Brachial plexus block is an excellent method for attaining optimal operating conditions for upper limb surgeries by producing complete muscular relaxation, maintaining haemodynamic stability and the associated sympathetic block. They also provide extended postoperative analgesia with minimal side effects. In addition, it offers a better preservation of mental functions in elderly; decreased risk of aspiration due to intact pharyngeal and laryngeal reflexes; avoids difficult intubation; decreases postoperative complications associated with intubation and provides better postoperative analgesia without undue sedation facilitating early mobilization and discharge [1].
Many adjuvants have been used including opioids such as morphine, fentanyl, tramadol, buprenorphine, sufentanil and calcium channel blockers such as verapamil and alfa-agonists such as clonidine [2].
Use of steroids as adjuvant to local anaesthetic drug in brachial plexus block is gaining popularity. Recently, dexamethasone has been studied as an adjuvant to local anaesthetic in peripheral nerve block [3]. Steroids have nerve block prolonging effects by blocking transmission of nociceptive myelinated c-fibres and suppressing ectopic neuronal discharge. They are also thought to alter the function of potassium channels in the excitable cells. Thus, dexamethasone was selected as an adjuvant to local anaesthetic (levobupivacaine) in this study because it has been reported to prolong duration of action of local anaesthetics with no respiratory depression [4].
Amongst various approaches to brachial plexus block, supraclavicular approach is the most commonly performed and most reliable method for surgeries below the shoulder joint. Potential complications include pneumothorax (1-6%), haemothorax, horner’s syndrome and phrenic nerve block [4].
To observe the effect of dexamethasone on onset and duration of anaesthesia, when used as an adjuvant to levobupivacaine in supraclavicular brachial plexus block.
Materials and Methods
In this prospective randomized, controlled, double blinded study which was conducted from August 2013 to October 2015. It included 60 patients, aged 18 to 65 years of ASA grade I and II of either sex who were scheduled to undergo elbow, forearm and hand surgery under supraclavicular brachial plexus block. The subjects were randomly allocated in two equal groups of 30 each. In Group-1 patients received 30 ml of levobupivacaine 0.5% with 2ml of normal saline while in Group-2 patients received injection dexamethasone 2ml (8mg) in addition to 30ml of levobupivacaine 0.5%.
Exclusion criteria were patient refusal, uncontrolled diabetes mellitus, renal or liver disease, circulatory instability, pregnant women, allergy to local anaesthetic, coagulation disorder, neurological disorder deficit or associated nerve lesion, skin lesion at the site of blockade or associated lesions in other areas of body requiring general anaesthesia, severe respiratory disease.
A written informed consent was obtained from each patient after explaining the technique prior to inclusion in this study in their own vernacular language.
Heart Rate (HR), Systolic and Diastolic Blood Pressures and Oxygen Saturation (Spo2) were recorded just before the block and at regular intervals thereafter. An intravenous drip was started before undertaking the procedure which continued throughout the duration of surgery and oxygen at the rate of 2L/min administered through oxygen mask.
The brachial plexus block was carried out with the patient lying in the supine position without a pillow, arms at his/her sides and head turned to side opposite to the one being blocked. The upper limb to be anaesthetized was abducted and extended along the side towards the ipsilateral knee as far as possible. About 2cm above the mid-clavicular point, just lateral to subclavian artery pulsation, a 24 gauge 1.5 inch needle was introduced and directed caudally and medially to reach the first rib. Paraesthesias were elicited by “walking over” the first rib, when 30ml of local anaesthetics solution was injected in this area.
Sensory and motor blocks of the median, radial, ulnar and musculocutaneous nerves were recorded at 5, 10, 15, 20, 25, 30, 45, 60, 75, 90 and 120 minutes after the block and 30 minutes and 3, 6, and 12 hours after the end of the surgery.
After injection, patients were pinpricked to assess for sensory blockade. The palmar surfaces of the index and little finger were used to test the median and ulnar nerve in the hand, respectively. To test the radial nerve the dorsal surface of the thumb was used. Sensory characteristics of the block were assessed using response to pinprick to 23-G hypodermic needle.
0 normal sensations to pin prick.
1 dull response to pin prick.
2 no response to pin prick.
Motor block was tested by thumb adduction (ulnar nerve), thumb abduction (radial nerve), flexion of the elbow and pronation of forearm (musculo-cutaneous nerve), and thumb opposition (median nerve).
A modified Lovett rating scale was used for assessing motor block, ranging from 6 (usual muscular force) to 0 (complete paralysis). Thumb abduction was evaluated for the radial nerve, thumb adduction for the ulnar nerve, thumb opposition for the median nerve and flexion of elbow for the musculo-cutaneous nerve [5].
