A critical objective of root canal therapy of a tooth with apical periodontitis is to eliminate the microorganisms within the root canal system. The major cause for failure of root canal therapy is the incomplete removal of microorganisms from the apical third of the root [1]. Enterococcus faecalis (E. faecalis) is a persistent organism that, despite making up a small proportion of the flora in untreated canals, plays a major role in the root canal failure [2]. E. faecalis in root canals mainly exists as a biofilm by adhering to the root canal walls, accumulating and forming communities that are 1000 times more resistant to antimicrobials, antibodies and phagocytosis than isolated planktonic organisms [3]. Hence it is important to develop newer endodontic disinfection strategies that are more effective in eliminating bacteria within endodontic biofilm.
An important step involved in the control of endodontic infection is the use of various irrigating solutions in different concentrations during biomechanical instrumentation [4]. Sodium hypochlorite (NaOCl) is the most commonly employed root canal irrigant due to its potent antimicrobial action and effective tissue dissolution property. However, it has a cytotoxic effect when injected into the periapical tissues, a foul smell and taste [5]. Also, it has been reported that the high surface tension of NaOCl could affect its ability to penetrate into the dentinal tubules, thus reducing the antibacterial effectiveness [6].
Chlorhexidine gluconate (CHX) is a widely used antimicrobial agent with advantage of substantivity, has emerged as a potential irrigant and inter-appointment medication to be used during the endodontic treatment of teeth with apical periodontitis [7]. However, invitro studies suggest CHX is highly cytotoxic and caution should be exercised with the use of this antiseptic in the oral procedures. Moreover, it lacks tissue dissolving property during cleaning and shaping procedures [8]. Recognizing the potential toxicity of NaOCl and CHX with limited action on E. faecalis, an equally effective but safer irrigant is desirable [9]. Octenidine Dihydrochloride (OCT) (Octenisept, schulke and Mayr GmBH, Norderstedt, Germany) is a recently investigated solution and few studies have recommended it to be used as an alternative irrigant against E. faecalis infection [10–13].
With the conventional irrigation technique, the penetration of irrigant into the apical region is incomplete due to the small diameter of the canal and ramifications [14]. Hence, studies have suggested the use of Passive Ultrasonic Irrigation (PUI) to improve the action of various irrigants in effectively cleaning the complex anatomic areas in the canal [14,15].
To our knowledge and based on a literature search there are no in vitro studies to evaluate and compare the effect of agitation of OCT and CHX with and without PUI in root canals of human teeth infected with E. faecalis. Thus the aim of this invitro study was to evaluate antimicrobial effects of OCT versus CHX as root canal irrigant with and without PUI against E. faecalis.
Materials and Methods
The study was conducted at the Department of Conservative Dentistry and Endodontics, JSS Dental College and Hospital (JSS University), Mysore in association with Department of Microbiology, JSS Medical College and Hospital (JSS University), Mysore and was approved by the Institutional Ethical Committee for research on human subjects or specimens (JSS/PGS/Ethical/2013-14). The model proposed by Haapasalo and Orstavik, Berber et al., and Menezes et al., were used and modified for the present study [16–18]. Forty eight freshly extracted intact straight, single-rooted permanent human mandibular premolars with mature apices were collected and were disinfected in 5.25% sodium hypochlorite (NaOCl) (Nice Chemicals, Kochi, India). Calculus and tissue remnants were removed using ultrasonic scaler (Varios 750, NSK Nakanishi Inc., Tochigi, Japan). Only teeth with single root and canal were selected and teeth with curvature, pre-existing carious lesions, cracks, fracture, endodontic treatment, resorption, open apices or radiographically invisible or multiple canals were excluded from the study. The type I canal configuration was confirmed by digital radiograph (Oralix AC Gendex, Dentsply, Milano, Italy.) in mesiodistal and labiolingual planes. The teeth were decoronated with a diamond disc (NTI® Diamond Discs, Axis-Sybronendo, Kerr Corporation CA, USA.) and the specimens were standardized to 14mm length. Specimens were stored in 0.2% sodium azide solution until use.
The canals were initially instrumented 0.5mm beyond the apical foramen up to size 25 K-file [17]. Coronal part of the canal was prepared using Gates Glidden drills sizes #3 to #1 (Mani Inc, Tochigi, Japan.) and the apical size was standardized to 50 K-file (Mani Inc, Tochigi, Japan.) using manual technique with 1% NaOCl (Nice Chemicals, Kochi, India.) as irrigant. The internal diameter of the canal at the middle third was standardized to Gates Glidden drill #2 with a slow speed handpiece [19]. The canals were rinsed with 10ml of 17% EDTA (Canalarge, Ammdent, Chandigarh, India.) for 3min to remove smear layer and finally with 20ml of physiological saline solution (Nice Chemicals, Kochi, India.). The apex was sealed using light cure composite resin (Tetric N-Ceram, Ivoclar Vivadent AG, Liechtenstein.) and root surface was coated with nail varnish. The specimens were then allowed to dry at room temperature for one hour.
