Aneurysmal Bone Cyst: An Uncommon Secondary Event in Calcaneal Chondroblastoma
Sandip Barman1, Preeti Diwaker2, Divya Bansal3, Neelam Wadhwa4, Gurvinder Singh5
1 Junior Resident, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
2 Assistant Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
3 Senior Resident, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
4 Associate Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
5 Senior Resident, Department of Orthopaedics, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Preeti Diwaker, Assistant Professor, Department of Pathology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi-110095, India.
E-mail: diwaker_preeti@yahoo.co.in
Chondroblastoma is an uncommon benign bone tumour, involvement of epiphysis of long bones is typical. Chondroblastoma of the calcaneum is uncommon and its association with secondary aneurysmal bone cyst is even rarer. Only two cases of calcaneal chondroblastoma associated with secondary aneurysmal bone cyst have been reported till date.
A 22-year-old male presented to the department of orthopaedics with complains of pain and swelling in the left heel since the last 10 months. On clinico-radiological grounds differentials considered were giant cell tumour of bone and aneurysmal bone cyst. In view of the histopathological findings of bone curettage and results of special stain and immunohistochemical marker, final diagnosis of chondroblastoma with secondary aneurysmal bone cyst, left calcaneum was rendered.
Although rare, chondroblastoma should always be considered in osteolytic lesions of calcaneum. The identification of secondary aneurysmal bone cyst component is important as it has higher chances of recurrence than usual chondroblastoma.
Aneurysmal, Bone cysts, Chondroblastoma, Calcaneum
Case Report
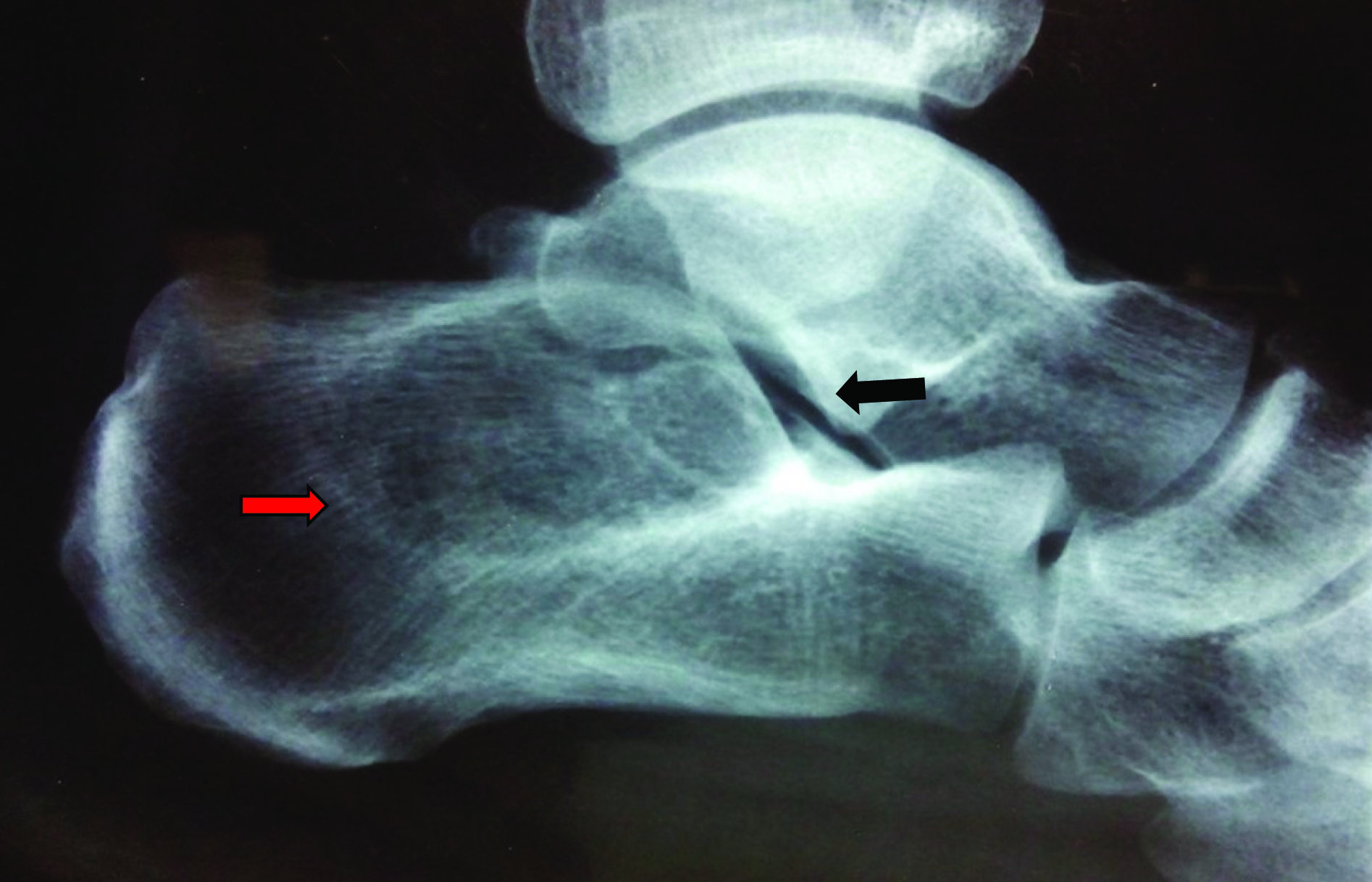
A 22-year-old male presented to the Department of Orthopaedics with complain of pain and swelling in the left heel since last 10 months. The pain was insidious in onset, dull aching which got aggravated on walking or standing and was relieved on rest. The swelling was gradually increasing in size. Clinical examination showed an ill-defined swelling present on medial aspect of left calcaneum. It was firm in consistency, non-pulsatile, non-compressible and tender on deep palpation. Sub-talar joint movement was painful with restriction in inversion of left foot. Left calf muscle wasting was also present and he had an antalgic gait. Lateral radiograph of the left ankle and foot showed an eccentric osteolytic lesion with sclerotic margin in the calcaneum extending upto the subtalar joint [Table/Fig-1]. MRI showed an expansile lesion with irregular borders and cystic areas with multiple fluid levels [Table/Fig-2]. The differentials of lytic lesion in calcaneum include intraosseous lipoma, Simple Bone