6 = Normal muscular force
5 = Slightly reduced muscular force
4 = Pronounced reduction of muscular force
3 = Slightly impaired mobility
2 = Pronounced mobility impairment
1 = Almost complete paralysis
0 = Complete paralysis.
The time of onset of sensory block was defined as the interval between the completion of injection and loss of pain in pinprick test on palmar surfaces of the index and little finger dorsal surface of the thumb and at around the injury site of forearm.
The onset time of motor block was defined as the time between the completion of the local anaesthetic injection and complete paralysis.
The duration of the sensory block was defined as the time interval between complete sensory block and the return of normal sensation.
The duration of motor block was defined as the time interval between the complete paralysis and complete recovery of motor function.
The time to first analgesic use and total need for analgesics were recorded during the first postoperative 12 hours.
Pain was evaluated using the visual analog scale (VAS) where zero (0) represented no pain and 10 meant the worst possible pain [5].
If VAS values were > 4, it was considered that analgesic action of the drugs is terminated and rescue analgesic (IM Diclofenac 1-1.5mg/kg) given.
Possible Side Effects of Brachial Plexus Block
The following possible side-effects were anticipated and their incidence was noted:
Drowsiness
Pruritus
Nausea/vomiting
Horner’s syndrome
Phrenic nerve palsy
Pneumothorax
Respiratory depression
Signs and symptoms of local anaesthetic toxicity.
The above assessments were carried out by the principal investigator who was blinded to the drugs administered in the plexus block. Neither the patient nor the principal investigator knew about the drug preparation and treatment group of the patient.
In the circumstance of inadequate or patchy action of the block, the block was supplemented with general anaesthesia.
Statistical Analysis
Sample size calculation was performed before patient recruitment based on a previous study [7,8].
All results were expressed in Mean±Standard Deviation (SD) or percentage as applicable. Statistical analysis was carried out using Statistical Package for Social Science for Windows Version 13.0. Results were considered statistically significant where p-value were less than 0.05.
Results
Demographic characteristics and duration of surgery were comparable in both the study groups [Table/Fig-1].
| Group-1(n=30)(M ±SD) | Group-2 (n=30)(M ±SD) |
|---|
| Age (years) | 39.20±12.508 | 38.60±13.206 |
| Sex (Male/Female) | 21/9 | 20/10 |
| Weight (kg) | 66.20±6.172 | 67.20±5.054 |
| Duration of surgery (min) | 65.167±7.129 | 66.23±8.717 |
The mean time of onset of sensory blockade was 10.20 minutes (mean) in Group 1 and 8.1667 minutes (mean) in Group 2 while the onset time of motor blockade was 15.033 minutes (mean) in Group 1 and 13.76 minutes in Group 2 [Table/Fig-2].
| Group-1(n=30)(M ±SD) | Group-2(n=30)(M ±SD) | p-value |
|---|
| Onset of sensory blockade (min) | 10.20±1.349 | 8.1667±0.985 | <0.001(SS)* |
| Onset of motor blockade (min) | 15.033±0.889 | 13.7667±2.045 | 0.003(SS)* |
| Duration of sensory blockade (min) | 657.5±8.382 | 923±12.905 | 0.0001(SS)* |
| Duration of motor blockade (min) | 540±7.428 | 798.83±15.010 | <0.001(SS)* |
| Total analgesic requirement | 24 | 0 | 0.03 (SS)* |
*SS- Statistically Significant
The mean duration of sensory blockade was 657.2 minutes (mean) in Group 1 and 923 minutes (mean) in Group 2 while the duration of motor blockade was 540 minutes (mean) in Group 1 and 798.83 minutes (mean) in Group 2. The 12-hour postoperative VAS was also lower in Group 2 [Table/Fig-2].
