Oral health is an important aspect of general health and wellbeing of an individual which also affects the quality of life. Even though, oral diseases affect all the age groups, many reports suggest that due to multitude of factors, it is more common among children and elderly [1–5]. Dental caries is a major oral disease which affects children significantly. The reasons for the high incidence of dental caries among children are due to poor oral hygiene practices, frequent intake of diet containing sucrose, reduced salivary flow rate, lack of visit to a dentist and others [6].
Children also suffer from many chronic diseases, which make it necessary for long term medication that may have adverse effect on oral health [7]. Chronically ill children usually present with multiple risk factors which include poor oral health, high intake of sugar incorporated medicines along with improper dietary habits and poor social conditions [8]. Long term use of liquid medicines multiplies the risk of dental caries and dental erosion as well. Children are generally prescribed liquid medications or syrups which contain sucrose so as to make it acceptable and palatable for children [9]. Sugars (sucrose) have been used as a sweetening agent since 15th century. Along with sweetening properties, sucrose has been used as an antioxidant, demulcent, solvent and a bulking agent as sucrose is less expensive, non-hygroscopic and easy to process [10].
Epilepsy is a relatively common neurological disorder affecting 0.5-1% of the population in India. The causes and treatment protocols vary widely [11–13]. Dentists must be aware of its treatment side effects [13].
It was found that patients with epilepsy suffered with higher rate of dental caries due to multitude of factors and anti-epileptic drugs may act as an additional risk factor in the development of caries. It is also seen that if these patients are not on a regular follow up with the dentist then the number of decayed and missing teeth they have was higher than that of the general population. Decreasing the utilization of dental services has also found to decrease the number of restored and replaced teeth in epileptic patients. So it has become essential that dentists should know the exact side effects related to all Anti-Epileptic Drugs (AEDs), mainly those which are prescribed more often like the newer-generation AEDs [14].
Liquid Oral Medication (LOM) becomes an additional source of sugars for chronically ill children on long term care. Nearly 45% to 55% of all the liquid medications available are sugar – based [15]. Therefore, it becomes very essential that every health care professional who is involved with the prescription of medicine or drugs be aware of any consequential disorders that may arise as a side effect [16].
We designed the present study to test the hypothesis, formulated from clinical impressions that taking liquid medicine containing sucrose on a long term basis is a risk factor for dental caries. The evidence for association between sugar based LOM and dental caries in children suffering from epilepsy is still deficient, therefore high quality clinical studies need to be conducted.
The present study was carried out with the aim to assess and compare the dental caries experience and its relationship with long term usage of LOM with those not under such medication among 2-12 years old children with epilepsy.
Materials and Methods
The cross-sectional study was carried out from March 2012 to June 2012 at J.K. Loan Hospital, Jaipur, Rajasthan, India, which is a premier Government Pediatric Hospital of Rajasthan. The study participants included patients visiting the hospital and suffering from epilepsy. Before scheduling the present study, the required ethical clearance which was obtained from the research review board of Jaipur Dental College to conduct the study and permission was taken from the concerned hospital authorities. After taking the permission, detailed schedule was made and hospital authorities were informed in advance. A written informed consent was obtained from the parents of all children who were willing to participate in the survey. The research was conducted in full accordance with the World Medical Association Declaration of Helsinki.
Participants: Based on the findings of the pilot study, a total of 84 chronically ill children among 2-12 years under long term (for more than three months) LOM therapy were included as subjects of the study group (in patients) and in order to know the differences, a comparative group of 106 children, who were newly diagnosed cases of epilepsy were included as control group [children visiting Out-Patient Department (OPD)] for the first time.
Children aged 2-12 years, suffering from epilepsy, receiving LOM for more than three months and those children whose parents gave the consent were included in the study. Study subjects who were not on long term oral liquid medications or on any other form of medication, those children whose parents did not give the consent and study subjects with medical disorders requiring major modifications to the carbohydrate content of their diet, such as diabetes mellitus and obesity and patients suffering from any other systemic disease were excluded from both groups.
Training and calibration: The clinical examination for every subject was comprehensively carried out by single investigator. Prior to conducting the study, the investigator was calibrated at the Department of Public Health Dentistry, Jaipur Dental College, Jaipur, Rajasthan, India, in order to limit examiner variability and kappa value was found to be 0.82 which was satisfactory.
In order to assess the intra examiner reliability, the investigator applied DMFT/dmft/DMFS/dmfs/dft (Decayed, Missing, Filled Teeth/Surfaces) index on 30 selected subjects and recorded the findings. The same subjects were randomly examined on different days and the investigator repeated examinations on them. Intra examiner variability was 85%. These values reflected high degree of conformity in observation.
