The developing knowledge of neurology fostered the concept that pain was mediated by specific pain pathways and was not simply a result of excessive stimulation of the special senses. In recent years, however some specialization of nociceptive pathways has been identified [1]. Monheim’s has defined pain as an unpleasant emotional experience usually initiated by a noxious stimulus and transmitted over a specialized neural network to the central nervous system where it is interpreted as such [2]. Pain after oral surgical procedures is one of the most studied models in pharmacology and pain research. Sensory nociception in the oral cavity is disproportionately greater than in most other areas of the body [3].
The surgical removal of third molar under local anesthesia causes postoperative pain, swelling, trismus either as direct or immediate consequences after the clinical procedure [4]. The clinicians generally emphasize the necessity for better control over pain, swelling and trims in patients who undergo third molar surgery. Many patients do report suffering from acute pain after surgical intervention [5].
The various methods used to control post-operative pain are local anaesthetic block, opioids, non-steroidal anti-inflammatory drugs or their combination [6].
Non-Steroidal Anti-Inflammatory Drugs (NSAID) such as diclofenac potassium and ibuprofen has altered the management of postoperative pain in oral and maxillofacial surgery [7]. The mechanisms postulated for the efficacy of NSAID when administered prior to surgical trauma are that they have a pharmacokinetic nature. The administration of NSAID prior to onset of pain, the drug absorption begins and therapeutic blood level will be achieved. The presence of a cyclooxygenase inhibitor at the surgical site may limit the production of prostaglandins and prostacyclin’s associated with hyperalgesia and edema [4,5].
Pre-emptive analgesia on the basis of clinical observations at the beginning of the previous century was discovered by Crile [8].
Pre-emptive analgesia due to the analgesic drug before nociception, would be more effective than the same intervention if commenced afterwards. This advantageous effect would outlast the pharmacological duration of action of the analgesic concerned. This prevents the central nervous system from reaching a hyper excitable state known as central sensitization, in which it responds excessively to afferent inputs. This clinically implies more effective pain management, thereby reducing the postoperative pain and analgesic requirements [9].
Diclofenac sodium is a non selective cyclooxygenase enzyme inhibitor, of the aryl acetic acid group, shown to be useful in controlling postoperative pain after removal of third molars [5]. Diclofenac shows analgesic, anti-inflammatory as well as antipyretic activity. Ketorolac of pyrrole-pyrrole group of NSAIDs possesses analgesic, anti-inflammatory and antipyretic activity. Oral and parenteral ketorolac has been shown to be effective for control of postoperative pain.
Various studies have been carried out in the light of pre-emptive analgesia such as “pre-treatment” versus “post-treatment”, “pre-treatment” versus “no treatment” and “orally” versus “intravenously” administered analgesics. Comparative studies of analgesic efficacy between intramuscular analgesics for third molar surgeries are rare. To the best of our knowledge studies that compare the efficacy of intramuscular ketorolac and diclofenac sodium, have not been carried out in the past. Hence, we found it important to compare the analgesic efficacy of preoperative intramuscular injection of ketorolac and diclofenac in third molar surgeries for controlling post operative pain.
Materials and Methods
Source of data: A double blind randomized study was carried out on 50 patients scheduled for surgical removal of third molar surgery in the Department of Oral and Maxillofacial surgery at Dr. D.Y. Patil Dental College and Hospital, Pimpri, Pune between September 2008 and December 2010.
Sample size: A total of 50 patients fulfilling the inclusion criteria listed below were included in the study. A pilot study was conducted with 12 patients, four in each group with 95% confidence level and hence the sample size of 50 was derived. The institutional review board with ethical clearance was taken before the study started.
The inclusion criteria were patients with bilateral impacted third molar with similar difficulty index in healthy young adults of both genders belonging to age group of 20– 30 years, willing to give written informed consent were included.