Each tooth specimen was placed in glass test tube containing 3ml of brain heart infusion broth (Himedia Laboratories, Mumbai, India.) and centrifuged to allow better penetration of broth in dentinal tubules [20]. The specimens were then autoclaved at 121°C for 15min under 15lbs pressure. To check the efficacy of sterilization the specimens were kept in an incubator at 37°C for 48 hours.
Cultivation of the E. faecalis and specimen contamination: Pure culture of E.faecalis (ATCC 29212) previously cultivated in BHI broth for 48 hours were obtained and then cultured on sheep blood agar + BHI agar plates in anaerobic conditions. The optical density of the bacterial suspension was adjusted spectrophotometrically to approximately 1.5 x 108 Colony Forming Units (CFU)/ml (concentration equivalent to 0.5 in the McFarland standard).
The glass test tubes containing the sterile specimen and broth were opened inside a laminar flow (Thermo Fisher Scientific Inc, Waltham, MA USA.) and automated micropipette (Himedia Laboratories, Mumbai, India.) was used to transfer 50μL of E. faecalis suspension into the tubes. The tubes were closed with sterile cotton ball. The infected specimens were incubated at 37oC for seven days and every second day the specimens were transferred to fresh tubes containing 3ml of broth contaminated with 50μL of E. faecalis [21]. Broth purity was checked by sub culturing 5μl on sheep blood agar. To confirm the penetration of microorganism into the dentinal tubules, two specimens from each group were submitted to the same initial instrumentation and contamination procedures followed by irrigation with sterile saline (control) and were then observed under Scanning Electron Microscopy (SEM).
Irrigation protocol: The irrigants tested were 0.1% OCT (Octenisept, Schulke and Mayr GmBH, Norderstedt, Germany.) and 2% CHX (RC-Chlor, Azure Lab, Kochi, India.) with and without PUI. The root specimens incubated for seven days were randomly divided into four groups containing 12 teeth each (n=12) according to the irrigation method:
Group I - Conventional syringe irrigation with 2% chlorhexidine (CSI/CHX).
Group II - Conventional syringe irrigation with 0.1% octenidine dihydrochloride (CSI/OCT).
Group III - Passive ultrasonic activation with 2% chlorhexidine (CHX+ PUI).
Group IV- Passive ultrasonic activation with 0.1% octenidine dihydrochloride (OCT+PUI).
In Group I and II, each root specimen was carefully removed from the broth and held with artery forceps and irrigated with 5mL of sterile saline to remove the broth. Then 4mL of irrigant (2%CHX or 0.1% OCT) was used for 2min with a side venting 27-gauge endodontic irrigation needle (Medic Disposable Needle, Warszawa, Poland.) keeping the tip of the needle 1mm short of working length using digital pressure, while the needle was moved back and forth without binding in the canal.
In Group III and IV, the irrigant 2% CHX solution (Group III) or 0.1% OCT (group IV) was filled in the canal using the side venting 27-gauge needle and ultrasonically activated for 2 minutes using an ultrasonic file of size 15 (2% taper) (Mani Inc, Tochigi, Japan) inserted to a depth 1 mm short of working length. The ultrasonic unit (Varios 750, NSK Nakanishi Inc., Tochigi, Japan.) was used in the “dry” mode and power setting on the ultrasonic unit was kept at one quarter of maximum. The passive ultrasonic irrigation was programmed for two 20sec cycles of activated irrigation during the two-min irrigation period as recommended in previous studies [20, 22]. Total of 4ml of irrigating solution was administered over 2min in these groups such that: 1.5ml of syringe irrigation was initiated for 30sec followed by 20sec PUI, the next 1ml syringe irrigation for 20sec, 20sec PUI, followed by 1.5ml of syringe irrigation for 30sec, totaling 2min of irrigation [20,22].
Microbial Analysis: Sterile saline solution was used to neutralize the irrigant in the canal and dried with paper points. Using diamond disc, horizontal notches were made at the junction of apical and middle third of the root and the apical segment was removed with pliers. Dentinal shavings were obtained at two depths (200μm and 400μm) by using sterile Gates Glidden drills #3 & #4 respectively in a circumferential technique in slow speed hand piece as per a previous study [19]. The dentin chips obtained were collected in a test tube containing 3ml of phosphate buffered saline. The suspension was homogenized by vigorous vortexing (Cyclo Mixer, Remi Laboratory Instruments, Mumbai, India.) for 5min. The dentin chips were allowed to sediment for 5min and the supernatant was used for microbiological analysis. A sterile loop was used to remove a 1μL of supernatant and inoculated on sheep blood agar plates using streaking method and incubated for 24 hours at 37°C. The numbers of CFU of E. faecalis were counted and readings were tabulated.