Cyst (SBC), aneurysmal bone cyst, giant cell tumour, osteosarcoma, Ewing’s sarcoma, metastasis and chondroblastoma [1]. On clinico-radiological correlation, Giant Cell Tumour of bone (GCT) and Aneurysmal Bone Cyst (ABC) were considered. The radiological findings matched with ABC as there was well defined osteolytic lesion with sclerotic margins and multiple fluid levels were identified. GCT was considered in view of the eccentric well defined lytic lesion abutting the subtalar joint. The sclerotic margins although are not a feature of GCT but may be seen uncommonly in cases of GCT [2]. MRI findings could also be explained on the basis of secondary ABC component. Intraosseous lipoma is the most frequent calcaneal bone lesion, however not considered in view of the absence of fat content and presence of multiple fluid levels on MRI. Per-operatively the lesion resembled ABC. Bone curettage and bone grafting with G-bone synthetic bone graft [Table/Fig-3] and iliac crest autologous bone grafting [Table/Fig-4] was done. The bone curettage specimen comprised of multiple soft tissue pieces together measuring 4x2x1cm. The haematoxylin and eosin stained sections revealed highly cellular tumour with interspersed giant cells and few areas of amorphous pink chondroid [Table/Fig-5]. Tumour cells were round to polygonal with pink granular cytoplasm, single nuclei which showed indentation and grooving [Table/Fig-6]. These findings were highly suggestive of chondroblastoma. A separate area within the tumour showed cyst like spaces filled with hemorrhagic material. These spaces were lined by thin fibrocellular septae with few giant cells. This area was histopathologically suggestive of aneurysmal bone cyst [Table/Fig-7]. Chicken wire calcification, necrosis and atypical mitosis were not seen in any of the sections examined. In view of the clinic-radiological differentials and two types of tumour morphology seen on histopathological examination, reticulin stain and S-100 were performed to confirm the diagnosis of chondroblastoma. Reticulin stain showed characteristic honeycomb pattern [Table/Fig-8] and the tumour cells displayed diffuse cytoplasmic positivity with S-100 [Table/Fig-9]. Thus a final diagnosis of chondroblastoma with secondary ABC, left calcaneum was rendered. The patient was followed up for 8 months and there were no signs and symptoms of recurrence till date. Unfortunately, the patient could not furnish his post-op radiograph as he had supposedly lost it.
Lateral radiograph of the left ankle and foot shows an eccentric osteolytic lesion with sclerotic margin in the calcaneum (red arrow) extending upto the subtalar joint (black arrow).
MRI shows an expansile lesion with irregular borders (arrow) and cystic areas (arrow heads) with multiple fluid levels.

Bone curettage and bone grafting with G-bone synthetic bone graft.