Exclusion criteria were patients with infection, systemic condition, on anti-inflammatory and on anticoagulant therapy. The study was conducted with institutional ethical board clearance and all patients written informed consent for the surgical procedure were obtained.
A thorough history was recorded followed by a detailed clinical examination. The findings were entered accordingly into the proforma. Preoperative radiological examination consisted of intra oral periapical radiograph, Ortho Pantamo Graph (OPG). The laboratory investigations of complete haemogram, bleeding time, and clotting time were carried out for all those patients who gave their consent to become a part of the study.
The analgesic drugs used in the study were intramuscular injection Ketorolac 30mg and intramuscular injection Diclofenac 75mg. The rescue medication used in the study was tablet ibuprofen 400mg
Study design: In Group A, were the patients who underwent surgical removal of third molar of one side in the first session. Group B included those patients who underwent surgical removal of the third molar of the contralateral side after three to four weeks in the next session.
Group A – 25 patients received 30mg ketorolac intramuscular injection 30 minutes preoperatively in the deltoid region.
Group B – 25 patients received 75mg diclofenac sodium intramuscular injection 30 minutes preoperatively in the deltoid region.
The allocation ratio of 1:1 with parallel study group design of randomized control trial was adapted. The concealment pouches were used for the delivery of the drugs and randomly allocated by lottery system. They were injected in a double blinded manner where the principal investigator and patient were blinded. The group which received the injection and those assessing were blinded and hence single operator performed the surgeries.
The standard protocol for surgical removal of third molar was followed. The modified wards incision for the third molar surgery respectively was placed in the region of the third molar to be removed with no. 15 surgical blades. The buccal bone guttering was done with carbide bur no.8 and no. 703. The tooth was sectioned and elevated out. With 3-0 silk, interrupted sutures were given. After surgical removal of third molars, patients were instructed to follow standard postoperative instructions. The patients were instructed to take ibuprofen 400mg when pain becomes unbearable and maintain record of the number of tablets consumed over three days postoperatively.
Post-surgical assessment was done on the basis of three key end points.
1. Severity of the patient’s pain perception was assessed by a visual analogue scale; 100mm in length, where ‘0’ is marked as ‘no pain’ and ‘4’ is ‘marked as most severe pain imaginable’. The patients were asked to record pain on the visual analogue scale for the first 12hrs from the time the patient reports of severe pain after the surgery.
2. The median time taken for re-medication that is time from the end of the surgery to the time at which rescue medication ibuprofen 400mg was necessary for the patient.
3. The total analgesic consumption in the postoperative period, for the three days after surgery was calculated.
Statistical Analysis
The data obtained from the patients was analyzed by using statistical computer software SPSS 11.0 (Statistical package for social sciences 11.O version of SPSS Inc.). The data obtained from the VAS and number of tablets, the mean was evaluated with paired t test.
Results
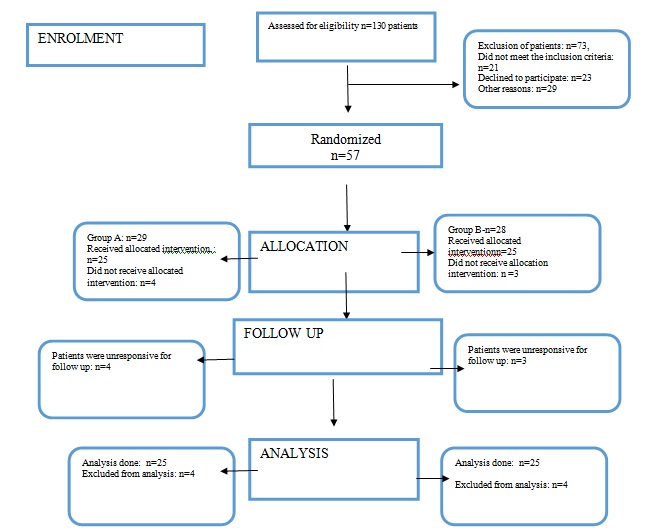
The CONSORT flow diagram of the patients are described in [Table/Fig-1]. The patients had a mean age of 26.44 years with male patients’ more than female patients. Each patient was undertaken for surgical removal of impacted mandibular third molar on two different occasions for either side with a time gap of three weeks. Diclofenac sodium or ketorolac was administered 30minutes before start of surgery. All patients were evaluated postoperatively for 12 hours after surgery for maximum time duration during which the patient was free from pain. On perception of unbearable pain the patients were prescribed rescue medication tablet ibuprofen 400mg and they were asked to maintain a record of the number of tablets consumed over three days. The pain was assessed using a visual analogue scale. The patients were evaluated postoperatively for three days for the number of rescue medication taken.
