Classical Cases of Lymphangioma – As Multiple Vesicular Eruptions
Anju Devi1, Anjali Narwal2, Achla Bharti Yadav3, Virender Singh4, Ambika Gupta5
1 Assistant Professor, Department of Oral Pathology, Pt. B D Sharma University of Health Sciences, Rohtak, Haryana, India.
2 Associate Professor, Department of Oral Pathology, Pt. B D Sharma University of Health Sciences, Rohtak, Haryana, India.
3 Demonstrator, Department of Oral Pathology, Pt. B D Sharma University of Health Sciences, Rohtak, Haryana, India.
4 Professor, Department of Oral & Maxillofacial Surgery, Pt. B D Sharma University of Health Sciences, Rohtak, Haryana, India.
5 Associate Professor, Department of Oral Medicine & Radiology, Pt. B D Sharma University of Health Sciences, Rohtak, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anju Devi, Assistant Professor, Department of Oral Pathology, Pt. B D Sharma University of Health Sciences, Rohtak, Haryana, India.
E-mail: anjukr24@gmail.com
Lymphangiomas are uncommon congenital hamartomas of the lymphatic system, usually diagnosed in infancy and early childhood. They are rarely situated in oral cavity and most commonly identified on the anterior two-thirds of the tongue. Though rarely seen in the oral cavity, lymphangiomas are the entities which should be taken into consideration by the clinician while examining vesicular lesions of the oral cavity. Early recognition is of utmost importance for the initiation of proper treatment and to avoid serious complications. We hereby report two classical cases of lymphangioma of the buccal mucosa with multiple vesicular eruptions, a rare site.
Buccal mucosa, Hamartomas, Lymphatic vessels
Case Report
Case-1
A 17 year old female patient reported to the Department of Oral Medicine and Radiology, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India, with a chief complaint of swelling on left side of the face. Patient gave a history of trauma 12 years back on the same site, after which swelling appeared. Initially, swelling was smaller and gradually increased to present size. Swelling was asymptomatic except difficulty in chewing.
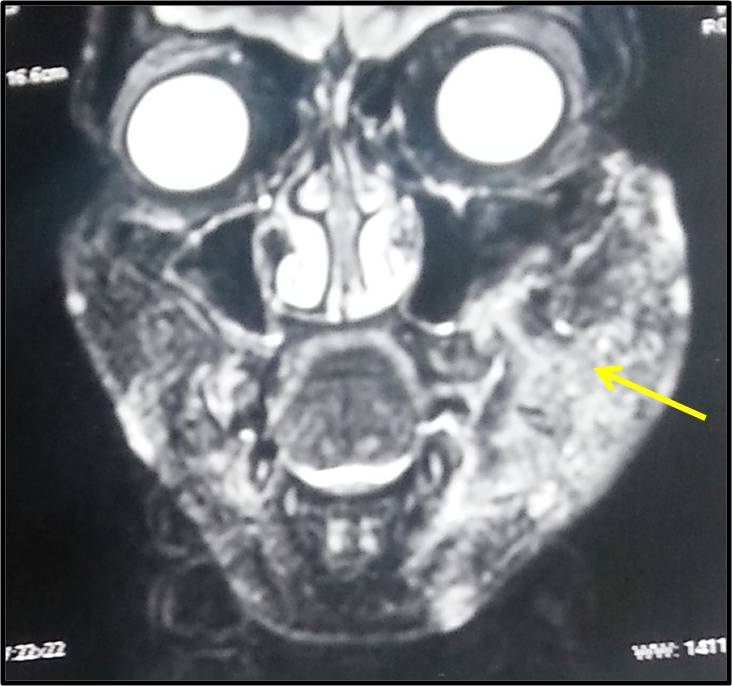
On extraoral examination, a diffuse swelling measuring 5x4cm2 (approx.) was present on left cheek causing facial asymmetry. It was soft, compressible and non tender on palpation. Intraorally, an erythematous area with transparent vesicles was present over left buccal mucosa involving the retromolar region [Table/Fig-1]. Magnetic Resonance Imaging (MRI) revealed left facial hypertrophy due to increased subcutaneous fat showing focal edema/infiltration [Table/Fig-2]. After thorough clinical and radiological examination, provisional diagnosis of lymphangioma or hemangioma was made.