Pilot study and sample size calculation: Sample size was calculated at 80% study power, alpha error 0.05 and beta error 0.2 assuming prevalence of caries in non exposed/control/general population group of 35% and in exposed group of 60% as per the results of pilot study which was carried out on 30 children.
Sample size thus obtained was 70 subjects in each group which was further enhanced to 84 patients in each group considering 20% drop outs/attrition/non response/non cooperation.
General information: First part consisted of general information of children on long term liquid oral medication suffering from epilepsy regarding their name, age, gender, postal address, contact details, group to which they belong (study/control), education level of child’s father and mother.
Clinical examination: Second part consisted of clinical oral examination and the examination was purely clinical (mirror and probe); no radiographs were used in which dental caries in the permanent dentition was assessed by DMFT and DMFS given by Henry Klein, Carole E Palmer and Knutson JW in 1938 [17]. For assessing the dental caries in the deciduous dentition in less than five years, dmft and dmfs index and in mixed dentition dft and dfs index given by Gruebbel A.O. in 1944 was used [18]. Type III examination was conducted. The intra oral examination was carried out by the investigator under artificial white light in the inpatient and outpatient departments of the hospital under aseptic conditions. In some situations (during clinical examination) chemical method of disinfection was followed using cold solution [Korsolex (Glutaraldehyde-7.0gm; 1-6 dihydroxy 2.5 dioxyhexane-8.2gm and polymethyl urea derivative- 11.6gm) diluted by adding 1 part to 9 parts of portable water] for 15 minutes for disinfection of instruments (mouth mirror and explorer).
Statistical Analysis
The recorded data was analyzed in SPSS 17 version and tests of significance such as ‘t’ test and one way ANOVA were used. Descriptive statistics included computation of means and standard deviations. ODDs Ratio was calculated to provide an association with the dependent and independent variables. Differences were considered significant at p<0.05.
Results
In the total of 190 children with a mean age of 5.38 years, 45.2% were male. The frequency distribution of the participants in study and control group is shown in [Table/Fig-1].
Classification of participants in study group and control group.
| Study Group (children on long term liquid oral medications) | Control Group (not on long term liquid oral medicines) |
|---|
| Male N (%) | Female N (%) | Total N (%) | Male N (%) | Female N (%) | Total N (%) |
|---|
| Epilepsy | 41(48.8) | 43(51.2) | 84(100) | 45(42.4) | 61(57.5) | 106(100) |
Primary Outcomes
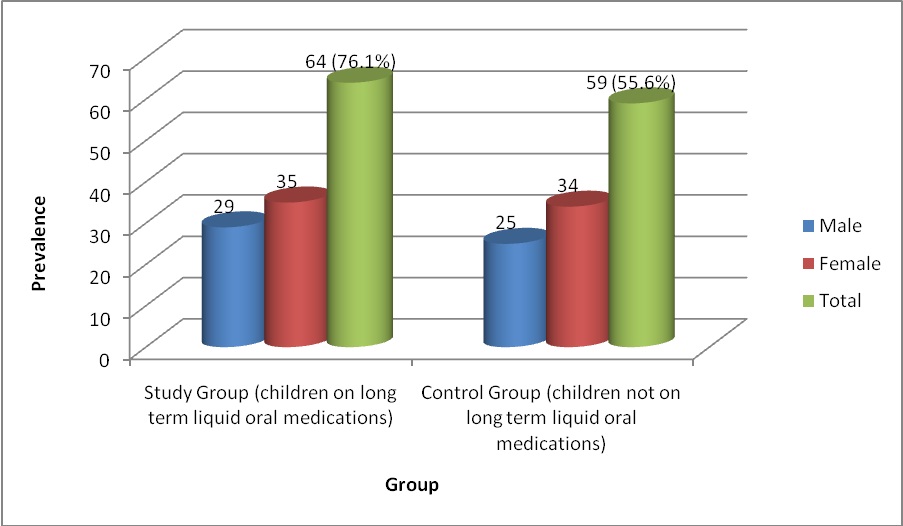
Dental caries was the outcome and was measured by DMFT/DMFS, dmft/dft and dmfs/dfs. Children who were on LOM were at the increased risk of dental caries than those who were not on medications (OR: 2.55) [Table/Fig-2]. [Table/Fig-3] shows the prevalence of dental caries in the study group (76.1%), was more when compared to control group (55.6%). The DMFT was found to be non-significant whereas the dmft/dft was highly significant between both groups [Table/Fig-4,5]. [Table/Fig-6,7] describes mean DMFS which was not significant in the study group (0.32±1.27) when compared to control group (0.23±1.34) (p=0.657, NS). The mean dmfs/dfs (6.86±7.83) in the study group was also higher when compared to control group (2.18±3.11) (p<0.001) [Table/Fig-7,8]. It was found that patient suffering with epilepsy were on Phenytoin on long term basis in study group.
