Asplenia Syndrome in a Neonate: A Case Report
Kapil Bhalla1, Jasbir Singh2, Jaivinder Yadav3, Suchi Mehra4
1 Assistant Professor, Department of Pediatrics, PGIMS, Rohtak, Haryana, India.
2 Senior Resident, Department of Pediatrics, PGIMS, Rohtak, Haryana, India.
3 Assistant Professor, Department of Pediatrics, PGIMS, Rohtak, Haryana, India.
4 Junior Resident, Department of Microbiology, PGIMS, Rohtak, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jasbir Singh, Senior Resident, Department of Pediatrics, PGIMS, Rohtak, Haryana-124001, India.
E-mail: jasbir2001@gmail.com
Asplenia syndrome is a syndrome of right isomerism or attempted bilateral right sidedness. It includes congenital asplenia in association with complex congenital cyanotic heart disease and situs anomalies of the other thoracoabdominal organs. Herein we report a case of asplenia syndrome so as to highlight and refocus attention on the possibility of this rare syndrome that must be considered in a neonate presenting with congenital cyanotic heart disease.
Congenital heart disease, Heterotaxia, Situs ambiguous
Case Report
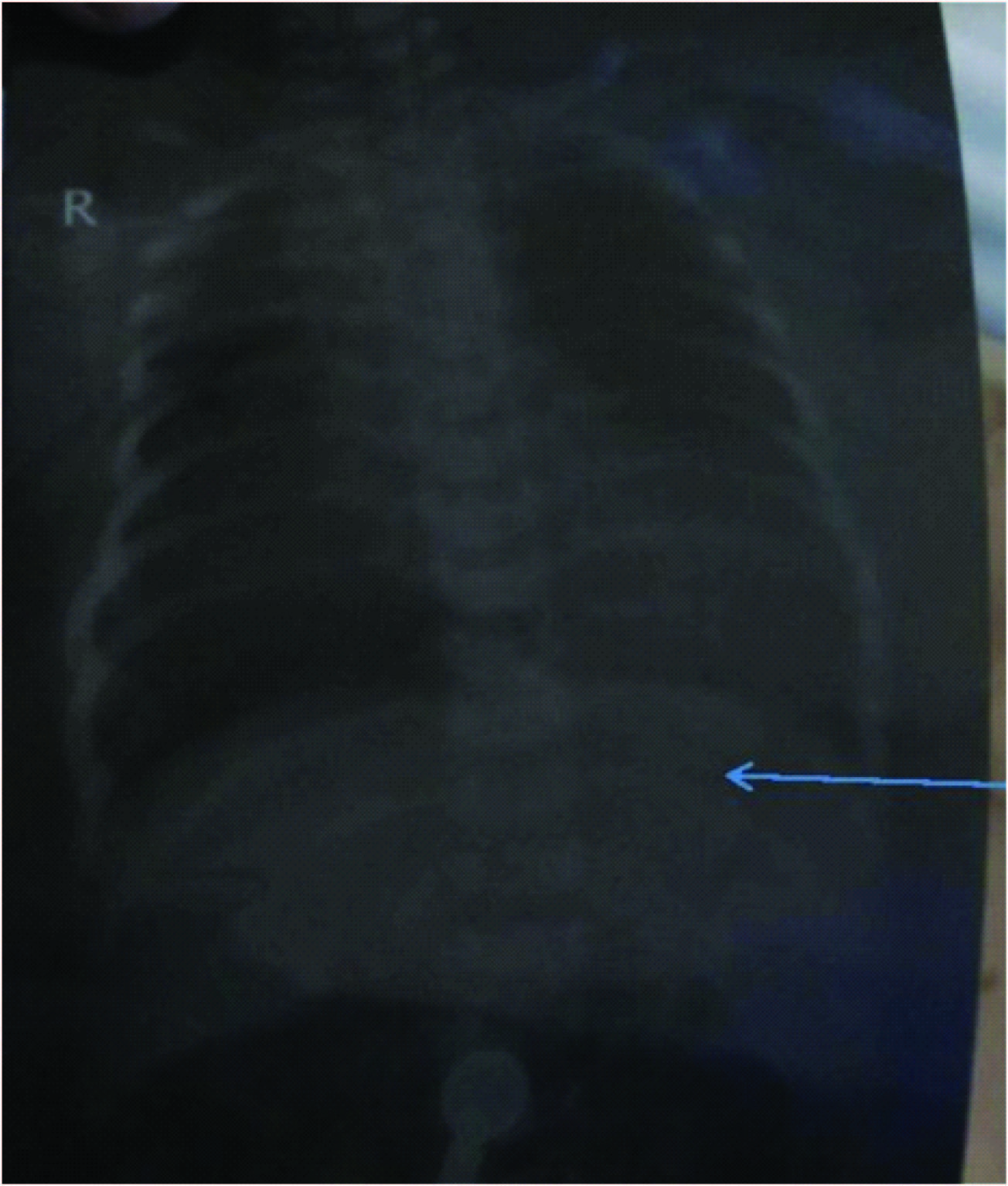
A 3195 gram male infant was a product of non-consanguineous marriage born to a 22-year-old primigravida mother at 40 weeks of gestation by caesarean section following failed induction at a private hospital. There was no history of drug intake or radiation exposure in any of the trimester. At birth, the baby was apparently well and handed over to mother for feeding. On day 2 of life, baby developed fast breathing and bluish discoloration of lips, refused feeding and was referred to pediatric emergency services of our hospital. At presentation there was central cyanosis, tachycardia (HR=168 per minute) and tachypnea (RR=72 per minute). The capillary refill time was more than 3 seconds and peripheral pulses were low volume. Pulse oximetry showed saturation of 32%. ABG showed pH 7.128, PaO2 42.2mmHg and PaCO2 40.8mmHg. Chest X-ray showed cardiomegaly (CT ratio 62%) and pulmonary oligemia. Prostaglandin E1 infusion was started. Shock improved after prostaglandin infusion with improvement in colour and saturation [Table/Fig-1]. Ultrasound abdomen revealed absent spleen and liver was in the midline predominantly on the left side [Table/Fig-2]. ECHO revealed mesocardia, complete atrioventricular septal defect, single ventricle, pulmonary arterial hypertension, large patent ductus arteriosus with left to right shunt.