Clinical photograph showing erythematous area with transparent vesicles.

MRI (coronal view) revealing hyperintense areas with indistinct margins in left subcutaneous tissue (arrow).
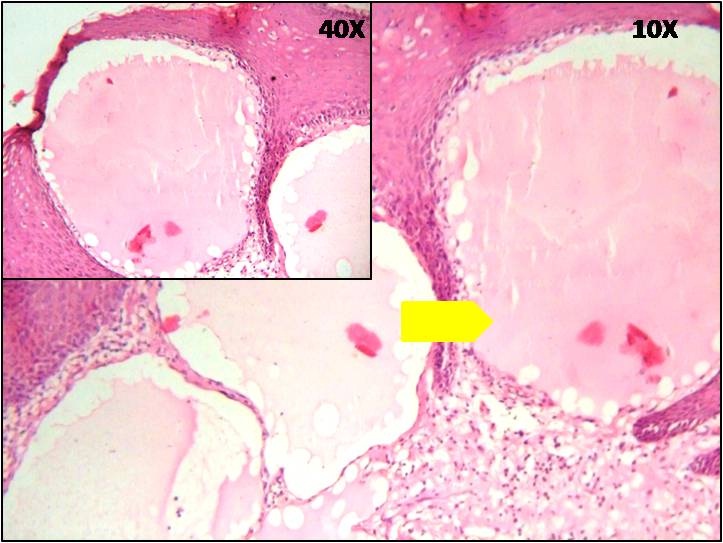
To confirm the diagnosis, an incisional biopsy was executed. Microscopic section revealed numerous endothelium lined dilated lymphatics containing proteinaceous fluid, characteristically located just beneath the surface epithelium. Focal aggregations of chronic inflammatory cells were evident around the lymphatic vessels [Table/Fig-3]. Histopathological examination confirmed the diagnosis of lymphangioma.
H & E stained sections showing varied size dilated lymphatic vessels
Case-2
A 6-year-old female patient reported to the Department of Oral Medicine and Radiology, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India, with a chief complaint of swelling on left side of face with blisters on soft palate and buccal mucosa for the last two months. Blisters were related with frequent episodes of bleeding and difficulty in eating and swallowing.
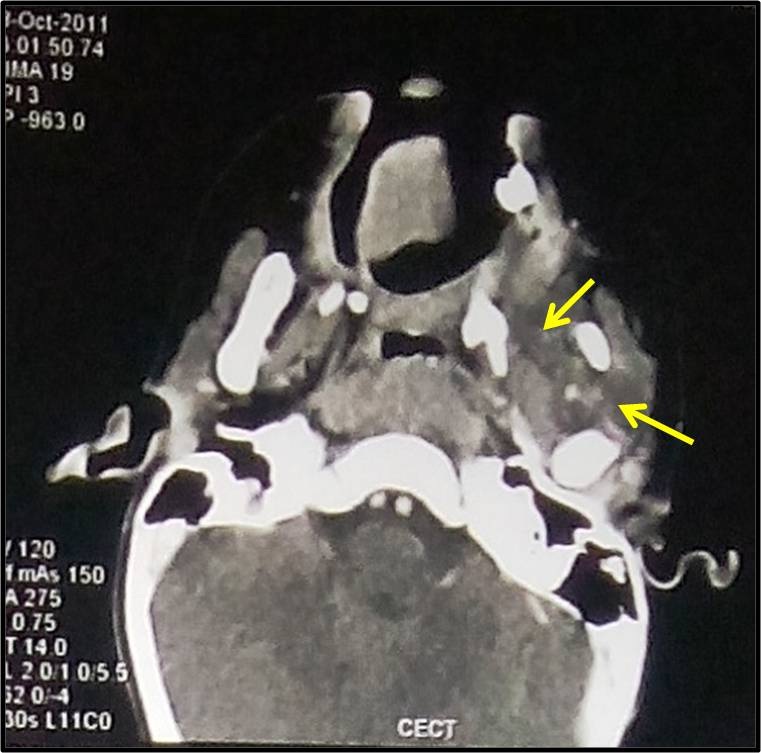
Extra-oral examination revealed a diffuse, soft, compressible swelling measuring 3x2cm2 (approx.) on left side of the cheek which was tender on palpation. On intraoral examination, exophytic vesicular lesions on left buccal mucosa involving retromolar region, extending up to the soft palate with color ranging from translucent to yellow-reddish were seen [Table/Fig-4]. Axial Computed Tomography (CT) Scan revealed a heterogeneously enhancing mass in the left infratemporal region extending to soft palate, tonsillar and cheek region [Table/Fig-5]. Clinically and radiologically, the lesion was diagnosed as lymphangioma.