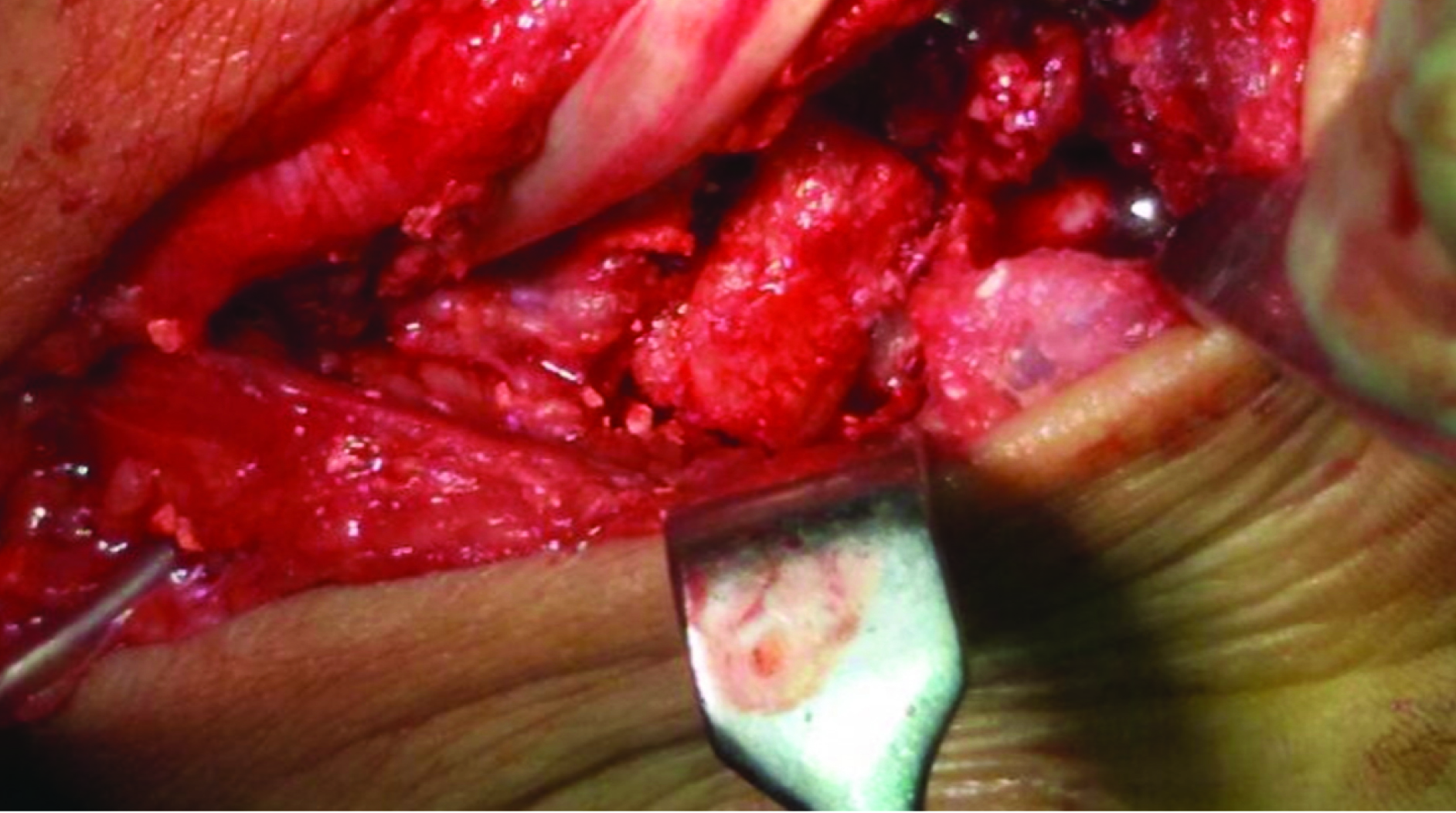
Iliac crest autologous bone grafting.

Sections show highly cellular tumour with interspersed giant cells (arrows) and few areas of amorphous pink chondroid (arrow-head). (H&E; 100X).
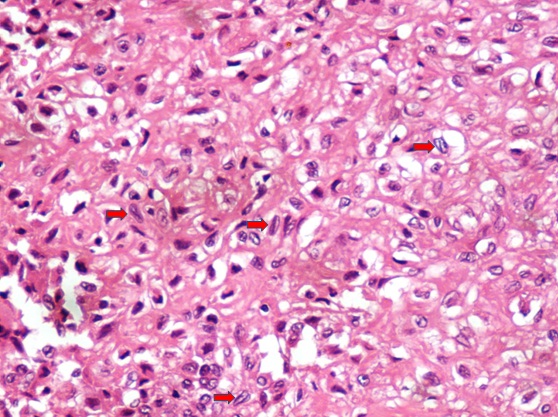
Tumour cells are round to polygonal with pink granular cytoplasm, single nuclei which show indentation and grooving (arrow) (H&E; 400 X).
