An Approach with Hybrid Segmental Mechanics
Harsh Ashok Mishra1, Raj Kumar Maurya2
1 Private Practitioner, Department of Orthodontics, Ashok Dental Hospital, Mumbai, India.
2 Graded Spl, Department of Orthodontics, Corps Dental Unit, Bhopal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raj Kumar Maurya, P8 Khulna Marg, Corps Dental Unit, S I lines, Military Station, Bhopal-462001, India.
E-mail: bracedbyraj@gmail.com
Present case report provides an insight into the hybrid segmental mechanics with treatment of 13-year-old male, considering the side effects of sole continuous arch wire sliding mechanics. Patient was diagnosed as a case of skeletal class I jaw relationship, low mandibular plane angle, class II molar relation on right and class I molar relation on left side, anterior cross bite, crowding of 12mm in upper, 5mm in lower arch. He also had proclined upper and lower anteriors by 2mm, convex profile and incompetent lips. Total treatment duration was 20 months, during which segmental canine retraction was performed with TMA (Titanium, Molybdenum, Aluminum) ‘T’ loop retraction spring followed by consolidation of spaces with continuous arch mechanics. Most of the treatment objectives were met with good intraoral and facial results within reasonable framework of time. This approach used traditional twin brackets, which offered the versatility to use continuous arch-wire mechanics, segmental mechanics and hybrid sectional mechanics.
Burstone, Sliding mechanics, ‘T’ loop
Case Report
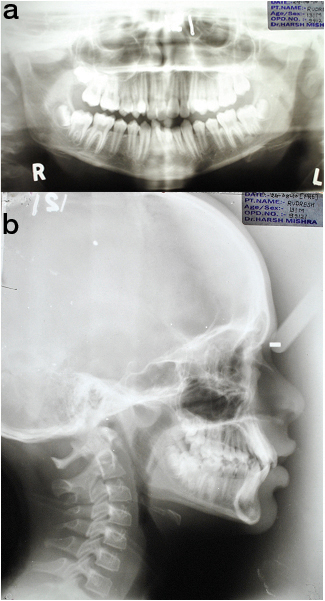
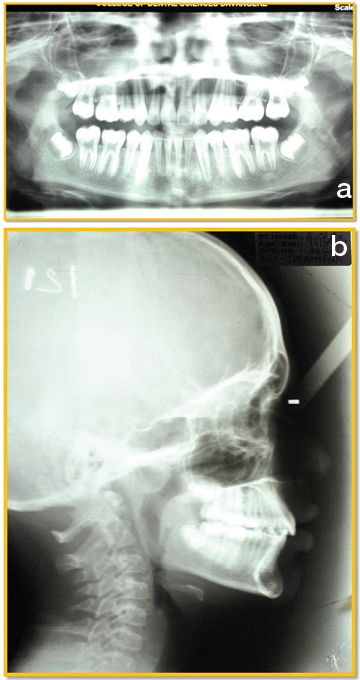
A 13-year-old, male patient presented with a chief complaint of irregularly placed upper front teeth. He was diagnosed as a case of skeletal class I jaw relationship with low mandibular plane angle, class II molar relation on right and class I molar relation on left side, anterior cross bite, crowding of 12mm in upper, 5mm in lower arch. Patient had proclined upper and lower anteriors by 2mm, convex profile and incompetent lips [Table/Fig-1a-c]. The maxillary canines were positioned buccally with significant distal tipping of root. The mandibular arch had moderate crowding with right lateral incisor lingually placed [Table/Fig-2a-e,3a&b].
Pre-treatment extra oral photograph.

Pre-treatment Intraoral photographs.

Pre-treatment ortho-pantogram & lateral cephalogram.
Treatment Objectives
De-crowd in upper and lower arch, to obtain class I molar and canine relation bilaterally and to improve smile aesthetics without significant round tripping.
Treatment Alternative
Non-Extraction with molar distalization.
Non-Extraction with proximal stripping.