CONSORT flow diagram of patients.
The visual analogue scale was filled by the patient for 12hours after surgery. The paired t test was used to compare the pain recorded on the visual analogue scale between intramuscular diclofenac sodium and ketorolac. The results are described in [Table/Fig-2].
Post operative pain evaluation for 12 hours post operatively.
| Pain score at different hours | Mean score | Std. Deviation | Wilcoxon Signed Ranks Test Z | p |
|---|
| Hour 1 | Gr-A | 0.22 | 0.465 | 0.211 | 0.833 |
| Gr-B | 0.24 | 0.517 |
| Hour 2 | Gr-A | 0.30 | 0.505 | 1.079 | 0.280 |
| Gr-B | 0.42 | 0.702 |
| Hour 3 | Gr-A | 0.66 | 0.745 | 1.824 | 0.068 |
| Gr-B | 1.00 | 1.050 |
| Hour 4 | Gr-A | 1.14 | 1.010 | 1.073 | 0.283 |
| Gr-B | 1.30 | 1.111 |
| Hour 5 | Gr-A | 1.38 | 1.159 | 1.988 | 0.047 * |
| Gr-B | 1.00 | 1.125 |
| Hour 6 | Gr-A | 1.00 | 1.088 | 1.183 | 0.237 |
| Gr-B | 0.78 | 0.887 |
| Hour 7 | Gr-A | 0.94 | 1.077 | 0.999 | 0.318 |
| Gr-B | 0.72 | 0.904 |
| Hour 8 | Gr-A | 0.80 | 1.088 | 0.310 | 0.757 |
| Gr-B | 0.84 | 1.017 |
| Hour 9 | Gr-A | 0.56 | 0.951 | 0.945 | 0.345 |
| Gr-B | 0.68 | 0.935 |
| Hour 10 | Gr-A | 0.56 | 0.787 | 0.854 | 0.393 |
| Gr-B | 0.66 | 0.961 |
| Hour 11 | Gr-A | 0.22 | 0.545 | 2.092 | 0.036 * |
| Gr-B | 0.52 | 0.863 |
| Hour 12 | Gr-A | 0.14 | 0.405 | 1.498 | 0.134 |
| Gr-B | 0.28 | 0.573 |
*p-value significant –Paired t test
The maximum time taken for pain perception for the patient in Group A (Ketorolac) was 5.48hours and in Group B (Diclofenac sodium) was 4.98hours. The p-value was 0.235 which was not significant. This means that both medicines had almost same pain free immediate post operative period [Table/Fig-3].
Comparison of the mean of the maximum time taken for pain perception.