Scanning Electron Microscopy (SEM): For each group, two additional teeth were used for SEM evaluation to confirm the penetration of microorganism into the dentinal tubule and the effect of various irrigation protocols. Deep longitudinal grooves were made along the entire length of the buccal and lingual surfaces of the root without perforating the canal before inoculation. Immediately after the irrigation protocol the roots were split longitudinally using a sterile long handled end cutting plier. One half of each root was selected for examination under a scanning electron microscope (SEM) (EVO® LS15, Carl Zeiss Microscopy GmbH, Goettingen, Germany). The central beam of the SEM was directed to the surface of each root under 10X magnification in order to observe the whole sample surface. To observe the shape of bacteria and their characteristics, areas of interest were photographed at 3000x - 10000x magnification.
Surface tension and shear viscosity measurement: The Surface tension of the test irrigants was determined using a stalogometer method (method of counting drops). The measurements were repeated three times for each solution and average was calculated.
The viscosity for 2% CHX and 0.1% OCT was determined using MCR100 controlled stress rheometer (Paar Physica, Anton Paar, Gmbh, Germany.) equipped with co-axial cylinders (CC 27) and the radii ratio of co-axial cylinders was 1.08477. The rheometer was equipped with an electric temperature controlled peltier system (TEZ-15P-C) to control the experimental temperature and to maintain constant temperature, a circulating water bath was used (Viscotherm VT-2). The rheological parameter, shear stress (Pa) was measured by increasing the shear rate linearly up to a maximum of 750s-1 for duration of 10min. The data collected was analyzed using universal software US200. The measurements were repeated three times for each solution and average was calculated.
The viscosity values were obtained by experimental shear rate and shear stress data fitting with Newton equation:

Where, σ is shear stress (Pa), η is viscosity (Pa s), and γ is the shear rate (s-I)
Statistical Analysis
The data were statistically analyzed with one-way analysis of variance (ANOVA), followed by Scheffes multiple comparisons means to check the differences in CFU count between groups (p<0.05). The paired t-test was used to check for differences in CFU count for different irrigation protocol and at two depths (p<0.05). The analysis was performed with Statistical Package for the Social Sciences (SPSS 16.0, SPSS Inc, Chicago, IL, USA.).
Results
Group I-IV exerted antibacterial activity. [Table/Fig-1] shows the mean CFU count of E. faecalis at two depths (200μm and 400μm) for four irrigation protocols with the results of t-test. The number of CFU in all the experimental groups was significantly lower in comparison to control group (1880 CFU) with saline irrigation.
Mean (±SD) values of CFuml-1 of E.faecalis after tested irrigation solutions at 200μm and 400μm, with ANOVA and paired t-test comparison.
| Groups (n=12) | Mean CFU (±SD) | t | p-value |
|---|
| 200 μm | 400 μm |
|---|
| Group I (CHX) | 613.33 (33.41)a* | 516.92 (41.44)d | 6.275 | 0.000 |
| Group II (OCT) | 425.42 (51.85)b | 339.08 (52.18)e | 4.066 | 0.001 |
| Group III (CHX+ PUI) | 0.00 (.00)c | 195.67 (37.84)f | -17.912 | 0.00 |
| Group IV (OCT+ PUI) | 0.00 (.00)c | 238.58 (37.84)f | -20.110 | 0.00 |
| One-way ANOVA test for CFU between groups (200 and 400 μm depth). | F value | 430.197 |
| p-value | <0.001 (HS) |
| Multiple comparisons between the groups (Dependent Variable: CFU Scheffe) |
| (I) SUBLEVEL | (J) SUBLEVEL | Mean Difference (I-J) | Std. Error | Significance | 95% Confidence Interval |
| Lower Bound | Upper Bound |
| CHX 200 | CHX 400 | 96.4167(*) | 15.38761 | 0.000 | 37.2028 | 155.6306 |
| OCT 200 | 187.9167(*) | 15.38761 | 0.000 | 128.7028 | 247.1306 |
| OCT 400 | 274.2500(*) | 15.38761 | 0.000 | 215.0361 | 333.4639 |