Intraoral photograph showing vesicular lesions.

CT scan (axial view) revealing a heterogeneously enhancing mass in left infratemporal region extending on left side of soft palate, tonsillar and cheek region (arrow).
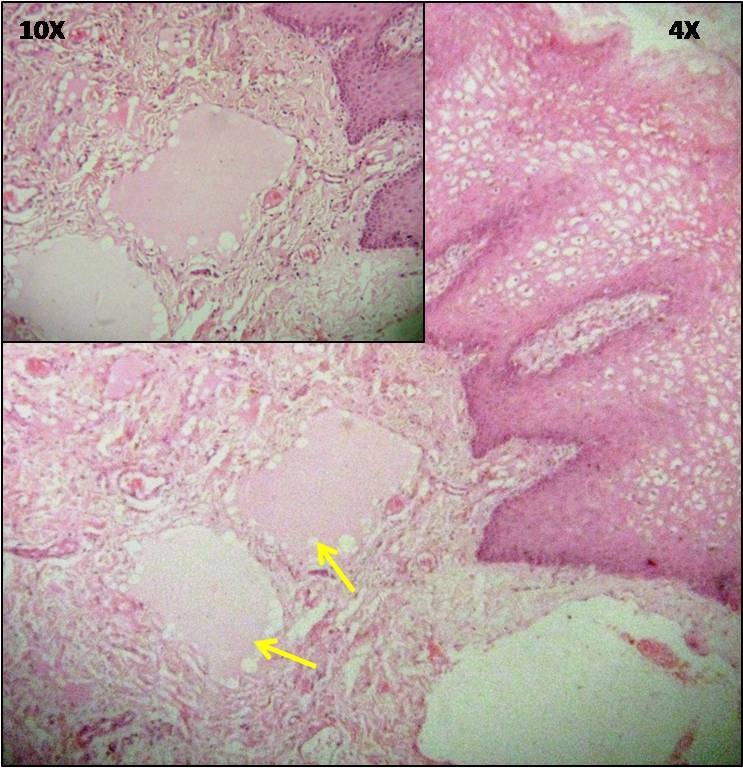
Microscopic examination showed numerous endothelium lined lymphatic channels and cavernous spaces. Eosinophilic material within these lymphoid spaces suggested lymph [Table/Fig-6]. Based on the histopathological analysis, a final diagnosis of lymphangioma was established.
H & E stained sections showing dilated lymphatic vessels (arrow) filled with proteic fluid (arrow head).
Discussion
Lymphangiomas are benign hamartomatous congenital malformations of the lymphatic system with a marked predilection for the head and neck region [1, 2]. They consist of localized centers of abnormal development of the lymphatic system [3]. It has been postulated that it develops from the sequestration of portions of the primitive embryonic lymphatic anlage. These sequestered areas never achieve efficient anastomoses with the larger lymph channels; therefore, functionally they exist as localized areas of lymphatic blockage, some appearing as lymphangiomas, others as cystic hygromas. The natural history of these lesions is one of the recurrent enlargements secondary to infection and trauma [4]. Approximately half of the cases are present since birth and about 90% develop before 2 years of age; it is rarely diagnosed in adults [5].
