Respiratory Syncytial Virus (RSV) is one of the most common causes of viral ARTI. It predominantly manifests as bronchiolitis followed by pneumonia [1,2]. According to WHO reports the estimated prevalence of RSV globally is 64 million cases and 1,60,000 deaths every year. RSV related pulmonary disease plays a major role in childhood mortality and morbidity [3]. The mortality rate amongst children hospitalized with RSV infection ranges from 0 -33%. Morbidity and mortality from RSV is more in patients with underlying illness [4]. Detection of RSV using rapid, sensitive and specific diagnostic test has further confounded the role of RSV in childhood respiratory tract infections [5].
The prevalence rates in northern and western parts of India have been studied, however, there are very few studies that determine the occurrence in Southern parts of India [6–8].
Hence, the present study was undertaken to estimate the occurrence of RSV related respiratory tract infection in pediatric age group in our set up and to assess the risk factors and clinical features associated with RSV infection.
Materials and Methods
A descriptive cross-sectional study was carried out on pediatric inpatient groups (0-5 years) in Father Muller Medical College over a period of 2 years from July 2011 to July 2013. A total of 100 patients were screened for RSV infection. Children presenting with fever, cough, rhinorrhea, sore throat and with evidence of fast breathing, wheezing or apnea or stridor were included in the study. Nasopharyngeal aspirates were collected from the selected patients after informed consent. The demographic profile of children, clinical symptoms and risk factors were documented. Nasopharyngeal aspirate was processed for RSV DFA smear preparation. Procedure supplied with the kit was followed. (Light Diagnostics, Millipore, USA).
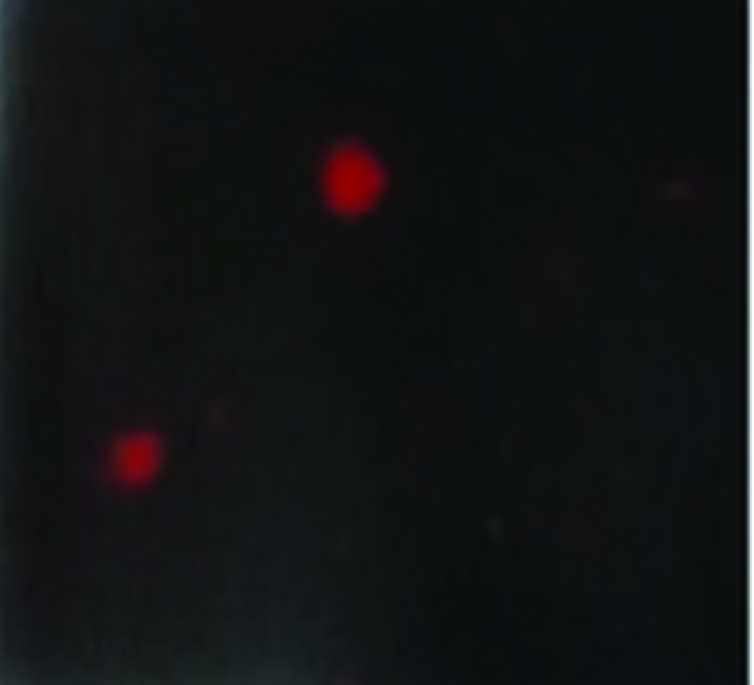
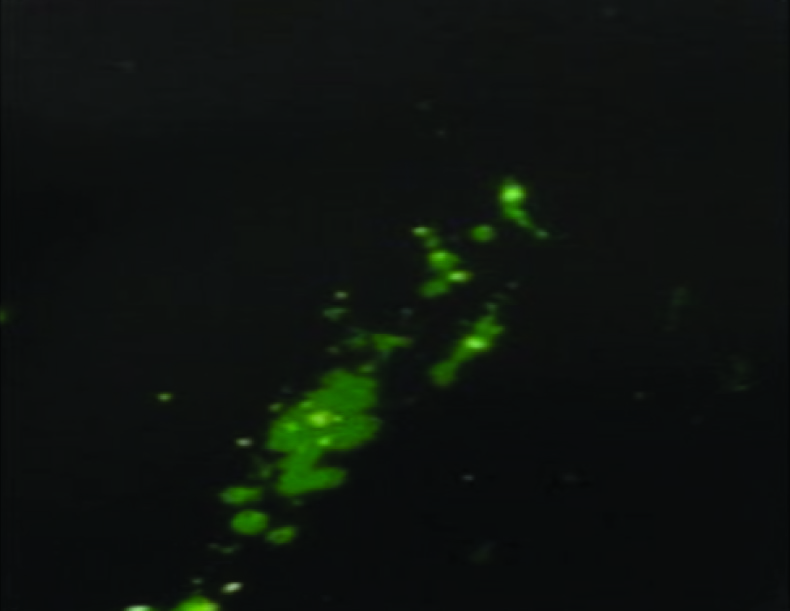