Extraction line of treatment with extraction of upper and lower first premolars
Treatment Progress
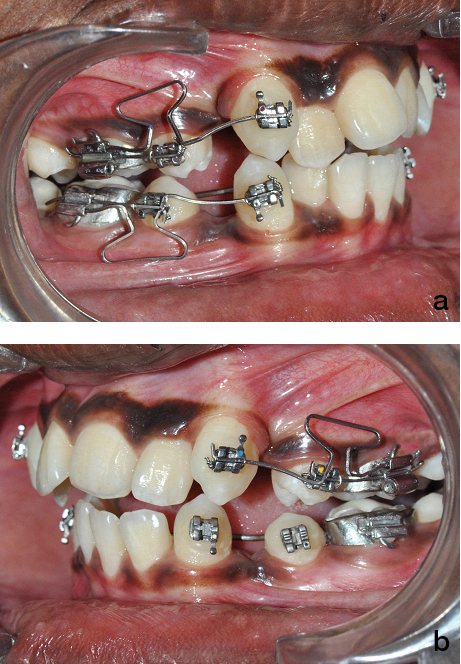
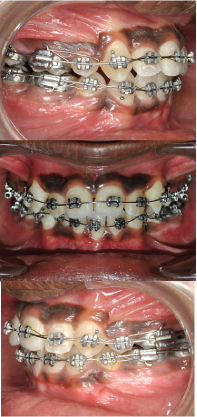
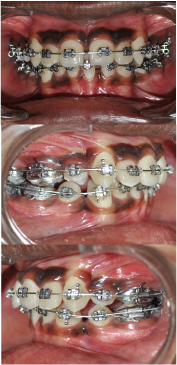
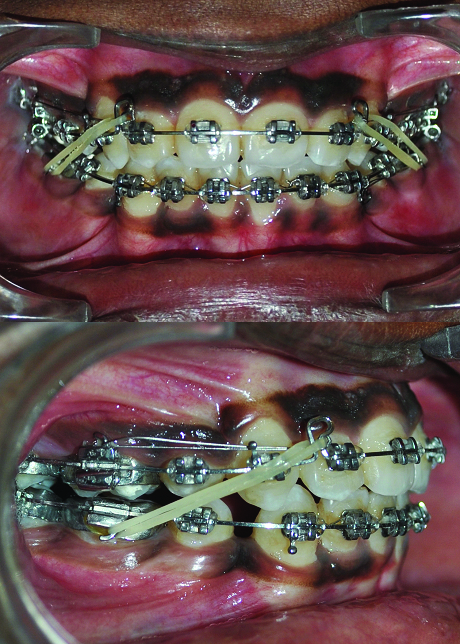
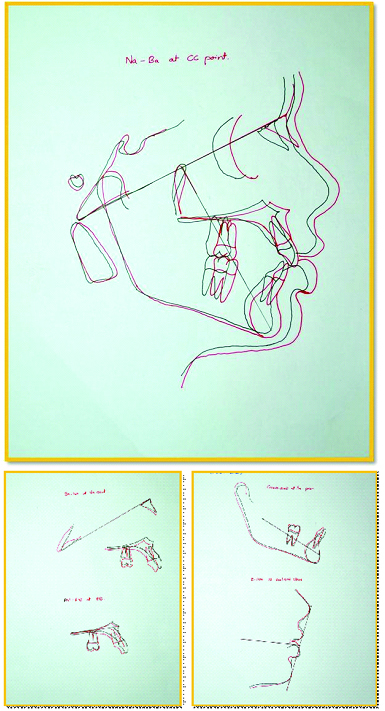
The case was treated using “Hybrid Segmental Mechanics” with extraction of all four 1st premolars with initial segmental retraction of maxillary canines and mandibular right canine using 0.017x0.025" TMA (Titanium, Molybdenum, Aluminum), ‘T-loop’ retraction spring [1,2] [Table/Fig-4a&b]. After segmented retraction of canine, leveling and alignment was carried out using continuous arch sliding mechanics using 0.016" Ni-Ti [Table/Fig-5a-c] and 0.019x0.025" Ni-Ti [Table/Fig-6a-c]. Residual Space closure was achieved using class II elastics [Table/Fig-7a&b]. In mandibular arch, right first molar was protracted to attain class I molar relationship. Finishing and detailing was carried out after closing all spaces. Most of the treatment objectives were met with the treatment, with good intraoral and facial results [Table/Fig-8a-c,9a-e,10a&b,11]. Pretreatment & post-treatment superimposition showed significant dento-alveolar change and good vertical control [Table/Fig-12a&b].
Canine Retraction with ‘T’ loop.
After initial segmental mechanics, continuous arch-wire sliding mechanics with 0.016" Ni-Ti in upper and lower arch.
Continuous arch-wire sliding mechanics with 0.019"x 0.025" Ni-Ti in upper and lower arch.
Residual space closure with continuous arch-wire sliding mechanics and class II elastics.
Post extra oral photograph.

Post intraoral photographs.

Post-treatment orthopantomogram & lateral cephalogram.
Comparison of pre-treatment and post-treatment cephalometric values.
