Extrahepatic biliary atresia is a progressive disorder characterised by fibroinflammatory obliteration or stenosis of a segment or all of the extrahepatic biliary tree leading to obstruction of bile flow and cholestatic jaundice [1–3]. Extrahepatic biliary atresia is the most common cause for cholestasis in newborn [4] and accounts for 25-30% of the neonatal cholestasis cases [1]. The incidence varies from 1 in 5000 to 1 in 18,000 live births [1]. Classically infants present with jaundice and alcholic stools [1]. Clinically it presents as 2 forms - The perinatal form and the fetal or embryonic form [1]. The perinatal form accounts for majority of the cases [1,5,6] and its aetiology includes genetic, toxic, vascular and infectious causes [6]. The embryonic or fetal form accounts for 10-20% of the cases and is associated with congenital abnormalities [1,6]. Duct plate malformation is involved in its aetiopathogenesis [6]. The fetal group has very severe disease and worst outcomes even when surgical intervention is done in early course of disease [6]. Cholecintigraphy with HIDA (Hepatobiliary Imidoacetic Acid) shows lack of bile excretion and liver biopsy shows evidence of extrahepatic obstructive liver disease with extensive bile duct proliferation and biliary fibrosis [7]. The primary treatment of choice for extrahepatic biliary atresia is kasai’s portoenterostomy [8]. The overall 5-year and 10-year survival rates following kasai’s portoenterostomy are about 50 and 30% respectively [5]. However, before reaching adulthood, chronic liver disease develops in 67% of patients and many will ultimately need liver transplantation [9].
The purpose of this study was to analyse the significance of the various histopathological features in diagnosis and prognosis of extrahepatic biliary atresia from liver biopsy specimens.
Materials and Methods
This study included 43 cases of extrahepatic biliary atresia diagnosed and treated at a tertiary care hospital between January 2010 to December 2014. The diagnosis of extrahepatic biliary atresia was confirmed by histopathological examination of the liver biopsy specimen and intraoperative cholangiography taken during kasai’s portoenterostomy. Formalin fixed paraffin embedded tissues were processed by standard technique and the slides were stained with hematoxylin and eosin. All the histopathological slides were retrieved and re-evaluated for this study. The various histopathological features were graded by a semi-quantitative scoring system. The following histopathological features were evaluated in all the cases of extra-hepatic biliary atresia included in the study: (i) Lobular features such as cholestasis, hepatocyte giant cell transformation, extramedullary hematopoiesis; (ii) Portal tract features including portal fibrosis, bile ductular proliferation, portal and periportal inflammation and duct plate malformation.
All the cases were followed up for a period of 6 months which was done during the study period and were divided into three groups: (i) Alive (cases without any complications); (ii) Poor outcome (cases with recurrent episodes of jaundice, hospitilisation and developed secondary biliary cirrhosis); (iii) Died.
Statistical Analysis
Statistical analysis was worked out using SPSS 17.0 (statistical package for the social science software). Two sided Pearson chi-square test was used to find association between various parameters with respect to mortality. Kaplan-Meier estimator was used for survival analysis of the population under study. It is used to measure the fraction or number of subjects living for a certain period of time after an intervention.
The scoring system for grading the extent of fibrosis [3,10] includes:
Grade I (mild) fibrosis comprised cases with portal fibrous expansion to porto-portal bridging fibrosis involving less than 50% of portal tracts.
Grade II (moderate) fibrosis included cases with porto-portal bridging fibrosis involving greater than 50% of portal tracts without nodular hepatic architecture.
Grade III (severe) fibrosis ranged from porto-portal and porto-central bridging fibrosis involving greater than 50% of portal tracts associated with nodular hepatic architecture.
Bile duct proliferation refers to presence of greater than 5 bile ducts per portal tract and is graded according to a semi-quantitative scoring system [3,11].
Presence of 5 to 9 bile ducts per portal tract is graded as mild.
Greater than or equal to 10 bile ducts per portal tract is graded as moderate.
An average number of bile ducts per portal tract greater than or equal to 10 but the ducts are elongated attenuated and angulated is graded as severe bile duct proliferation.
Portal and periportal inflammation is graded as [6]:
Mild if cells are present in less than one third of portal tracts.