| CHX+PUI 200 | 613.3333(*) | 15.38761 | 0.000 | 554.1194 | 672.5472 |
| CHX+PUI 400 | 417.6667(*) | 15.38761 | 0.000 | 358.4528 | 476.8806 |
| OCT+ PUI 200 | 613.3333(*) | 15.38761 | 0.000 | 554.1194 | 672.5472 |
| OCT+PUI 400 | 374.7500(*) | 15.38761 | 0.000 | 315.5361 | 433.9639 |
| CHX 400 | CHX 200 | -96.4167(*) | 15.38761 | 0.000 | -155.6306 | -37.2028 |
| OCT 200 | 91.5000(*) | 15.38761 | 0.000 | 32.2861 | 150.7139 |
| OCT 400 | 177.8333(*) | 15.38761 | 0.000 | 118.6194 | 237.0472 |
| CHX+PUI 200 | 516.9167(*) | 15.38761 | 0.000 | 457.7028 | 576.1306 |
| CHX+PUI 400 | 321.2500(*) | 15.38761 | 0.000 | 262.0361 | 380.4639 |
| OCT+ PUI 200 | 516.9167(*) | 15.38761 | 0.000 | 457.7028 | 576.1306 |
| OCT+PUI 400 | 278.3333(*) | 15.38761 | 0.000 | 219.1194 | 337.5472 |
| OCT 200 | CHX 200 | -187.9167(*) | 15.38761 | 0.000 | -247.1306 | -128.7028 |
| CHX 400 | -91.5000(*) | 15.38761 | 0.000 | -150.7139 | -32.2861 |
| OCT 400 | 86.3333(*) | 15.38761 | 0.000 | 27.1194 | 145.5472 |
| CHX+PUI 200 | 425.4167(*) | 15.38761 | 0.000 | 366.2028 | 484.6306 |
| CHX+PUI 400 | 229.7500(*) | 15.38761 | 0.000 | 170.5361 | 288.9639 |
| OCT+ PUI 200 | 425.4167(*) | 15.38761 | 0.000 | 366.2028 | 484.6306 |
| OCT+PUI 400 | 186.8333(*) | 15.38761 | 0.000 | 127.6194 | 246.0472 |
| OCT 400 | CHX 200 | -274.2500(*) | 15.38761 | 0.000 | -333.4639 | -215.0361 |
| CHX 400 | -177.8333(*) | 15.38761 | 0.000 | -237.0472 | -118.6194 |
| OCT 200 | -86.3333(*) | 15.38761 | 0.000 | -145.5472 | -27.1194 |
| CHX+PUI 200 | 339.0833(*) | 15.38761 | 0.000 | 279.8694 | 398.2972 |
| CHX+PUI 400 | 143.4167(*) | 15.38761 | 0.000 | 84.2028 | 202.6306 |
| OCT+ PUI 200 | 339.0833(*) | 15.38761 | 0.000 | 279.8694 | 398.2972 |
| OCT+PUI 400 | 100.5000(*) | 15.38761 | 0.000 | 41.2861 | 159.7139 |
| CHX+US 200 | CHX 200 | -613.3333(*) | 15.38761 | 0.000 | -672.5472 | -554.1194 |
| CHX 400 | -516.9167(*) | 15.38761 | 0.000 | -576.1306 | -457.7028 |
| OCT 200 | -425.4167(*) | 15.38761 | 0.000 | -484.6306 | -366.2028 |
| OCT 400 | -339.0833(*) | 15.38761 | 0.000 | -398.2972 | -279.8694 |
| CHX+PUI 400 | -195.6667(*) | 15.38761 | 0.000 | -254.8806 | -136.4528 |
| OCT+ PUI 200 | .0000 | 15.38761 | 1.000 | -59.2139 | 59.2139 |
| OCT+PUI 400 | -238.5833(*) | 15.38761 | 0.000 | -297.7972 | -179.3694 |
| CHX+US 400 | CHX 200 | -417.6667(*) | 15.38761 | 0.000 | -476.8806 | -358.4528 |
| CHX 400 | -321.2500(*) | 15.38761 | 0.000 | -380.4639 | -262.0361 |
| OCT 200 | -229.7500(*) | 15.38761 | 0.000 | -288.9639 | -170.5361 |
| OCT 400 | -143.4167(*) | 15.38761 | 0.000 | -202.6306 | -84.2028 |
| CHX+PUI 200 | 195.6667(*) | 15.38761 | 0.000 | 136.4528 | 254.8806 |
| OCT+ PUI 200 | 195.6667(*) | 15.38761 | 0.000 | 136.4528 | 254.8806 |
| OCT+PUI 400 | -42.9167 | 15.38761 | .363 | -102.1306 | 16.2972 |
| OCT+ US 200 | CHX 200 | -613.3333(*) | 15.38761 | 0.000 | -672.5472 | -554.1194 |
| CHX 400 | -516.9167(*) | 15.38761 | 0.000 | -576.1306 | -457.7028 |
| OCT 200 | -425.4167(*) | 15.38761 | 0.000 | -484.6306 | -366.2028 |
| OCT 400 | -339.0833(*) | 15.38761 | 0.000 | -398.2972 | -279.8694 |
| CHX+PUI 200 | .0000 | 15.38761 | 1.000 | -59.2139 | 59.2139 |
| CHX+PUI 400 | -195.6667(*) | 15.38761 | 0.000 | -254.8806 | -136.4528 |
| OCT+PUI 400 | -238.5833(*) | 15.38761 | 0.000 | -297.7972 | -179.3694 |
| OCT+US 400 | CHX 200 | -374.7500(*) | 15.38761 | 0.000 | -433.9639 | -315.5361 |
| CHX 400 | -278.3333(*) | 15.38761 | 0.000 | -337.5472 | -219.1194 |
| OCT 200 | -186.8333(*) | 15.38761 | 0.000 | -246.0472 | -127.6194 |
| OCT 400 | -100.5000(*) | 15.38761 | 0.000 | -159.7139 | -41.2861 |
| CHX+PUI 200 | 238.5833(*) | 15.38761 | 0.000 | 179.3694 | 297.7972 |
| CHX+PUI 400 | 42.9167 | 15.38761 | 0.363 | -16.2972 | 102.1306 |
| OCT+ PUI 200 | 238.5833(*) | 15.38761 | 0.000 | 179.3694 | 297.7972 |
*Scheffes Post Hoc test: Different letters (from a to f) indicate significant difference (p < 0.05) and groups with similar letters are not significant.