| Skeletal | Average | PreTreatment | PostTreatment |
|---|
| SNA | (0) | 82 | 82 | 82 |
| SNB | (0) | 80 | 80 | 80 |
| ANB | (0) | 2 | 2 | 2 |
| N perp to pt A | (mm) | 0 + 2 | 0 | 0 |
| N perp to pog | (mm) | 0 to -4 | -1 | -2 |
| Go-Gn to SN | (0) | 32 | 24 | 28 |
| LAFH | (mm) | 65.6 + 4.9 | 63 | 65 |
| Eff. Max length | (mm) | 92.1 + 2.7 | 91 | 93 |
| Eff. Mand length | (mm) | 121.6 + 4.5 | 115 | 118 |
| DENTAL | | | |
| U1 to NA angle | (0) | 22 | 26 | 22 |
| U1 to NA (4) | (mm) | 4 | 7 | 4 |
| U1 to SN angle | (0) | 102 | 106 | 102 |
| L1 to NB angle | (0) | 25 | 25 | 26 |
| L1 to NB (4) | (mm) | 4 | 6 | 4 |
| L1 to A Pog mm | (mm) | 1-2 | 5 | 2 |
| IMPA | (0) | 90 | 100 | 95 |
| Interincisal angle | (0) | 130 | 123 | 128 |
| SOFT TISSUE | | | |
| S line to U lip | (mm) | -2 | 2.5 | 1.5 |
| S line to L lip | (mm) | 0 | 4 | 2 |
| Nasolabial angle | (0) | 90-110 | 104 | 100 |
Ricketts Superimpositions.
Discussion
Till date, continuous arch-wire sliding mechanic remains the most often used and most popular form of mechanics. The advantages of this approach may not apply to many complex dentally and periodontally compromised cases [3]. The most common alternative approach is segmented arch mechanic proposed by Charles Burstone et al., with its subsequent modifications [4,5]. However, it includes the complexity of appliance design and activation, difficulty in arch co-ordination, increased chair side time in appliance construction, decreased ability to delegate chair-side work to staff, patient discomfort from loops/spring and potential difficulty in maintaining oral hygiene [5]. Hybrid sectional mechanics described by Kapila and Conley attempts to combine simplicity and other advantages of continuous arch-wire mechanics with the precision and control of the segmented arch technique [6]. This approach uses traditional twin brackets, therefore offers the versatility to use continuous arch-wire mechanics, segmental mechanics, hybrid sectional mechanics or sequentially to use both mechanics as required by the case and the stage of treatment.
The underlying principle of hybrid segmental mechanics includes simplifying treatment by “segmenting” posterior and anterior region of the arch [7]. However, rather than employing true segments, a single continuous wire is placed in brackets from second molar up to canines but bypassing the incisors. The primary reason for this segmentation is that it eliminates the early engagement and round tripping of the incisors, potentially eliminating or minimizing its adverse consequences. This allows the retraction of the canine in earlier stage of treatment [8,9].
The sequence of mechanics and wires was as follows
Initial alignment was performed using 0.017x0.025 inch Ni-Ti wires in 0.022 slot, or smaller wires in a 0.018-inch slot.
In patients, whom the canine root has moderate or severe mesial inclination, a 0.017x 0.025-inch TMA T-loop segmented retraction spring should be used to distalize the root in adequate alignment and to relieve crowding to avoid the adverse consequences of correcting with a continuous arch-wire.
Alternatively canine retraction can be done by using the principle of segmented tooth movement but on a continuous arch-wire i.e. a bypass arch, as suggested by literature [5,9].
Residual space closure after leveling and alignment.
Finishing and detailing of the dentition.
Conclusion
Hybrid segmental mechanics strive to provide the simplicity, versatility and ease of use, similar to that of continuous archwire mechanics with the control of tooth movement associated with segmented mechanics to achieve goal oriented orthodontic treatment outcome. Selection of ideal mechanical approach for individual patient and dental arch is imperative for clinical success. Careful appliance design, well-considered practical selection of most advantageous biomechanics and execution of strategies to minimize adverse tooth movements are expected to produce the most desirable and efficient outcomes in subjects seeking orthodontic treatment.
[1]. Marcotte MR, Biomechanics in Orthodontics 1990 St. LouisMosby [Google Scholar]
[2]. Chander NS, Jena AK, A new method for sectional t-loop attachment for incisor retractionInt J Orthod Milwaukee 2015 26:11-13. [Google Scholar]
[3]. Hollender L, Ronnerman A, Thailander B, Root resorption, marginal bone support and clinical crown length in orthodontically treated patientsEur J Orthod 1980 2:197-205. [Google Scholar]
[4]. Burstone CJ, The segmented arch approach to space closureAm J Orthod 1982 82:361-78. [Google Scholar]
[5]. Mulligan TF, Common sense mechanicsJournal of clinical orthodontics: JCO 1980 14(5):336-42. [Google Scholar]
[6]. Kapila S, Conley RS, Optimizing biomechanics in complex and compromised cases, in Current Therapies in Orthodontics, ed. Nanda R, Kapila S 2010 St. LouisMosby:228-250. [Google Scholar]
[7]. El-Bialy T, Segmented and sectional orthodontic technique: Review and case reportJ Health Spec 2013 1:90-96. [Google Scholar]
[8]. Southard TE, Marshall SD, Grosland NM, Friction does not increase anchorage loadingAm J Orthod Dentofacial Orthop 2007 131:412-14. [Google Scholar]
[9]. Sharma M, Sharma V, Khanna B, Mini-screw implant or transpalatal arch-mediated anchorage reinforcement during canine retraction: a randomized clinical trialJ Orthod 2012 39(2):102-10. [Google Scholar]