The 2x2 contingency table describing the odds ratio.
| Group | Had dental caries | Didn’t have dental caries |
|---|
| Study Group (On LOM) | 64 | 20 |
| Control Group (not on LOM) | 59 | 47 |
| Odd’s ratio= ad/bc = (64×47) ÷ (59×20) = 2.55 |
Prevalence of dental caries based on diagnosis among two groups.
Mean Decayed, Missing and Filled teeth (DMFT) among study group and control group.
| Groups | Sex | N | Case Group (children on long term liquid oral medications) | Control Group (not on long term liquid oral medicines) |
|---|
| Diagnosis | Decayed (DT) | Missing (MT) | Filled (FT) | Total (DMFT) | N | Decayed (DT) | Missing (MT) | Filled (FT) | Total |
|---|
| Epilepsy | Male | 41 | 0.17±0.62 | 0.00±0.00 | 0.00±0.00a | 0.17±0.62 | 45 | 0.13±0.54 | 0.00±0.00 | 0.00±0.00a | 0.13±0.54 |
| Female | 43 | 0.18±0.69 | 0.00±0.00 | 0.00±0.00a | 0.18±0.69 | 61 | 0.11±0.48 | 0.03±0.25 | 0.00±0.00a | 0.16±0.71 |
| Significance† | | 84 | 0.702* | 0.375* | NA | 0.772* | 106 | 0.702* | 0.375* | NA | 0.772* |
Non significant*, †Two-tailed t-test was applied
NA- Not applicable, cannot be computed because standard deviation was zero.
a = t statistics cannot be computed because standard deviation of both groups are zero
Mean decayed, missing and filled teeth (dmft/dft) among two groups.
| Groups | Sex | N | Study Group (children on long term liquid oral medications) | Control Group (not on long term liquid oral medicines) |
|---|
| Diagnosis | Decayed (dt) | Missing (mt) | Filled (ft) | Total (dmft/dft) | N | Decayed (dt) | Missing (mt) | Filled (ft) | Total |
|---|
| Epilepsy | Male | 41 | 2.51±2.59 | 0.39±1.04 | 0.19±0.64 | 3.02±2.88 | 45 | 1.13±1.28 | 0.44±0.20 | 0.02±0.14 | 1.2±1.34 |
| Female | 43 | 3.25±3.29 | 0.27±0.76 | 0.23±0.64 | 3.76±3.40 | 61 | 1.18±1.46 | 0.13±0.464 | 0.04±0.28 | 1.34±1.51 |
| Significance† | | 84 | 0.000*** | 0.026* | 0.018* | .000*** | 106 | 0.000*** | 0.026* | 0.018* | 0.000*** |
*Non significant, ***Highly significant, †Two-tailed t-test was applied.
Mean Decayed, Missing and Filled Surfaces (DMFS) among two groups
| Groups | Sex | N | Study Group (children on long term liquid oral medications) | Control Group (not on long term liquid oral medicines) |
|---|
| Diagnosis | Decayed(DS) | Missing(MS) | Filled(FS) | Total(DMFS) | N | Decayed(DS) | Missing(MS) | Filled(FS) | Total(DMFS) |
|---|
| Epilepsy | Male | 41 | 0.26±1.00 | 0.00±0.00 | 0.00±0.00 | 0.26±1.00 | 45 | 0.13±0.54 | 0.00±0.00 | 0.00±0.00 | 0.13±0.54 |
| Female | 43 | 0.37±1.46 | 0.00±0.00 | 0.00±0.00 | 0.37±1.46 | 61 | 0.14±0.60 | 0.16±1.28 | 0.00±0.00 | 0.31±1.71 |
| Significance† | | 84 | 0.353* | 0.375* | NA | 0.657* | 106 | 0.353* | 0.375* | NA | 0.657* |
*Non significant, †Two-tailed t-test was applied
NA- Not applicable, cannot be computed because standard deviation was zero
Comparison of dental caries among children with epilepsy among two groups.