Slides were examined by fluorescence microscopy with appropriate filter combination for FITC (excitation peak 490nm, emission peak 520nm) and were examined for cells with apple green fluorescence first under 100 to 200x, then detailed examination under 400x. These slides were then compared with positive and negative control slides supplied with the kit. Specimens showing one or more cells with characteristic cytoplasmic globular speckled fluorescence were considered positive for RSV [Table/Fig-1]. Specimens in which at least 20 epithelial cells with no fluorescence was observed was considered negative for RSV [Table/Fig-2]. Specimens with fewer than 20 cells with no fluorescence were rejected for DFA analysis. If the positive and negative control slides could not be clearly distinguished the test was considered invalid. Perinuclear and or diffuse cytoplasmic staining was considered nonspecific [Table/Fig-3]. (Ref: Based on the criteria mentioned in the kit Light Diagnostics, Millipore, USA).
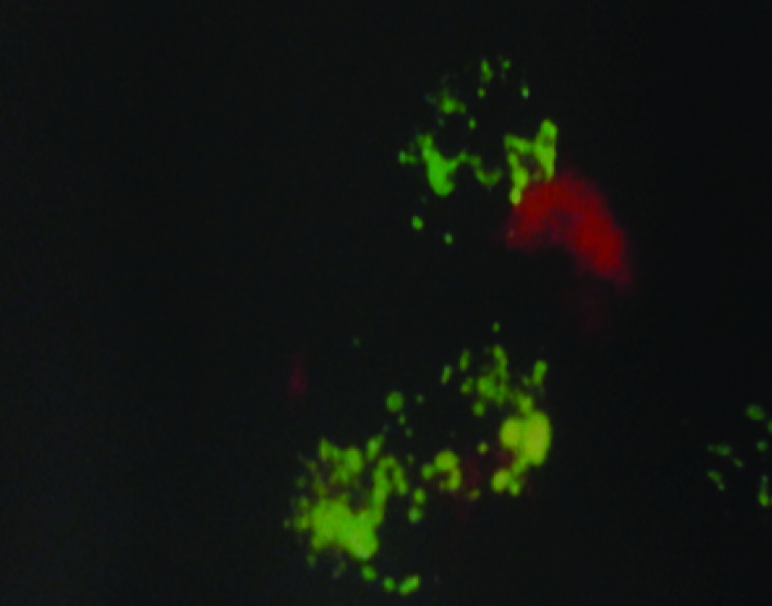
Nonspecific fluorescence.
Results
Out of the 100 samples tested 22 patients were positive for RSV and 78 patients were negative for RSV. [Table/Fig-4] shows that RSV infection was more common in the age group of 1-5 months (31.8%).
Age distribution of RSV positive patients.
| Age group | No of patients |
|---|
| Below 1 months | 2 |
| 1-5 months | 7 |
| 6-12 months | 5 |
| 13-24 months | 4 |
| 24-36 months | 1 |
| above 36 months | 3 |
The mean age group of RSV positive patients was 12 months and the male to female ratio of RSV positive patients was 1.75:1.
Approximately 81.8% of RSV positive children had a cough at admission but no statistically significant difference was observed when compared to the RSV negative group (83.1% vs. 81.8%, p >0.05). Two clinical parameters showed significantly different rates (p-value < 0.05) when comparing both the groups: wheezing and breathlessness was observed predominantly in the RSV positive group (50% vs. 10.3% and 68.2% vs. 35.7%, respectively yielding a p-value <0.05). Patients infected with RSV did not differ significantly in terms of other signs and symptoms as compared to RSV negative group. [Table/Fig-5] describes the signs and symptoms of RSV positive and RSV negative group.