Moderate if cells are present in more than one third to two-thirds of portal tracts.
Severe when dense packing of cells present in more than two-thirds of portal tracts.
Cholestasis was graded as [6]:
Absent.
Mild (accumulation of bile in centrolobular hepatocytes).
Moderate (accumulation of bile in centrolobular and periportal hepatocytes or even in portal tracts).
Severe (shows presence of bile infarcts).
Duct plate malformation is identified by presence of numerous unusual curved and concentric bile ducts arranged around a fibrous or a central vascular core in the portal tract [6]. Histopathological examination of the biliary remnant will show fibroinflammatory obliteration of the duct, apoptotic degeneration of the residual bile duct epithelium and variable degrees of periductal inflammation [5].
Results
Of the total 43 cases in the study period, 28 (65%) and 15(35%) cases were male and female patients respectively. At the end of 6 months follow-up, 6 patients were alive without any complications, 17 had poor outcome and 20 cases died. All the parameters considered in this study were analysed in these patients and is summarised in [Table/Fig-1].
Various clinicopathological factors and its survival outcome.
| Clinicopathological factors | Number of patients (% of total) |
|---|
| Alive | Poor Outcome | Died |
|---|
| Mean age at kasai’s portoenterostomy (in days) | <30 | 0 | 0 | 2(4.7%) |
| 30-60 | 6(14%) | 16(37.2%) | 6(14%) |
| >60 | 0 | 1(2.3%) | 12(27.9%) |
| Degree of fibrosis | Grade I (Mild) | 5(11.6%) | 1(2.3%) | 0 |
| Grade II (Moderate) | 1(2.3%) | 8(18.6%) | 4(9.3%) |
| Grade III (Severe) | 0 | 8(18.6%) | 16(37.2%) |
| Degree of bile duct proliferation | Grade I (Mild) | 6(14%) | 3(7%) | 0 |
| Grade II (Moderate) | 0 | 9(20.9%) | 5(11.6%) |
| Grade III (Severe) | 0 | 5(11.6%) | 15(34.9%) |
| Degree of cholestasis. | Grade I (Mild) | 6(14%) | 5(11.6%) | 0 |
| Grade II (Moderate) | 0 | 12(27.9%) | 18(41.9%) |
| Grade III (Severe) | 0 | 0 | 2(4.7%) |
| Duct plate malformation | Negative | 6 | 15(34.9%) | 13(30.2%) |
| Positive | 0 | 2(4.7%) | 7(16.3%) |
The mean age at kasai’s portoenterostomy is divided in to 3 groups [Table/Fig-1]. The cases with age at surgery <30 and >60 days had grave prognosis. Among those operated between 30 and 60 days only 6 (14%) cases are doing well and the rest had poor outcome. Thus age at surgery did not prove to have effect on prognosis as cases who had been operated earlier (<60 days) also had poor outcome and was found to be statistically insignificant.
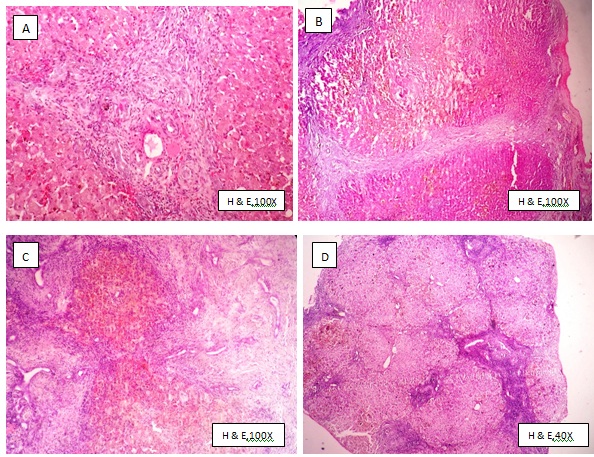
All the 43 cases had fibrosis and was graded as mild, moderate and severe [Table/Fig-1,2]. Of the patients alive, 5 out of the 6 cases had mild fibrosis and are doing well. Most of the patients with grade II fibrosis had poor survival with recurrent episodes of jaundice and developed secondary biliary cirrhosis. Among the patients with severe fibrosis none are alive indicating that the greater the degree of fibrosis, the poorer the survival and was found to be statistically significant (p= <0.001).