| Groups | N | Study Group (children on long term liquid oral medications) | Control Group (not on long term liquid oral medicines) |
|---|
| Diagnosis | DMFT(Mean+SD) | dmft/dft | DMFS | dmfs/dfs | N | DMFT(Mean+SD) | dmft/dft | DMFS | dmfs/dfs |
|---|
| Epilepsy | 84 | 0.17+0.66 | 3.40±3.16 | 0.32+1.27 | 6.86±7.83 | 106 | 0.15+0.64 | 1.28±1.43 | 0.23+1.34 | 2.18±3.11 |
| Significance† | | 0.772* | 0.000*** | 0.657* | .000*** | | 0.772* | 0.000*** | 0.657* | 0.000*** |
*Non significant, *** Highly significant, †Two-tailed t-test was applied
Mean decayed, missing and filled surfaces (dmfs/dfs) among two groups.
| Groups | Sex | N | Study Group (children on long term liquid oral medications) | Control Group (not on long term liquid oral medicines) |
|---|
| Diagnosis | decayed(ds) | missing(ms) | filled(fs) | Total(dmfs/dfs) | N | decayed(ds) | missing(ms) | filled(fs) | Total(dmfs/dfs) |
|---|
| Epilepsy | Male | 41 | 4.95±6.79 | 1.63±4.24 | 0.12±0.45 | 6.82±8.06 | 45 | 1.42±1.67 | 0.22±1.04 | 0.02±0.14 | 1.66±2.03 |
| Female | 43 | 5.39±6.06 | 1.32±3.79 | 0.23±0.64 | 6.9±7.71 | 61 | 1.88±2.73 | 0.65±2.32 | 0.03±0.25 | 2.57±3.68 |
| Significance† | | 84 | 0.000*** | 0.036** | 0.023** | .000*** | 106 | 0.000*** | 0.036** | 0.023** | 0.000*** |
**Significant, ***Highly significant, †Two-tailed t-test was applied.
Discussion
Dental caries may be considered a disease of modern civilization which is the result of complex interaction between bacterial enzyme, fermentable carbohydrates, host factors (teeth and saliva) and time. It can arise in early childhood as an aggressive tooth decay that affects the primary teeth of infants and toddlers up to the age of 71 months referred as Early Childhood Caries (ECC) [19].
Dental caries is the single most common chronic childhood disease which affects oral health related quality of life [20]. The study conducted by National Center for Health Statistics suggests that dental caries is more prevalent than many other systemic diseases including asthma, early childhood obesity and diabetes [19].
Similarly epilepsy affects 70 million people worldwide. It is considered a public health problem by the World Health Organization. India accounts for 10-20% (5-10 million) of the global burden of epilepsy. This is a challenge to health care services in India [11]. Dentists need to be familiar with the various manifestations of the disease, AEDs the patients are taking, and the complications and side effects of these drugs [13].
Prescription of sugar-free medication should be considered if there is a necessity for long term treatment (defined as daily or alternate days for more than three months) of epilepsy. Many of the children receiving long term medication are medically compromised and fall into high risk category for dental caries. Children suffering with epilepsy have multiple risk factors for occurrence of oral diseases such as poor oral hygiene practices, lack of visit to dentists, lack of preventive behavior, incorrect dietary habits, and others [21]. Along with these factors, the medication they take also has a profound effect on oral health.
The National Center for Health Statistics considers an illness chronic if its duration exceeds three months. Long term is defined as daily or alternate days for more than three months [21].
Liquid oral medicines, either prescription or over the counter, form a significant proportion (11%) of the medicines used by the population. The active agent present in these medicaments, can cause risk to oral health [22].
The findings of the present study provide fresh evidence regarding the association of LOM (phenytoin) with dental caries.
The prevalence of dental caries was higher in the study group when compared to control group. This may indicate that taking LOM for more than three months is a risk factor for dental caries. The highest contributor to the dmft/dft/dmfs/dfs index in both groups was missing teeth. This implied that the use of preventive services in the children was deprived. This may be due to the fact that the awareness of oral hygiene and judicious use of LOM for long term was very poor. Although parents normally recognize the importance of oral health for their quality of life, many will only visit a dentist in response to pain for their children due to lack of affordability or accessibility [23].
In permanent dentition the difference of dental caries experience was not significant between both groups but highly significant in primary dentition. This can be due to the fact that primary teeth are more prone to a rapid lesion progression from enamel to dentine and then to the development of pulpitis due to a lower thickness and a relatively larger pulp chamber in comparison to permanent teeth [24].