X-ray shows liver on the left side (arrow) and no discernible spleen.
Ultrasound abdomen revealed absent spleen and liver was in the midline predominantly on the left side.

A diagnosis of asplenia syndrome was made. The poor prognosis of the child and risks of the surgical management if attempted were explained to the parents who refused further intervention. The baby died on day 6 of life. We cannot perform autopsy as parents did not gave consent for the same.
Discussion
Asplenia syndrome is associated with complex cardiopathy and situs anomalies of other thoraco abdominal organs [1]. The reported incidence is 1% of newborns with symptomatic congenital heart defects [2]. Although not pathognomonic, but many congenital heart diseases (CHDs) have been described in this condition. Most common associated CHDs are pulmonary stenosis, transposition of the great arteries and TAPVC [3]. In the index case there was mesocardia, complete atrioventricular septal defect, single ventricle and pulmonary artery hypertension. Heterotaxia, the discordant alignment of different organs is a characteristic feature. Apart from complete forms of laterality defects, such as the asplenia syndrome, partial situs inversus defects have been described which probably represent the other end of a spectrum of laterality defects [4]. Other associated conditions include intestinal malrotation, biliary atresia, splenic abnormalities and consequent immunologic derangements, faulty gastric suspension mechanisms, displacement of abdominal viscera, and aberrant vascular structures and vascular connections. In the index case there was absent spleen and transverse liver. Underlying basis for these abnormalities may be failure of laterality determining mechanisms during embryogenesis. The heart is most often affected, and it is the organ that most frequently leads to clinically detectable abnormalities as was seen in the index case. The major cause of mortality and morbidity in the asplenia syndrome is undoubtedly the cardiac malformations as in the index case.
Although most cases of heterotaxia/asplenia, are sporadic, many cases are familial, and some are X linked [5]. Thus, the abnormality is more common in males (60%) than in females. In the Index case there was no history of consanguinity and other sibling was normal, therefore the likely possibility that this was a sporadic case. In one family, an X-linked gene for heterotaxia has been mapped to Xq24-q27.1 [6]. These genes are now the target of positional cloning strategies, and their isolation is likely to accelerate our understanding of body axis determination. Once the diagnosis of asplenia is made, aggressive management should be done to have good outcome. Antibiotics prophylaxis and vaccination with pneumococcal polysaccharide, Haemophilus influenzae type b and meningococcal conjugate vaccine are the most important steps to prevent serious infections. Associated congenital anomalies mandates multidisciplinary approach and these anomalies are responsible for increased morbidity and mortality.
Conclusion
Asplenia syndrome has high incidence of associated congenital anomalies. We have to be very vigilant in newborn who presents with any congenital malformation and every newborn should be screened for involvement of other organs to have good outcome.
[1]. Devriendt K, Casaer A, Van Cauter A, de Zegher F, Dumoulin M, Gewillig M, Asplenia syndrome and isolated total anomalous pulmonary venous connection in siblingsEur J Pediatr 1994 153:712-14. [Google Scholar]
[2]. Rose V, Izukawa T, Moes CAF, Syndromes of asplenia and polysplenia. A review of cardiac and non-cardiac malformations in 60 cases with special reference to diagnosis and prognosisBr Heart J 1975 37:840-85. [Google Scholar]
[3]. Ho SY, Cook A, Anderson RH, Allan LD, Fagg N, Isomerism of the atrial appendages in the fetusPediatr Pathol 1991 11:589-608. [Google Scholar]
[4]. Ferdman B, States L, Gaynor JW, Abnormalities of intestinal rotation in patients with congenital heart disease and the heterotaxy syndromeCongenit Heart Dis 2007 2:12-18. [Google Scholar]
[5]. Ferrero GB, Gebbia M, Pilia G, A submicroscopic deletion in Xq26 associated with familial situs ambiguousAm J Hum Genet 1997 61:395-401. [Google Scholar]
[6]. Casey B, Devoto M, Jones KL, Ballabio A, Mapping a gene for familial situs abnormalities to human chromosome Xq24-q27.1Nat Genet 1993 5:403-07. [Google Scholar]