Degree of fibrosis: A- mild, B- moderate, C and D- Severe.
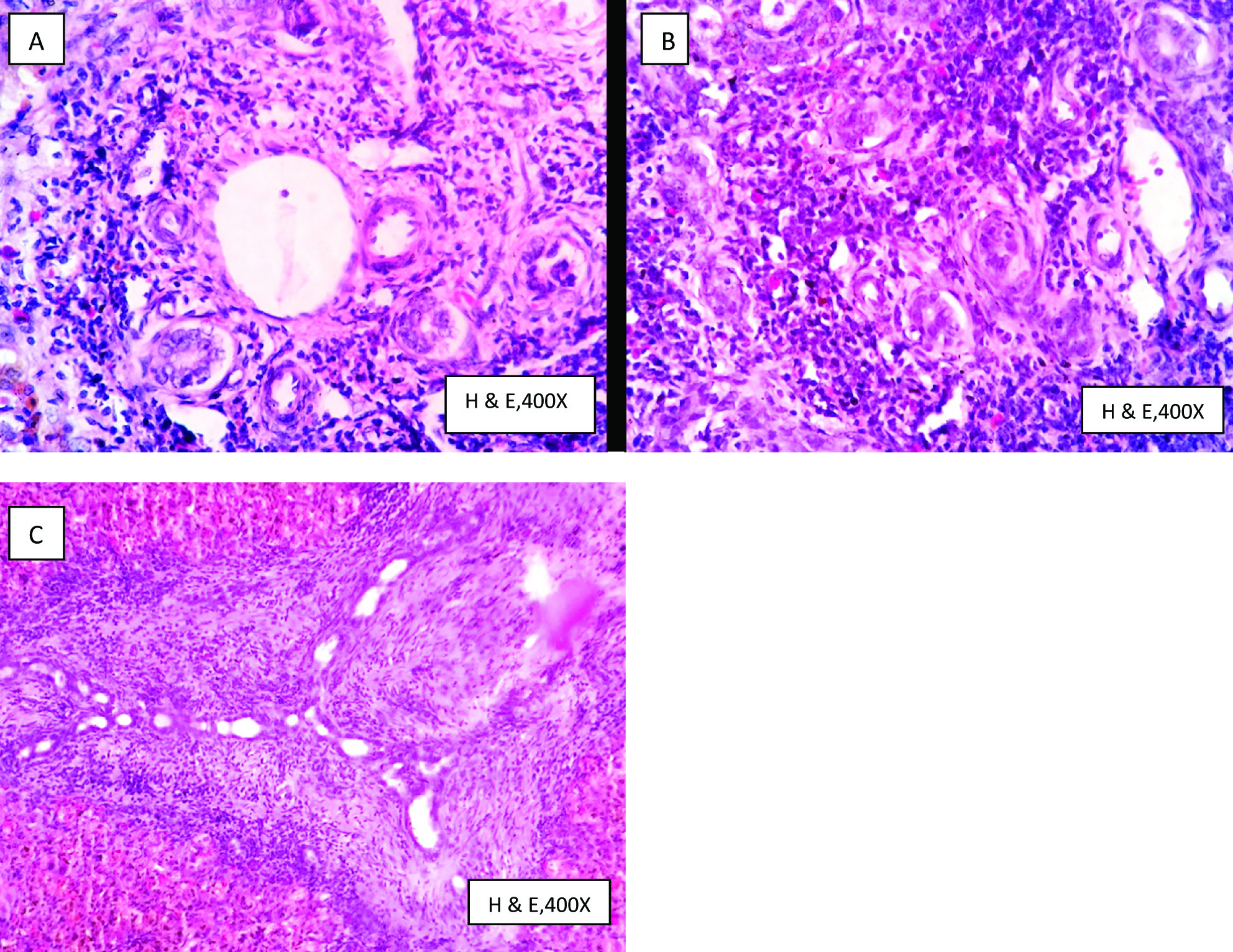
Bile duct proliferation was present in all the cases in this study and was graded as mild, moderate and severe [Table/Fig-1,3]. There was direct correlation between the severity of bile duct proliferation and the poor outcome and was proven to be statistically significant (p= < 0.001).