The findings of our study is in line with those of Sahgal J et al., (2002) [22], Roberts IF and Roberts GJ (1979) [25] and Maguire A et al., (1996) [26] who reported that experience of dental caries was higher in children under liquid oral medication when compared to healthier controls pointing a role of sugars present in the liquid oral medication.
Maguire A et al., reported higher dental caries experience with age-adjusted odd’s ratios 1.78 (95% CI: 0.55-2.97) compared to no caries experience in the primary dentition in chronically ill children [26].
Overall caries experience was recorded by Roberts and Roberts [25] with a mean defs of 5.55 for the children under LOM less than six years of age.
In the present study, children taking Phenytoin for treatment of epilepsy were 2.55 times more likely to suffer from dental caries than those without LOM which was highly significant.
Rajavaara P et al., demonstrated that the rate of dental restorations placed due to caries was constantly higher in girls with epilepsy than in their controls [27]. The observation supports the hypothesis that factors related to epilepsy, the antiepileptic medication in particular, might increase the risk of caries.
Studies done on various medicaments like analgesics, non-steroidal anti-inflammatory drugs, antibiotics, corticosteroids, anti-histamines, anti-tussives, multivitamins, bronchodilators, anti-emetics, anti-convulsants, anti-epileptics and anti-psychotics were found to show lower acidic pH (lower than the critical pH) needed for calcium dissolution [28–33]. Another report found a significant drop in plaque pH in medicines containing sucrose as compared to sucrose-free medicines [34]. Major concern of all health professionals should be to decrease the cariogenic and erosive potential of paediatric medicines. Adverse effects on oral health can be prevented if all the pediatricians prescribed sugar free syrups to their patients. Noting the adverse effects of sugar based LOM on dental health; many pediatricians prescribe sugar free medicines or opt for other forms such as tablets. The literature present few studies [Table/Fig-9] about association between various chronically ill children and LOM, but the present study specifically included the epileptic children [22,25,26]. Likewise, association between dental caries experience and congenital heart disease and asthma is being studied but the authors included medicine other then LOM like inhaled/oral steroids, bronchodilators etc., [35, 36]. Moreover few studies had found increased prevalence of dental caries in children suffering from epilepsy, sickle cell disease, and asthma but none of the authors had considered LOM as the research problem [37–40]. The data regarding association between LOM and dental caries experience in epileptic patient is still deficient.
Studies on association between dental caries experience and LOM
| Author (year) | Type of study | No. of patients | Findings |
|---|
| Roberts IF and Roberts GJ (1979) [25] | Cross sectional study. | 44- cases47- controls | Mean defs- 5.55 for the children under LOM less than 6 years of age. |
| Maguire A et al., (1996) [26] | Cross- sectional study | 186 ChildrenFour GroupsEpileptic patients- 15 | Children on LOM were 1.78 times more likely to suffer from dental caries than those not on LOM in primary dentition. |
| Sahgal J et al., (2002) [22] | Cross- sectional study | 51 on LOM54 not on LOM | Dental caries experience:Children on LOM> not on LOMPosterior teeth> anterior teeth. |
| Stecksén-Blicks C et al., (2004) [35] | Case-control study | 41- cases41- controls | Significant correlation between dmfs value and number of months on digoxin medication (only 10 children on digoxin syrup). |
| Vazquez EM et al., (2011) [36] | Cross- sectional study | 1160 children | Intake of nocturnal medication in asthmatic patients (OR = 2.41) was associated with dental cariesOther then syrups also included inhaled and oral steroids, bronchodilators or other medication. |
In a study carried out by Maguire A and Rugg-Gunn AJ, it was found that in Great Britain the percentage reduction in the use of liquid oral medicines among all medicines from year 1987 to 1992 was very small [41]. It is not always possible to avoid the use of liquid oral medications therefore the results of present study implicate that there is need for oral health promotion strategies that include brushing their teeth twice daily using toothpaste containing at least 500ppm fluoride, encouraging use of sugar-free chewing gum (particularly containing xylitol) and prescribing sugar free medicines to the patients [42]. It is also essential to deliver clear instructions regarding time of consumption of syrups and maintenance of good oral hygiene practices to ensure healthy dental habits throughout life.
Limitation
However, the results of the study cannot be extrapolated as the study was localized to one particular hospital. Further long term studies in different hospital settings can be conducted to find the association along with knowledge, attitude and practices regarding sugar based LOM among health practitioners.
Conclusion
Long term use of liquid medicines containing sucrose is a risk factor for dental caries among children with epilepsy. Therefore, the epileptic children requiring long-term liquid oral medication need targeted and comprehensive preventive care, if no suitable alternative to sugar-based medication is available.