| Group | Mean time | Std. Deviation | Paired t | p |
|---|
| Group - A | 5.48 hr | 2.278 | 1.20 | 0.235 * |
| Group - B | 4.98 hr | 2.519 | | |
p* value Paired t test – not significant
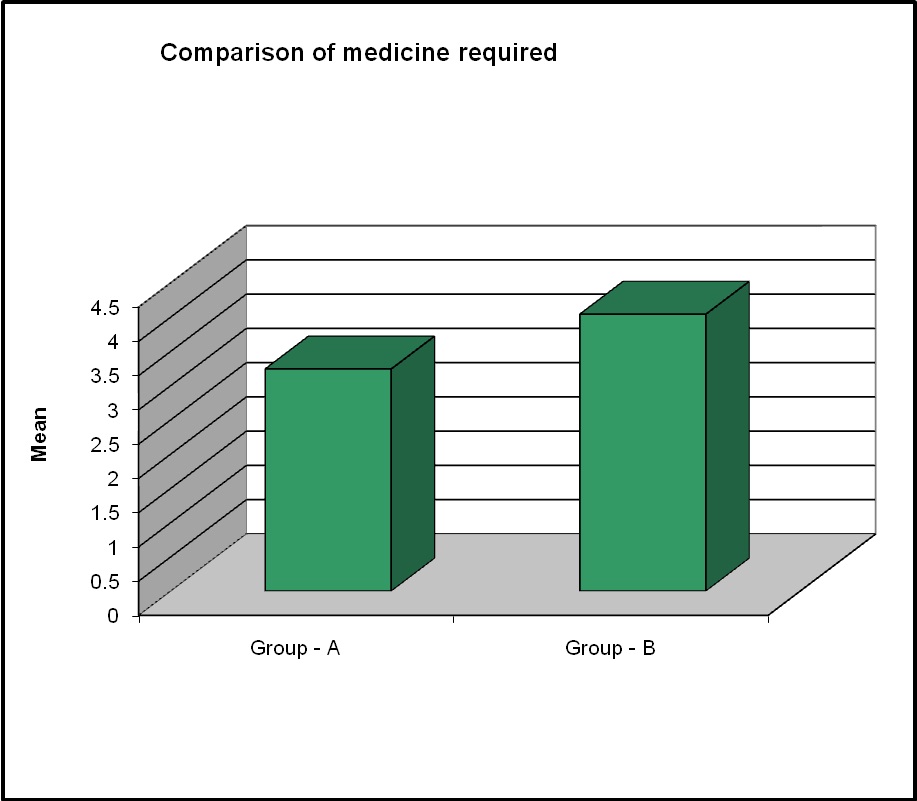
The mean number of tablets that is rescue medication taken by the patients in the first three post-operative days was 3.24 in Group A (Ketorolac) and 4.04 in Group B (Diclofenac sodium). The values were compared using the paired t test. The p-value was 0.004, which was significant [Table/Fig-4].
Comparison of number of rescue medication in both the groups.
(Paired t test)
Discussion
The third molar surgery postoperative squealae are pain, trismus and swelling. The incidence and severity of these complaints vary from patient to patient, and do not appear to be related to the degree of impaction [10]. The surgical extraction of impacted mandibular third molar induces moderate to severe pain, and has been used as an excellent clinical trial model for pain studies [11].
It is well documented that pain after removal of impacted third molars is of short duration and reaches its maximum intensity in the early postoperative period [12]. The pain experience is especially useful for evaluating the efficacy of single doses of analgesics. Single dose studies also facilitate investigations between pharmacokinetic variables of the drug and efficacy. Such information may provide an insight into the pharmacodynamics of certain analgesics together with pharmacokinetic variables that could determine their efficacy. Many clinical studies regarding the value of pre-emptive analgesia have been carried out according to the administrating times, kinds of drug and dosing routes [6,11,12] [Table/Fig-5]. The trials coincident with the “pre-emptive analgesia” were about different administration times and the results were varied.
Comparison of number of rescue medication in both the groups.