Degree of bile duct proliferation: A- Mild, B-Moderate and C-Severe.
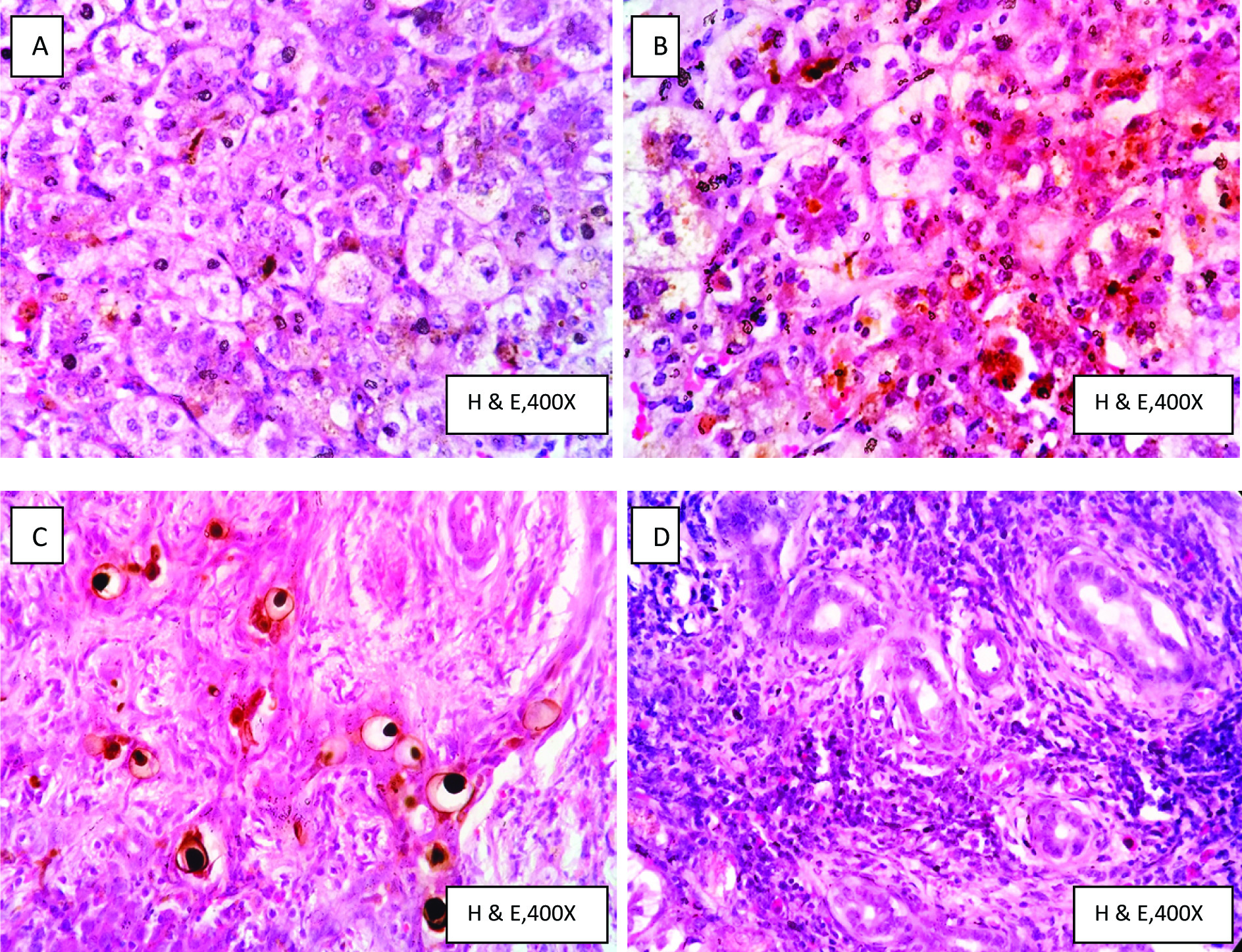
Cholestasis was present in all the 43 cases [Table/Fig-1,4] of which cases with grade II and III cholestasis had worst outcome and higher degrees of cholestasis were associated with greater degrees of fibrosis and bile duct proliferation and was proven to be statistically significant (p= < 0.001). Among the 43 cases, giant cell transformation of hepatocytes was seen in 6 (13.95%) cases. Portal and periportal inflammation with neutrophils and lymphocytes was found in all the patients included in the study. 10 (23.25%) cases had mild, 14 (32.56%) cases had moderate and 19 (44.18%) cases had severe portal and periportal inflammation. The extent of morbidity and mortality in this study was not altered by the severity of portal inflammation. Though portal inflammation was found in all 43 cases in variable degrees, it was found to be statistically insignificant [Table/Fig-4].