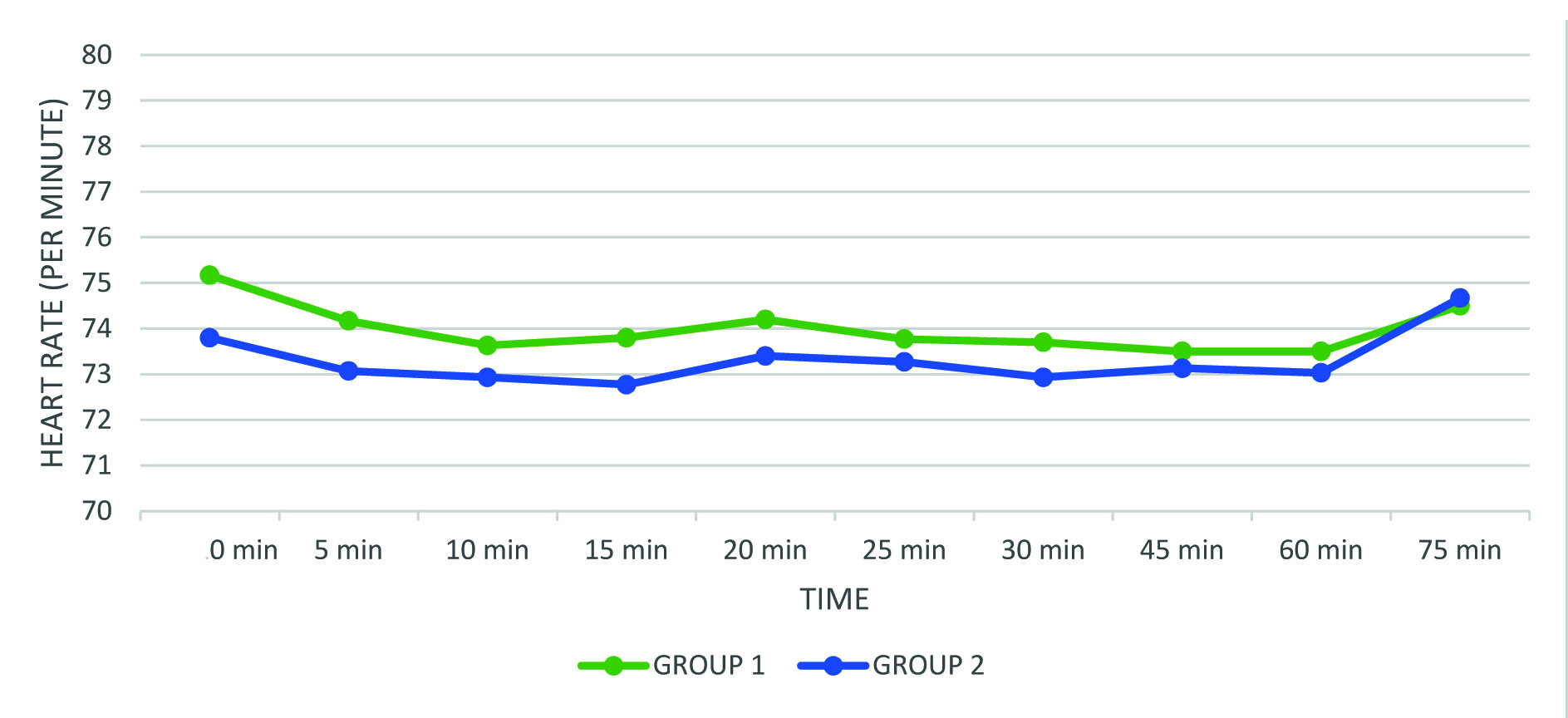
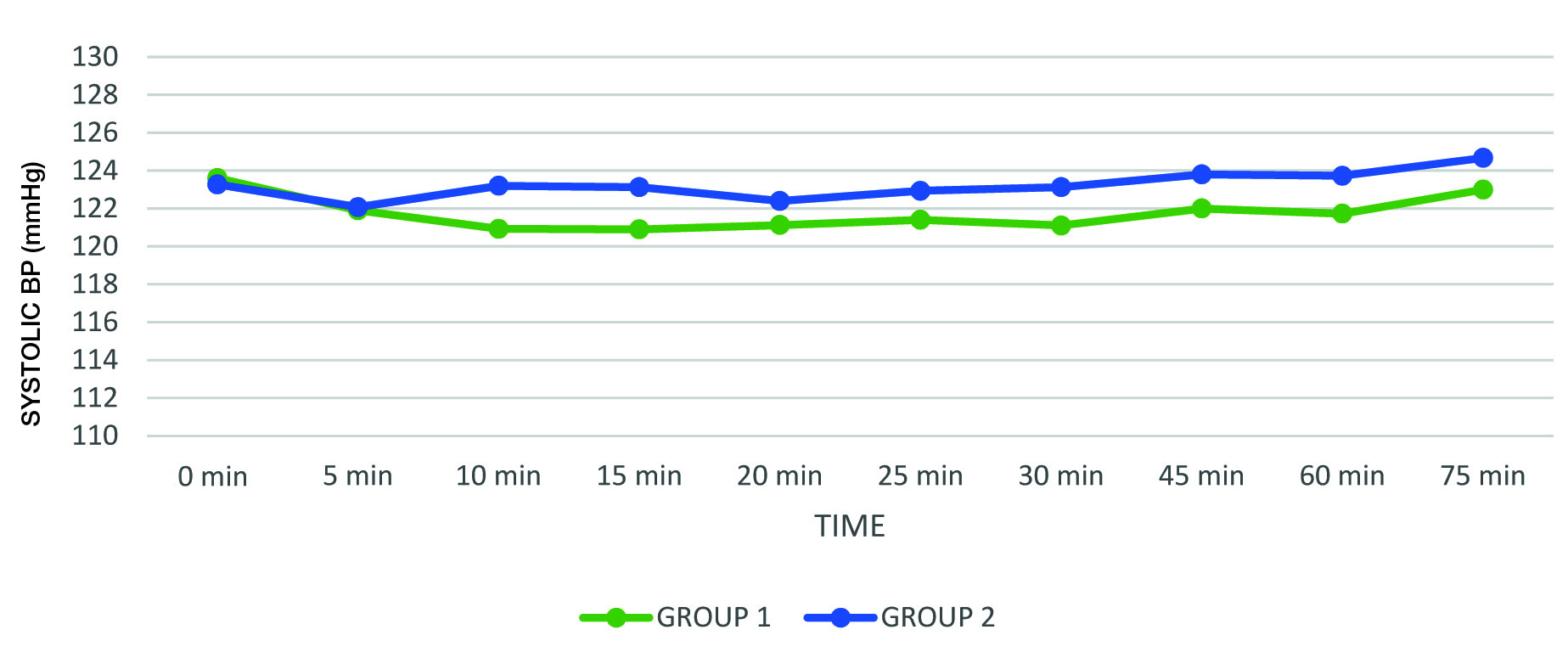
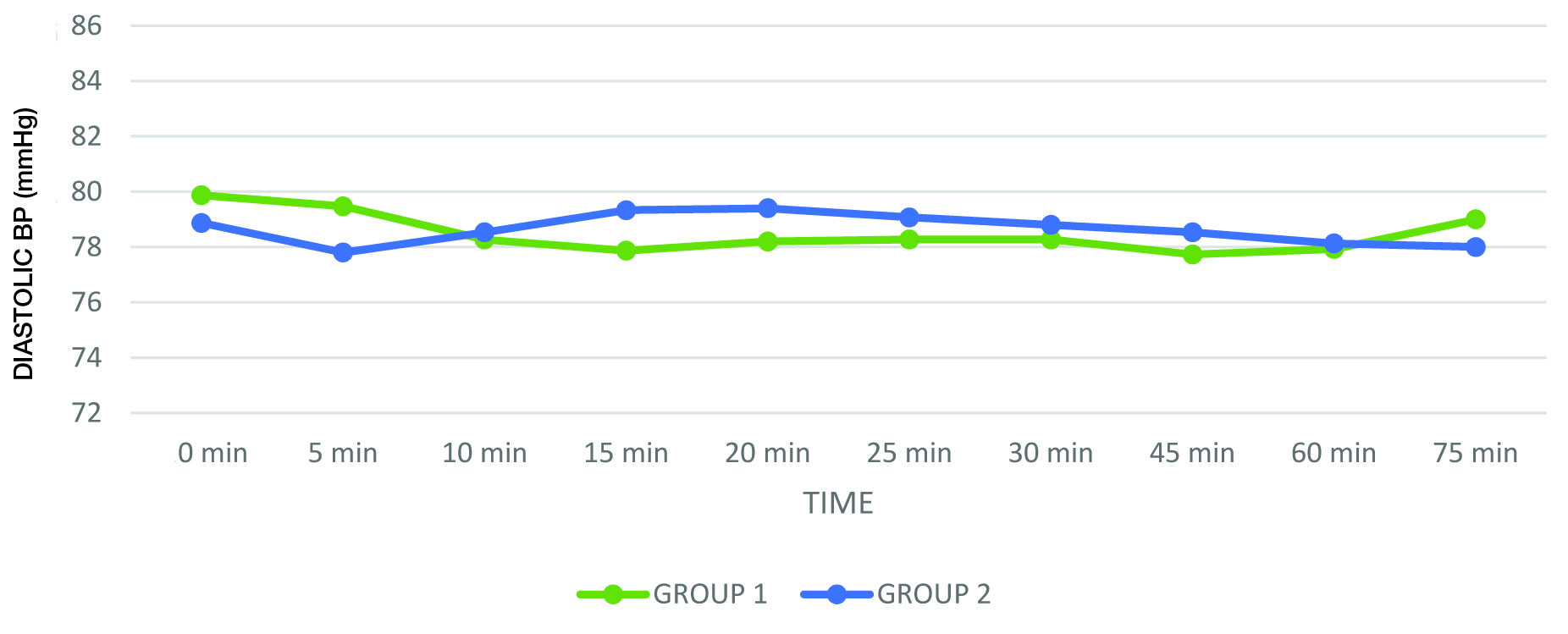
There was no statistically significant difference in heart rate, systolic and diastolic blood pressure on addition of dexamethasone to 0.5%levobupivacaine [Table/Fig-3,4 and 5].