| S. No. | Author Details | Study Design | Inference | Relevance in Our Study |
|---|
| 1. | Hutchison et al., [13] | 50 patients received placebo/ piroxicam 40mg, 2.5 hrs before third molar surgery | Patients did not require opiod analgesia postoperatively. The rescue medication paracetomol was required less | Group with Ketoralac received less rescue medication |
| 2. | Walton GM et al., [14] | Double blind study to compare the efficacy of intramuscular ketoralac and oral ketoralac | Both analgesic preparations of ketoralac were more effective than placebo | The efficacy of intramuscular ketoralac was compared with diclofenac |
| 3. | Bridgman JB et al., [15] | Double blind randomized study, to study the efficacy of intramuscular diclofenac sodium in 21 patients undergoing third molars | Preemptive analgesia effects of diclofenac sodium non significant | This was found similar in our study |
| 4. | Velasquez et al., [16] | Double blind pilot study between ketoprofen 100mg and 75mg diclofenac who received pre-emptively before third molar surgery | Intramuscular ketoprofen 100 mg more effective than intra muscular diclofenac | Ketoralac proved better as premptive analgesic in our study |
| 5. | Shah R et al., [17] | Prospective triple blind placebo controlled randomized trial in patients undergoing third molar surgery to evaluate efficacy of diclofenac sodium | Diclofenac sodium proved to be effective as premptive analgesia | Diclofenac sodium as preemptive analgesia was not significant |
| 6. | Gopalraju P etal., [18] | Comparative randomized prospective study to evaluate the preoperative efficacy of intravenous dose of either tramadol or ketoralac which was given 10 min prior to surgery | Premptive injection of 30mg ketoralac reduced the postoperative pain sequelae of asymptomatic third molar removal | Ketoralac intramuscular was found to be effective |
| 7. | Kumar R et al., [19] | Randomised, double-blind, cross-over trial, 15 healthy, young patients undergoing surgical removal of bilateral, impacted, third-molar teeth received the analgesic tramadol 50mg, as a single dose, either 2 hours prior or immediately before the surgical procedure | There were no differences in the post-operative pain levels or degree of trismus between the two methods of administration of tramadol (p>0.05), suggesting absence of any pre-emptive analgesic effect for the drug in the dose studied | Tramadol not used in our study. |
| 8. | Ong KS et al., [20] | Double blind, randomized, placebo-controlled study in 34 patients. One side was pretreated with intravenous ketorolac 30mg, before surgery followed by placebo injection after surgery, and for the other side, the patient was given placebo injection before surgery and post-treated with intravenous ketorolac 30mg, after surgery. | Pretreatment with intravenous ketorolac has a preemptive effect for postoperative third molar surgery and extended the analgesia by approximately 2hrs. | Ketoralac had a prolonged analgesia compared to diclofenac |
| 9. | Ong KS et al., [21] | Comparative study in 64 patients for analgesic efficacy of a single-dose of preoperative intravenous tramadol versus ketorolac in preventing pain after third molar surgery | Preoperative intravenous ketorolac 30mg is more effective than tramadol 50mg in the prevention of postoperative dental pain | We used intramuscular ketoralac to compare with diclofenac |
| 10. | Morse Z et al., [22] | Double blind randomized comparative study, to compare the pre-emptive analgesic effect of rofecoxib, with ibuprofen for mandibular third molar surgery | Ibuprofen is as effective as rofecoxib for the relief of acute postoperative pain following third molar surgery when used pre-emptively | Ibubrofen was used as rescue medication post operatively and ketoralac group received less rescue medication |
Jung YS et al., conducted a study to compare the efficacy of analgesics administered at three different times. The oral NSAID was first administered one hour preoperatively, or one hour postoperatively, or no scheduled administration pre- or post-surgery. The results implied that scheduled postoperative analgesics before pain development were adequate for postoperative analgesia without preoperative administration [8]. The preoperative dose was effective in our study for ketorolac group.
Surgical trauma initiates the peripheral inflammatory reaction which is the cause for post operative pain. Therefore, NSAIDs have been reported to be effective for the pain after surgical extraction and have been used for the effectiveness of pre-emptive analgesia concerning administration time in numerous reports [12]. The PubMed search of the last 20 years has been described in comparison to our study in [Table/Fig-5].
Various studies have been carried out individually on ketorolac and diclofenac sodium in controlling post operative pain. But to the best of our knowledge no studies have been carried out comparing the analgesic efficacy of intra muscularly administered ketorolac and diclofenac sodium.