A and B-shows feathery degeneration of hepatocytes, intracanalicular and intrahepatocyte cholestasis; B- shows focal hepatocyte giant cell transformation. C-shows ductular cholestasis (bile plugs); D-shows dense portal inflammation with neutrophils, lymphocytes and few eosinophils.
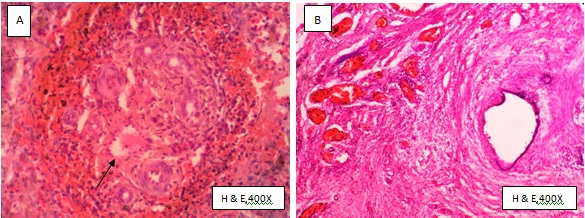
Duct plate malformation [Table/Fig-1,5] was seen in 9 cases of which 7 cases died in the early postoperative period irrespective of age at surgery and the other 2 cases had very poor survival indicating that the presence of duct plate malformation points to poor prognosis which was found to be statistically significant (p=0.0064). None of the 43 cases showed extramedullary haematopoesis.
A-shows duct plate malformation with numerous curvilinear and misshapen bile ducts peripherally arranged around a central vascular core (arrow). B-shows the biliary remnant with fibroinflammatory changes, apoptotic degeneration of the residual bile duct epithelium and variable degrees of periductal inflammation
Among the 43 cases, histological study of the biliary remnant could be done in 24 (55.82%) cases only. In rest of the cases the tissue obtained was flimsy or could not be excised properly for histopathological examination. Hence only those cases with good representative samples were studied and presented. Nevertheless the other cases had biliary atresia according to histological features of the liver biopsy specimen and intraoperative cholangiography. Among the 24 cases, 19 (44.8%) cases had variable degrees of fibrosis, periductal inflammation and a few showed apoptotic degenerative changes of the lining biliary epithelium [Table/Fig-5]. Only 5 among 24 cases showed complete fibroinflammatory obliteration of the biliary remnant.
The Kaplan-Meier survival curves for the 4 histopathological attributes which had a statistically significant effect on prognosis of cases is presented in [Table/Fig-6].
Kaplan meier survival curves relating the severity of various histopathological factors with survival. A- Degree of fibrosis, B- degree of bile duct proliferation, C- degree of cholestasis and D- duct plate malformation. In A,B,C the labelling 1,2 & 3 refers to the grading of fibrosis, bile duct proliferation and cholestasis respectively and shows that cases with grade 1 of all the above parameters had better survival. In D- ‘0’ refers to absence and ‘1’ refers to presence of duct plate malformation and shows that those cases with absence of duct plate malformation had better survival.