* Mean difference is significant at .05
Using one way ANOVA with multiple comparisons, statistically significant differences were found comparing Group I (CHX) and Group II (OCT) at 200μm and 400μm (p = 0.000) proving OCT to be better in reducing mean CFU count [Table/Fig-1]. Statistically significant differences were noted comparing Group I (CHX) and Group III (CHX+PUI) at 200μm and 400μm (p = 0.000). Similarly statistically significant differences were noted comparing Group II (OCT) and Group IV (OCT+PUI) at 200μm and 400μm (p= 0.000). CHX+PUI and OCT+PUI were most effective against E. faecalis at 200μm. No statistical significant difference were found between mean CFU count for CHX+PUI (Group III) and OCT+PUI (Group IV) (p=1.000) at 200μm; similarly no statistical significant difference were found between mean CFU count for CHX+PUI (Group III) and OCT+PUI (p=0.363) (Group IV) at 400μm.
However significant difference were found for CHX+PUI/OCT+PUI comparing the depths at 200μm and 400μm (p = 0.000) [Table/Fig-1]. Hence PUI was most effective at 200μm for both the irrigants.
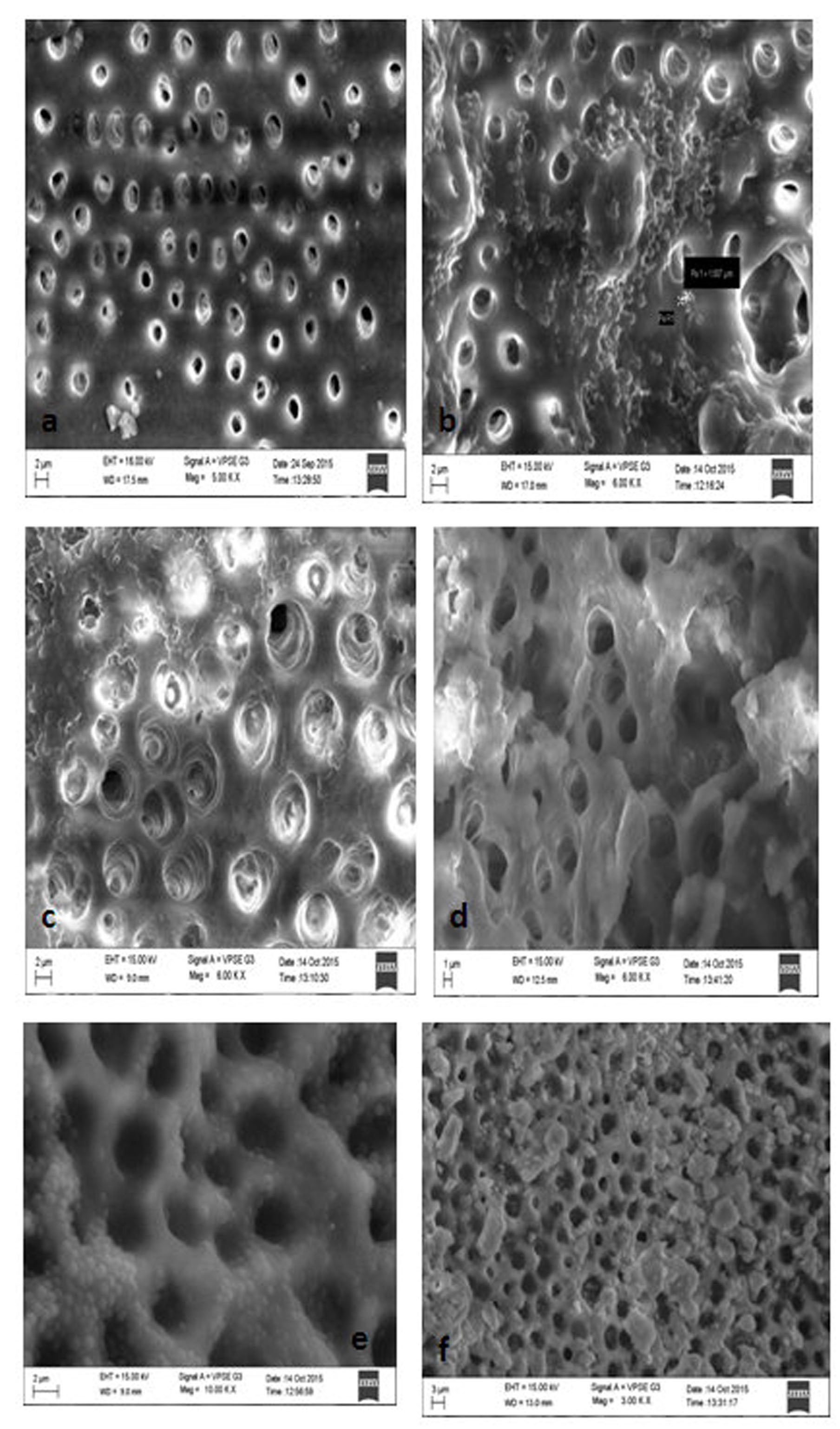
The SEM evaluation of root canal specimens showed invasion of the bacteria within the dentinal tubules. Infection of the root canal dentin was confirmed when harvested dentin shavings of control group yielded positive growth [Table/Fig-2]. The results of viscosity and surface tension measurements are presented in [Table/Fig-3].
Scanning electron microscopy (SEM) (a) dentin surface showing absence of smear layer and fully exposed dentin tubules (b) E. faecalis biofilm. Note the size of the E. faecalis (c) (Group I) after treatment with 2% CHX syringe irrigation (d) Group III- after treatment with 2% CHX syringe irrigation and PUI (e) Group II- after treatment with 0.1 % octenidine syringe irrigation (f) Group IV- after treatment with 0.1 % octenidine syringe irrigation with PUI.
Results of shear viscosity and surface tension.
| Irrigant | Shear viscosity (cP) | Surface tension (mN/m) |
|---|
| 2% Chlorhexidine | 1.5659 | 34.03 |
| 0.1% Octenidine | 1.2097 | 32.30 |
*cP – Centipoise, mN/m – millinewton/meter
Discussion