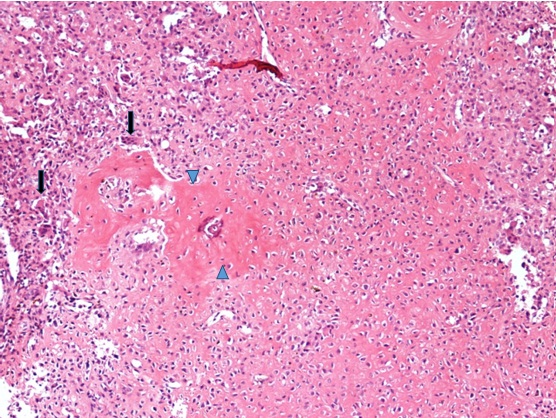
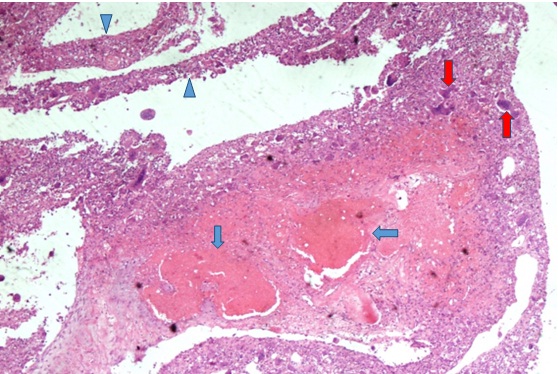
Cyst like spaces filled with hemorrhagic material (blue arrows). These spaces were lined by thin fibrocellular septae (arrow-heads) with few giant cells (red arrow) histopathologically suggestive of aneurysmal bone cyst (H&E; 40X).
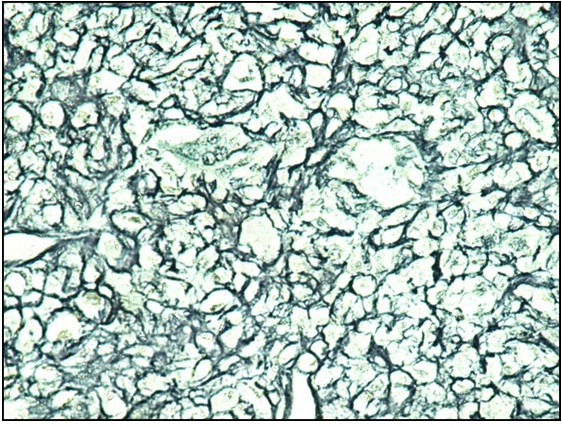
Section shows characteristic honeycomb pattern (reticulin; 100X).
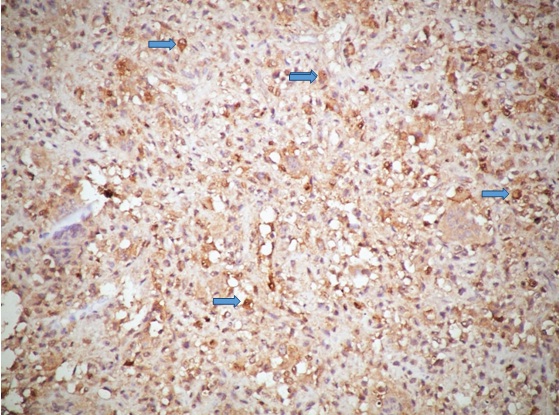
The tumour cells displayed diffuse cytoplasmic positivity with S-100(arrow) (Immunohistochemistry with S-100; 100X).