Comparison of clinical features of RSV positive and RSV negative patient. *p<0.01, **p<0.001
| Clinical features | RSV positiven=22(22%) | RSV negativen=78(78%) | p-value |
|---|
| Fever | 8 (36.4%) | 41(52.6%) | 0.179 |
| Cough | 18(81.8%) | 64(83.1%) | 0.887 |
| Breathlessness | 15 (68.2%) | 28(35.7%) | 0.007* |
| Wheezing | 11(50%) | 8(10.3%) | 0.000** |
| Coryza | 3 (13.6%) | 23(29.5%) | 0.134 |
| Sore throat | 0 (0%) | 10 (12.8%) | 0.171 |
| Ear pain | 0 (0%) | 2 (2.6%) | 0.607 |
[Table/Fig-6] shows that preterm birth and congenital heart disease were significantly associated with RSV positive patients (p-value <0.005). However, no statistically significant correlation was associated with asthma, neuromuscular defect, immunosuppression and bottle fed infants (p-value > 0.05).
Comparison of risk factors between RSV positive and RSV negative patients. *p<0.01, **p<0.001
| Risk factors | RSV Positiven=22(22%) | RSV NegATIVEn =78(78%) | p-value |
|---|
| Congenital heart disease | 3(13.6%) | 1 (25%) | 0.009* |
| Asthma | 3(13.6%) | 4 (5.1%) | 0.304 |
| Neuromuscular defect | 1(4.5%) | 0 (0%) | 0.220 |
| Immunosuppression | 0(0%) | 1(1.3%) | 0.780 |
| Preterm birth | 9(40.9%) | 2 (2.6%) | 0.000** |
| Bottle fed | 2(9.1%) | 3 (3.8%) | 0.658 |
Out of the 22 RSV positive patients, majority of the patients 68.18% (15/22) had no abnormality detected and 38.18% (7/22) had findings on X-ray.
[Table/Fig-7] shows that the predominant X- ray findings among the RSV positive patients was interstitial infiltrates 18.18% (4/6) followed by hyperinflation and patchy infiltrates.
X- ray features associated with RSV positive patients.
| X – ray features | RSV positive patient’s n (%) |
|---|
| Interstitial infiltrates | 4 (18.18%) |
| Hyperinflation | 2 (9.09%) |
| Patchy infiltrates | 1 (4.54%) |
Discussion
Previous hospital based studies from India reported RSV prevalence rates that were similar to the findings in present study of 22% among children with ARTI. Bharaj et al., reported RSV prevalence of 20.3% from Northern India [6] and Yeolekar et al., reported 26% prevalence in Western India [7]. Broor et al., reported 30% prevalence of RSV in the community among children in rural North India [8].
Studies show that RSV affects mainly children during the 1st year of life [9]. According to our study, 54.5% of children were younger than 1 year old suggesting that illness caused by RSV can be severe in this age group.
Males are known to be prone to severe RSV ARTI as boys have shorter and narrower airways and are at a greater risk for bronchial obstruction in case of RSV infection [10]. In this study, the ratio of boys to girls in RSV positive group was found to be 1.75:1.
In the present study, wheezing and breathlessness were predominantly observed in RSV positive group (p-value <0.005). This is in accordance to the study done by Diniz et al., who noted that wheezing was significantly more frequent in the RSV positive group [11].
In this study, prematurity and congenital heart diseases were the two factors that independently correlated with the disease severity. Studies done by Mac Donald et al., & Navas et al., shows that infants with CHD are prone for RSV infection and have a higher mortality rates [12,13].
Studies show that premature infants are at an increased risk for RSV infection, the reason being inadequate cellular immunity and small, immature alveoli [14].
In this study, we could not demonstrate a significant association between lack of breast feeding and RSV positivity. This was in accordance with the FLIP-2 study and the Canadian PICNIC study where the protective effect of breast feeding on RSV infection could not be demonstrated [15,16].
The radiological findings in our study have shown that 18.18% of RSV-positive patients developed interstitial infiltrate. Diniz et al., found a significant correlation between viral lower respiratory tract infection and interstitial infiltrate [11].
RSV DFA has a sensitivity and specificity of 94% and 96.8% respectively and can detect RSV antigens even in conditions where the virus cannot be isolated [17].
Limitation
The possible limitation of this study was the lack of use of confirmatory test like RT- PCR or virus culture.
Conclusion
RSV infection plays a major role in childhood morbidity as is indicated by the prevalence rate in children hospitalized for ARTI. Our results also emphasize that routine testing of RSV using rapid tests can reduce the unnecessary use of antibiotics and also infection control precautions can be applied to prevent the transmission of infection to other patients and staff.