However, lymphangiomas rarely involve the oral cavity, although, the most commonly involved site is dorsum of tongue. Less commonly involved sites include palate, buccal mucosa, gingiva, floor of the mouth and lips [6]. Brennan et al., reviewed 49 cases of oral lymphangioma and found that 17 were located on tongue, while only one case was described at retromolar region and one at soft palate [5].
Clinically, clear vesicles are the manifestation of oral lymphangiomas. Such vesicles, which normally present a translucent hue due to the superficial location of the lymphatic vessels, may occasionally assume red or blue colour because of the rupture of blood capillary into the lymphatic inner spaces. Nodular masses of variable color may also appear clinically, especially in deeper lesions [5].
Lymphangiomas have been classified into:
Lymphangioma Simplex (Capillary Lymphangioma) consists of small, capillary sized vessels.
Cavernous Lymphangioma is composed of large, dilated lymphatic vessels.
Cystic Lymphangioma (Cystic Hygroma) exhibits large macroscopic cystic spaces [7].
The lymphatic channels are usually lined by a single layer of endothelial cells. Often all three histological types may be found in the same lesion. Among these the most common is cavernous lymphangioma and is found in areas such as the tongue and floor of mouth [6]. The case we are reporting here is also of cavernous type but the site of occurrence is buccal mucosa which is rare.
Histopathological picture of more irregular lumens lined by spaced nuclei and proteinaceous material filling the lumen differentiate lymphangiomas from cavernous hemangiomas. Immunohistochemical procedures are not a reliable means of distinguishing hemangiomas from lymphangiomas, as endothelial lining in both express factor VIII-associated antigen and CD31 [8].
In addition to surgical excision and steroid therapy, other treatment modalities for lymphangioma include radiation therapy, cryotherapy, electrocautery and laser surgery [9]. In the present case the patient is on medication, as the lesion is diffusely spread.
Conclusion
The present cases of oral lymphangiomas are of clinical interest as involving the rare site i.e., buccal mucosa with uncommon presentation. In addition, these rare case might contribute in the future studies of incidence of oral lymphangiomas.
[1]. Stanescu L, Georgescu EF, Simionescu C, Georgescu I, Lymphangioma of the oral cavityRomanian Journal of Morphology and Embryology 2006 47:373-77. [Google Scholar]
[2]. Rathan JJ, Vardhan BGH, Muthu MS, Venkatachalapathy Saraswathy K, Sivakumar N, Oral lymphangioma: a case reportJ Indian Soc Pedod Prev Dent 2005 23:185-89. [Google Scholar]
[3]. Grasso DL, Pelizzo G, Zocconi E, Schleef J, Lymphangiomas of the head and neck in childrenActa Otorhinolaryngol Ital 2008 28:17-20. [Google Scholar]
[4]. Haranal S, Naresh N, Vinuth DP, Agarwal P, Rohit M, Lymphangioma of the buccal mucosaInternational Journal of Medical Dentistry 2013 3:322-24. [Google Scholar]
[5]. Vasconcelos MG, Santos BC, Lemos LCP, Ribeiro BF, Iglesias DPP, Vasconcelos RG, Oral lymphangioma: case reportRevista Sul-Brasileira de Odontologia 2011 8:352-56. [Google Scholar]
[6]. Bindhu PR, Mathew J, Thomas P, Jayanthi P, Krishnapillai R, Cavernous lymphangioma of lower lipHealth Sciences 2013 2:1-7. [Google Scholar]
[7]. Devi SI, Gupta MK, Durga Prasad KVN, Shankar T, Majid J, Lymphangioma of soft palate: a case reportJ of Evolution of Med and Dent Sci 2014 3:13607 [Google Scholar]
[8]. Yoganna SS, Gowda R, Prasad R, Sekar B, Oral lymphangioma of the buccal mucosa a rare case reportJ Pharm Bioallied Sci 2014 6(Suppl 1):S188-91. [Google Scholar]
[9]. Sargunam C, Thomas J, Raneesha PK, Cavernous lymphangioma: two case reportsIndian Dermatology Online Journal 2013 4:210-12. [Google Scholar]