Comparison of heart rate at different time intervals in group I and II.
Comparison of systolic blood pressure at different time intervals in group I and II.
Comparison of diastolic blood pressure at different time intervals in group I and II.
Discussion
Upper limb orthopedic surgeries are known to cause severe postoperative pain. Supraclavicular Brachial plexus block is conducted with anaesthetic agents for upper limbsurgeries and is not only an anaesthetic method that allows easier homeostasis control duringsurgery, but also allows easier postoperative pain control.
It is desirable both for surgeons and for anaesthesiologists to have prolonged analgesia. One of the believed mechanisms of dexamethasone is to specifically inhibit nociceptive C-fibre transmission. This suggests that dexamethasone may have a direct effect on nerve transmission [3]. Persec et al., have evaluated low-dose dexamethasone in conjunction with plain levobupivacaine for brachial plexus blockade at the supraclavicular level [9].
Dexamethasone is not known to have any imminent effect on heart rate. Complications with a single dose of dexamethasone are rare and previous studies have determined that short-term use of dexamethasone was safe.
In the present randomized, double blind study, on comparison of heart rates, systolic and diastolic blood pressure in both groups at different time intervals, no statistically significant difference was observed. None of the patients had bradycardia or tachycardia, hypertension or hypotension following administration of dexamethasone along with local anaesthetic agent. Our findings corroborated with that of Choi et al., Persec et al., and Shreshtha et al., who also found no significant difference in haemodynamic parameters on addition of dexamethasone to LA [3,9,10].
In the present randomized, double blind study, we demonstrated that the addition of dexamethasone to 0.5% isobaric levobu-pivacaine in supraclavicular brachial plexus block results in faster onset of sensory and motor blockade as well as prolonged duration of sensory and motor blockade which is generally consistent with previous studies, but direct comparisons are difficult because of the variety of local anaesthetic mixtures used, different blocks studied and different methods of evaluating block duration [11–13].
Shrestha et al., confirmed that addition of dexamethasone leads to significantly faster onset of action and prolonged duration of analgesia for brachial plexus block, without any unwanted side effects [8]. However, Movafegh et al., observed that the onset times of sensory and motor block were similar on adding dexamethasone to Lidocaine in Axillary Brachial Plexus Blockade [14]. But, the duration of sensory (242±76 versus 98±33 min) and motor (310±81 versus 130±31 min) blockade were significantly longer in thedexamethasone than in the control group (p < 0.01).
Islam et al., concluded that on adding dexamethasone to local anaesthetics in brachial plexus block, the onset occurs significantly earlier and duration is markedly prolonged. No unwanted side effects were noted [11].
Biradar et al., conducted a prospective randomized, double blind study to evaluate the effect of dexamethasone added to lidocaine in supraclavicular brachial plexus block [12]. The onset of sensory and motor blockade was significantly more rapid in the dexamethasone group than in the control group (=0.001). The duration of sensory and motor blockade was significantly longer in the dexamethasone group than in the control group (p=0.001).
In the present study, at 12 hours postoperative interval, 24 (80%) of 30 patients in Group-1 complained of pain in contrast with Group-2, where none of the patients complained of pain at 12 hours postoperative interval. (Chi-square test p-value = 0.03).
Thus, addition of dexamethasone decreases postoperative total analgesic use. Similar results were also shown by Persec et al., Shrestha et al., Islam et al., Tandoc et al., and by many other authors [9–11,15].
Persec et al., concluded that using single-shot low-dose dexamethasone in a mixture with levobupivacaine results in prolonged analgesia duration and less analgesic use compared with levobupivacaine alone [9].
Conclusion
To conclude, the addition of 8mg of dexamethasone to 0.5% isobaric levobupivacaine effectively and safely shortens the onset of sensory and motor blockade, increases the duration of sensory and motor blockade and increases the duration of postoperative analgesia without any haemodynamic disturbances.
*SS- Statistically Significant