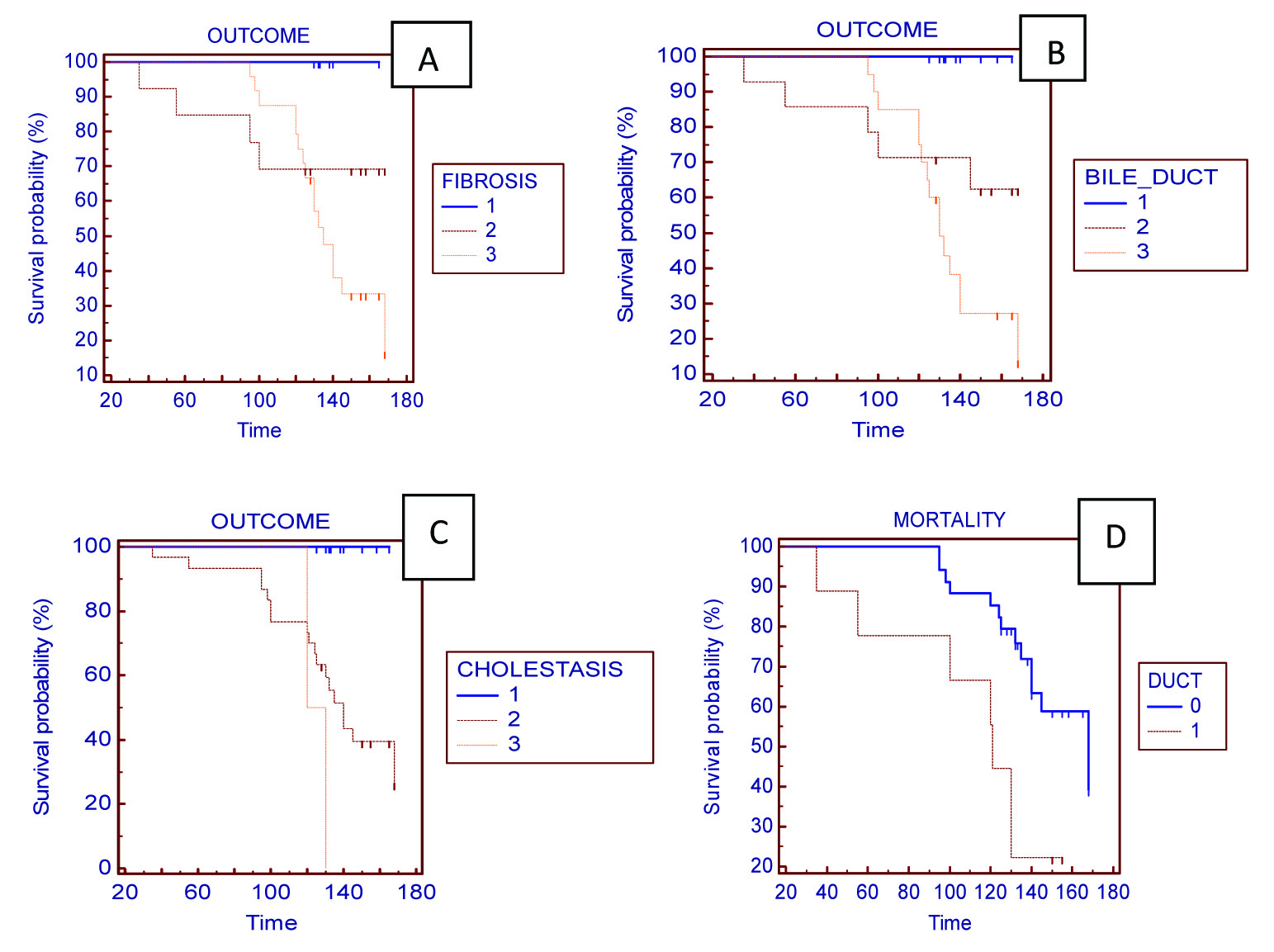
From the above data, it is observed that fibrosis, bile duct proliferation, cholestasis are the three important histopathological features to have a consistent association with extrahepatic biliary atresia and presence of duct plate malformation, greater degrees of fibrosis, bile duct proliferation and cholestasis were strongly associated with poor prognosis.
Discussion
Extrahepatic biliary atresia is the most common cause for cholestasis in newborn [4] and accounts for 25-30% of the neonatal cholestasis cases [1]. Various clinical features and laboratory tests like liver function tests, ultrasonography abdomen, HIDA scan and histopathological examination of liver can help us arrive at the correct diagnosis. In cases where the clinical, laboratory and radiological findings are inconclusive, histopathological study of the liver biopsy specimen is critical in making patient management decisions [12]. Histopathological findings of biliary atresia vary depending on whether the liver biopsy is taken during early or late course of the disease. Those cases in early stages of the disease show obstructive type of features such as lobular cholestasis, variable degrees of bile duct proliferation and portal odema. Other features like focal hepatocytic multinucleated giant cells may also be seen. Biopsy taken in late course of the disease shows less amount of ductular proliferation and many a times shows ductopenia [12]. The most consistent features of biliary atresia are the bile duct proliferation and portal fibrosis as said in various studies.