Discussion
Chondroblastoma is an uncommon benign tumour accounting for less than 1% of bone tumours. It mainly involves the epiphysis or epimetaphysis of long bones [3]. Chondroblastoma of calcaneum is an uncommon entity and calcaneal chondroblastoma with secondary aneurysmal bone cyst is even rarer. Only two cases of calcaneal chondroblastoma associated with secondary Aneurysmal Bone Cyst (ABC) have been reported till date [3,4]. Chondroblastoma (Codman tumour) was first described in 1931 by Codman [5]. It occurs predominantly in 10-20 years of age. Males are affected more than the females. The epiphyses in the femur, humerus and tibia (in descending order of frequency) account for about 70% of all chondroblastomas. Less common locations include foot bones [6,7], scapula, patella [8], radius, fibula, and temporal bone in skull [9]. Chondroblastoma of calcaneum is rare and accounts for only 0-6% of all chondroblastomas according to different series and review articles published in literature [3,5,10,11]. Clinical presentation of chondroblastoma varies from local pain and tenderness to joint effusion due to chronic reactive synovitis. Radiologically it usually presents as a well-defined, eccentric, osteolytic, lesion with a ring of sclerosis and intact cortical borders [5]. In our case similar radiological findings were found. Microscopically other than the findings in our case, chicken wire calcification, foci of haemorrhage and necrosis, foam cells and cholesterol clefts and areas of osteoid and osteo-chondroid may be found [5]. Chondroblastomas may exhibit cystic changes and according to a study by Fink et al., 24 (57.14%) of 42 chondroblastomas involving foot bones exhibit cystic changes [12]. However, fluid filled levels seen on radiological investigations have not always been confirmed as evidence of ABC [13]. Chondroblastoma is a reticulin rich tumour and shows characteristic honeycomb pattern with reticulin and cytoplasmic positivity with S-100 and both these findings were demonstrated in our case.
Chondroblastomas can be associated with aneurysmal bone cyst in about 15% of cases [10]. This association is more common in patients older than 20 years [4]. According to Huvos et al., the local recurrence was found to occur in virtually all cases of chondroblastomas with associated ABC [14]. Thus the identification and reporting of secondary ABC component in a chondroblastoma has clinical relevance as it has more chances of recurrence as compared to usual chondroblastoma i.e., without secondary ABC [3].
Conclusion
Although rare, chondroblastoma should always be considered in osteolytic lesion of calcaneum. The identification of secondary ABC component in chondroblastoma is important as the patient should be kept on extended follow-up in view of higher chance of recurrence.
[1]. Yeager KK, Mitchell M, Sartoris DJ, Diagnostic imaging approach to bone tumors of the footJ Foot Surg 1991 30(2):197-208. [Google Scholar]
[2]. Purohit S, Pardiwala DN, Imaging of giant cell tumour of boneIndian J Orthop 2007 41(2):91-96. [Google Scholar]
[3]. Guedes A, Barreto B, Soares Barreto LG, Athanazio DA, Athanazio PRF, Calcaneal chondroblastoma with secondary aneurysmal bone cyst: a case reportJ Foot Ankle Surg 2010 49(3):298.e5-8. [Google Scholar]
[4]. Ly JQ, LaGatta LM, Beall DP, Calcaneal chondroblastoma with secondary aneurysmal bone cystAJR Am J Roentgenol 2004 182(1):130 [Google Scholar]
[5]. Mirra JM, Chondroblastoma. In: Mirra JM, Picci P, Gold RH, edsBone tumours 1989 Philadelphia, PALea & Febiger:589-623. [Google Scholar]
[6]. Kilgore WB, Parrish WM, Calcaneal tumours and tumour-like conditionsFoot Ankle Clin 2005 10(3):541-65. [Google Scholar]
[7]. Zhang K, Gao Y, Dai H, Zhang S, Li G, Yu B, Chondroblastoma of the talus: a case report and literature reviewJ Foot Ankle Surg 2012 51(2):262-65. [Google Scholar]
[8]. Singh J, James SL, Kroon HM, Woertler K, Anderson SE, Jundt G, Tumour and tumour-like lesions of the patella – a multicentre experienceEur Radiol 2009 19(3):701-12. [Google Scholar]
[9]. Bui P, Ivan D, Oliver D, Busaidy KF, Wilson J, Chondroblastoma of the temporomandibular joint: report of a case and literature reviewJ Oral Maxillofac Surg 2009 67(2):405-09. [Google Scholar]
[10]. Bloem JL, Mulder JD, Chondroblastoma: a clinical and radiological study of 104 casesSkeletal Radiol 1985 14(1):1-9. [Google Scholar]
[11]. Turcotte RE, Kurt AM, Sim FH, Unni KK, McLeod RA, ChondroblastomaHum Pathol 1993 24(9):944-49. [Google Scholar]
[12]. Fink BR, Temple HT, Chiricosta FM, Mizel MS, Murphey MD, Chondroblastoma of the footFoot Ankle Int 1997 18(4):236-42. [Google Scholar]
[13]. Kahmann R, Gold RH, Eckardt JJ, Mirra JM, Case report 337: cystic chondroblastoma of calcaneusSkeletal Radiol 1985 14:301-04. [Google Scholar]
[14]. Huvos AG, Marcove RC, Chondroblastoma of bone. A critical reviewClin Orthop 1973 (95):300-12. [Google Scholar]