Endodontic irrigants are liquid antimicrobials used to disinfect microbial biofilms within the root canal. The process of delivery of endodontic irrigants within the root canal is called irrigation. The overall objectives of root canal irrigation are to inactivate bacterial biofilms, inactivate endotoxins, and dissolve tissue remnants and the smear layer (chemical effects) in the root canals, as well as to allow the flow of irrigant entirely through the root canal system, in order to dettach the biofilm structures and loosen and flush out the debris from the root canals (physical effects). While the chemical effectiveness will be influenced by the concentration of the antimicrobial and the duration of action, the physical effectiveness will depend upon the ability of irrigation to generate optimum streaming forces within the entire root canal system. The complex anatomy and chemical environment of the root canal prevents antimicrobial irrigating solutions and medicaments from exerting their full potential against all microorganisms found in endodontic infections [21]. Human mandibular premolars were selected because anatomy of the root canal may affect the result of microbial status within the root canal system.
The model in this study utilized a mono-species of E. faecalis for biofilm formation on the root canal walls of extracted teeth which provided a well-standardized anatomical model and allowed comparison of different irrigants in the intricacies of tubules with the inert buffering properties of dentin [22].
E. faecalis was chosen as the bacteriological marker in this study because of its clinical relevance, reported resistance to chemo-mechanical and intra-canal medication procedures; and for its prevalence in cases of endodontic failure [1,23]. There are many in vitro infection studies demonstrating E. faecalis to be capable of proliferating into dentinal tubules [4]. A seven day dentin contamination protocol as suggested by Haapasalo and Orstavik (modified) was used in the present study and the broth was changed on alternate days to prevent saturation of broth with E.faecalis and to replenish the nutrient source [21].
The depth of invasion of E. faecalis into the dentinal tubules is associated with nutritional conditions and the culture time during invitro studies [24]. Specimens infected for one day revealed penetration of bacteria up to 300μm-400μm depth in a few canals when studied in the light microscope and after three weeks of incubation with E. faecalis a moderate infection was usually seen up to 400μm-500μm [16]. The sampling procedure employed with Gates Glidden drill seemed quite sensitive and it was possible to take sample from inside the dentinal tubules at 200μm and 400μm from the canal lumen.