The overall accuracy of histopathological study of liver biopsy in diagnosing extrahepatic biliary atresia is 60-95%. Such variability is due to lack of strict histopathological diagnostic criteria for biliary atresia [9]. This study is undertaken to analyse the significance of the various histopathological features in diagnosis and prognosis of extrahepatic biliary atresia from liver biopsy specimens. Features such as increased age at kasai’s portoenterostomy, portal fibrosis, bile duct proliferation, cholestasis, portal inflammation and duct plate malformation were said to have effect on prognosis in various studies. All these parameters were analysed in this study group comprising of 43 patients.
In this study, an increased incidence of EHBA was observed in male patients which was in contrast to other studies that stated EHBA occurs more commonly in females when compared to male patients [13–15].
There are many studies highlighting the age at kasai’s portoenterostomy as a critical factor in determining the long term survival and also the extent of biliary fibrosis on initial biopsy [3]. Higher the age at surgery worser the prognosis as documented by most authors [16–19]. Sanghai et al., in their study concluded that surgery before three months of age has good outcome [20]. Hung et al., demonstrated poor outcome in infants operated after 120 days and noted a change in survival pattern based on the age at portoenterostomy [21]. Altman et al., have demonstrated no increased risk of failure between those operated before 49 days and the intermediate group operated between 50-70 days. But those patients operated by 71 days or more had significantly increased risk of failure when compared to the aforementioned groups [22]. Davenport et al., in their study have proven a reasonable medium-term survival in about one-third infants operated at 100 days or more [23]. In this present study, age at surgery did not show any correlation with prognosis as cases operated even at <60 days had poor survival.
Fibrosis is considered a progressive and an irreversible process and it impairs flow of bile leading to jaundice and worst outcome even after surgery [6]. According to the studies conducted by Arii et al., and Wildhaber BE et al., Biliary fibrosis at the time of surgery is an important prognostic factor in biliary atresia [24,25]. Bittmann et al., demonstrated the association between the presence of cirrhosis and poor prognosis and also it is an early indication for liver transplantation [26]. In this study we noted that high grade of fibrosis was uniformly associated with poor prognosis even when the cases presented early for surgery and did not have any other risk factors.
Bile duct proliferation is one of the most important histopathological feature in diagnosing EHBA [27] and shows a constant association with it except in very early stages of the disease [28]. There are only a very few studies on the prognostic importance of bile duct proliferation in EHBA. Some studies states that severe bile duct proliferation is associated with worst prognosis [29]. In this study we noted that lesser the degree of bile duct proliferation better the prognosis. The association between the degree of biliary proliferation and the survival rate of children with EHBA was also reported by Santos et al., [30]. This study also demonstrated a direct correlation between the extent of biliary fibrosis and bile duct proliferation and an increase in the degree of fibrosis also increased the bile duct proliferation proportionately.
Intrahepatic bile pigments (cholestasis) is said to be a consistent feature associated with biliary atresia [6,9] but not many studies speak on its prognostic significance. In the present study we found better survival in cases with lesser degree of cholestasis.
Absence of portal inflammation is said to be associated with poor prognosis according to Kahn et al., [2]. The present study did not show any correlation between portal inflammation and prognosis in biliary atresia. Hepatocyte giant cell transformation is seen in 20-50% of biliary atresia cases but is not as prominent as seen in neonatal hepatitis [1,4,31,32] and in our study it was present in 13.95% of cases and it did not have any diagnostic or prognostic significance.
Intrahepatic bile ducts develop from fetal duct plate by process of duct plate remodeling. Any disturbance in this orderly process gives rise to Duct Plate Malformation (DPM) as a result of which the ducts retain their fetal configuration. DPM has been associated with development of biliary atresia [3]. Awasthi et al., noted DPM in 51.29% of their cases [33] and various studies have demonstrated its incidence varying from 21-63% [34–36]. In this study we observed a mildly lower occurrence of DPM of about 30%. This might be because of lack of strict diagnosing criteria for differentiating DPM from biliary proliferation. All the cases with DPM in our study had very severe fibrosis with nodular transformation of liver and also had increased biliary proliferation. Most of cases with DPM had grave outcome pointing to the poor prognosis due to the presence of DPM.
Conclusion
From this study it can be concluded that in extrahepatic biliary atresia patients, presence of duct plate malformation, greater degrees of fibrosis, bile duct proliferation and cholestasis were strongly associated with poor prognosis.