1) Timing of administration: Ong KS, Guillien AP, Lau SL with their studies proved the positive effect of premedication with analgesic before third molar surgeries [20,10,23].
A study conducted by Dunn GL et al., in which zomiperac was compared as a preoperative and postoperative analgesic medication. They concluded that pre-emptive analgesia was effective when administered 30 minutes prior to surgery [24].
So based on the above mentioned studies pre operatively administered analgesic is more advantageous than post operative analgesics in terms of reducing the intake of rescue medication. Hence, we selected the administration of analgesics 30 minutes prior to surgery.
2) Time gap between surgeries: There is a controversy regarding the use of crossover designs for clinical trials because statisticians were concerned about the possibility of spurious conclusions resulting from carryover effects. According to the earlier studies by Jones B et al., Seymour RA et al., carryover effects can be prevented by separating the study periods by one month. This time gap is also known as the washout period [25,26].
In our study, a washout period of minimum three weeks was given between the two surgical interventions.
3) Choice of NSAID
a) Ketorolac: Ketorolac is a potent analgesic used in oral surgery. Ong KS have assessed the efficacy of ketorolac in third molar surgeries and found it to be effective in controlling post operative pain [21].
In our study it was seen that ketorolac was better than diclofenac sodium. The mean time at which maximum pain perceived was 5.48 hours; this was slightly longer than for diclofenac sodium. The pain score at every hour was less for ketorolac in comparison with diclofenac sodium except at the 5th, 6th, 7th hour, where diclofenac sodium had significantly lesser pain scores. The pain score of the group receiving ketorolac was significantly lesser at the 11th hour. The consumption of rescue medication was significantly lesser in the group which took ketorolac as pre-emptive analgesia.
Pozos-Guillen compared pre-emptive analgesic effect of tramadol against post treatment analgesic effect of tramadol. They concluded that pre-emptive use of tramadol is an alternative for the acute pain treatment after the removal of an impacted mandibular third molar carried out under local anaesthesia [27].
b) Diclofenac Sodium: In studies conducted by Westhuijzen AJ, Bailey BMW concluded that diclofenac sodium provides pain relief after third molar surgeries [28,29].
Administration of preoperative intra muscular diclofenac sodium provided analgesia on an average of 4.9 hours after surgery. In comparison with ketorolac, the patients receiving diclofenac sodium have significantly less pain scores at 5 hours post operatively that is 1 as compared to ketorolac 1.38. But at 11 hours post operatively the pain score of patients who received diclofenac sodium show higher pain score than ketorolac. The consumption of rescue medication by patients who received diclofenac sodium was significantly higher than ketorolac.
4) Postoperative pain: Previous studies by Seymour RA and Szmyd L stated that after third molar surgery, pain usually occurs during the first 12 hours, with peak intensity after 6-8 hours when a conventional local anesthetic is used [26,30].
The intake of rescue medication in the group of patients who took ketorolac as premedication was significantly less as compared to those who took diclofenac sodium as premedication.
No adverse effects were reported by any patient during the course of the study.
Limitation
The patient had to receive an injection at the deltoid region was the limitation during the study. The pre-emptive effect of ketorolac in patients undergoing third molar extraction will certainly reduce the postoperative pain is the clinical implication of the study. To conclude the immediate postoperative pain free period provided by both the analgesics, ketorolac and diclofenac sodium are almost same.
Conclusion
The parenteral ketorolac results in prolonged analgesia over long term period. This can be seen in terms of consumption of rescue medication, which is significantly less in ketorolac than in diclofenac sodium. Therefore, pre-emptive analgesia with ketorolac should be considered as an adjunctive before surgical procedures. Effectiveness with these intramuscular injections with more prospective studies should be encouraged for a much extensive, qualitative as well quantitative assessment of the ideal pre-emptive analgesic.
*p-value significant –Paired t test
p* value Paired t test – not significant