Various irrigants and medicaments like calcium hydroxide, 2% povidone-iodine [19], MTAD [6,25], chlorhexidine [29,25], tetraclean [6], green tea polyphenols and Triphala [26] have been tried for removal of E. faecalis biofilm, but have not been very efficient. Sodium hypochlorite is the most commonly used irrigant in root canal system. Regardless of the fulfillment of its desirable properties it has a certain drawbacks [5]. Chlorhexidine a broad spectrum synthetic cationic bis-guanide antimicrobial agent also shows a promising potential use as a root canal irrigant and medicament [4]. It has potent and substantive antimicrobial activity against E. faecalis and less cytotoxic in comparison to NaOCl [4]. Due to potential lack of dissolving necrotic tissue remnants, CHX cannot be advocated as the main irrigant in standard endodontic cases [8].
Recently a new irrigant Octenidine Dihydrochloride (Octenisept, Schulke and Mayr GmBH, Norderstedt, Germany.) a bispyridine derivative(N,N’-[1,10-decanediyldi-1(4H)-pyridinyl-4-ylidene] bis(1-octanamine) dihydrochloride), has been suggested as an alternative endodontic irrigant based on its antimicrobial effects and lower cytotoxicity [10]. Octenidine shows properties of positively charged (cation-active) chemical compounds, exhibits high antimicrobial efficacy and specific ability to adhere and form complexes with chemical components of cells and whole cells [27]. Tandjung et al., demonstrated efficacy of octenidine against E. faecalis in infected root canal dentin model [11].
In the present study significant difference were found comparing CHX (group I) and OCT (group II) at 200μm and 400μm (p = 0.000) indicating OCT to be better in reducing mean CFU count and the results are in agreement with a previous study [10].
Tirali et al., evaluated the effectiveness of NaOCl, CHX and OCT solutions at different time intervals against E. faecalis and C. albicans and concluded OCT being better with least CFU at 5min contact time [10]. In the present study the contact time of irrigant was 2 min and statistical significance was noted comparing OCT and CHX, with reduced CFU count with OCT both at 200μm and 400μm. Lucena et al., in an in vitro study on CHX and OCT based intra-canal medications found these to be better than calcium hydroxide [12]. Tirali et al., in an in vitro study compared the antimicrobial activity of NaOCl, CHX and OCT in different concentrations against E. faecalis, C. albicans and a mixture of both in agar diffusion test, and found OCT to have comparable antimicrobial activity to NaOCl [13]. In the same study it was observed that 2% CHX exhibited significant less antimicrobial effect compared to OCT. Tandjung et al., investigated the antimicrobial activity of Octenidine-phenoxyethanol gel against E. faecalis and found octenidine was particularly effective after incubation period of 10min and seven days. It was also found that Octenidine itself is the active agent and that the synergistic antimicrobial effect of phenoxyethanol is limited [11]. A study by Tirali et al., demonstrated octenidine to be more effective than NaOCl 5.25% in killing E. faecalis, S. aureus and C. albicans after different time intervals in a broth dilution test [10].
Based on tube dilution method the Minimal Inhibitory Concentration (MIC) values of Octenisept for E. faecalis, was found to be 0.002μg/ml [10]. However, another study in a preliminary experiment, found the MIC of Octenisept ranged between 0.0625 and 0.1875μg/mL [11]. Anuradha et al., evaluated the antimicrobial efficacy of OCT and NaOCl against E. faecalis by irrigating infected dentin blocks with 3ml of irrigant for 1min and found OCT to be more effective than 5% NaOCl [28]. Makkar et al., compared various concentrations of OCT and CHX against E. faecalis with different contact time found the number of CFU’s dropped to zero after 3min and remained zero after 5min and 10 minutes contact time, with 0.1% OCT and 2% CHX [29].
Bacteria can penetrate deeper into dentinal tubules to a variable range and that of E. faecalis was found to be upto 653μm by Parmar et al., [16,24]. Studies comparing syringe irrigation and Passive Ultrasonic Irrigation (PUI) conclude that PUI is more effective in removing remnants of pulp tissue, dentin debris and planktonic bacteria [3,30]. Hence, PUI was considered in this study.
