basis of Clinical Practice 2016 41st editionNew YorkElsevier Churchill Livingstone:202 [Google Scholar]
[18]. Reuter SR, Redman HC, Gastrointestinal angiography 1977 2nd EdPhiladelphiaWB Saunders:31-65. [Google Scholar]