An ultrasonic device converts electrical energy into ultrasonic waves of a certain frequency (30kHz) by magnetostriction or by piezoelectricity [31]. During PUI, there is occurrence of acoustic microstreaming and acoustic cavitation. The streaming pattern corresponds to the characteristic pattern of nodes and antinodes along the length of the oscillating file with maximum displacement amplitude at the tip. The shear flow caused by acoustic microstreaming produces shear stresses along the root canal wall, which can remove debris and bacteria from the wall [32]. Acoustic cavitation can be defined as the creation of new bubbles or the expansion, contraction and/or distortion of pre-existing bubbles in a liquid, the process being coupled to acoustic energy [31]. According to Roy et al., two types of cavitation could occur during PUI of root canals: (i) stable cavitation and (ii) transient cavitation. Stable cavitation is linear pulsation of gas filled bodies in a low amplitude ultrasound field, and transient cavitation occurs when vapour bubbles undergo highly energetic pulsations [33].
The application of PUI creates shear forces that can cause physical disruption of bacterial aggregations (biofilm) [15]. In the present study, mechanical agitation was effective in enhancing the efficacy of both the test irrigants, thereby influencing bacterial viability in the biofilms. Studies report different outcomes regarding the antimicrobial efficacy of PUI. Ferreira et al., found CHX to be less effective than NaOCl in removal of debris, when applied ultrasonically in a continuous way [34].
In our knowledge there are no studies comparing the effectiveness of OCT when agitated with PUI. The PUI groups with irrigant had better disinfection action compared to syringe irrigation only and this was statistically significant.
In addition to mechanical agitation, the effectiveness of killing biofilm bacteria is dependent on the chemistry of the antibacterial agent and the contact time. The differences in the physical properties of the materials affect the transmission of ultrasonic energy by the irrigant [35]. The probable reason for the enhanced antimicrobial effect of octenidine can be attributed to its cation-active structure that tends to bind readily to the negatively charged bacterial cell envelope, automatically disrupting the vital functions of the cell membrane and killing the cell. Preliminary results point to a strong adherence particularly to lipid components (e.g., cardiolipin) prominent in bacterial cell membranes explaining the high antimicrobial efficacy without adversely affecting human epithelia or wound tissue [36]. Octenidine has been demonstrated to be more effective than chlorhexidine as a means for prolonged bacterial anti-adhesive activity [37]. It also proved to resists organic challenges by maintaining its antimicrobial property in the presence of organic material when compared to chlorhexidine and iodine [27].
Other factors which could have a role in better penetration and antimicrobial action of OCT compared to CHX can be correlated to two important parameters: (i) surface tension and (ii) viscosity which help to understand fluid dynamics in root canals.
The surface tension is defined as ‘the force between molecules that produces a tendency for the surface area of a liquid to decrease’. This wettability (surface tension) of the solution governs the capability of its penetration both into the main and lateral canals, and into the dentinal tubules [6]. High surface tension could affect the ability of irrigant to penetrate into dentin and thus reduce its antibacterial effectiveness within dentinal tubules and previous studies have showed an increase in penetration of the irrigant (NaOCl) with a decrease in viscosity and surface tension [6,38].
Dynamic viscosity is an essential parameters related to fluid flow which is the resistance exhibited by a fluid while it is being deformed by tensile or shear stresses. The lesser the viscosity, the easier is the fluid movement [39]. Two types of flow patterns exists in fluid dynamics, namely, (i) laminar flow, characterized by smooth and constant fluid motion and (ii) turbulent flow which has chaotic eddies, vortices and other flow instabilities [39,40]. The turbulent flow may improve root canal cleaning efficiency by breaking the biofilm and debris, like the cavitation phenomenon reported with the use of ultrasonics. In practice, factors such as dentin irregularities, canal ramifications and agitation technique may also contribute to turbulent flow [40].
Previous studies have shown an increase in penetration of the irrigant with a decrease in viscosity and surface tension [6]. In the present study, the shear viscosity and surface tension of OCT was less compared to CHX and hence better flow characteristics in the canal.
Limitation
The limitation of this study include (i) it was an invitro study and accurate replication of clinical conditions are not achieved, (ii) it was not possible to assess the presence of bacteria from areas other than the main canal and (iii) Rheometer was used to measure the shear viscosity, in contrast to viscometer to measure the dynamic viscosity which is more specific in irrigation dynamics.
The present study found the efficacy of Octenidine in biological complex environment to be adequate and indicates the justification for further comparative studies, including common antimicrobial agents used in endodontics.
Conclusion
Under the limitation of the present study,
With conventional syringe irrigation, 0.1% OCT was more effective than 2% CHX against E.faecalis both at 200μm and 400μm.
Passive ultrasonic irrigation of both test solutions (2% CHX and 0.1% OCT) showed complete reduction of bacterial colonies at 200μm and significant reduction of bacteria at 400μm, showing its superiority over conventional syringe irrigation.
*Scheffes Post Hoc test: Different letters (from a to f) indicate significant difference (p < 0.05) and groups with similar letters are not significant.
* Mean difference is significant at .05
*cP – Centipoise, mN/m – millinewton/meter