Bilateral Clavicle Fractures: A Report of Three Cases
Devendra Lakhotia1, Kavin Khatri2, Vijay Sharma3, Kamran Farooque4, Swati Sharma5
1 Assistant Professor, Department of Orthopaedics, Institute for Medical Sciences and Research Centre, Jaipur National University, Jagatpura, Jaipur, India.
2 Assistant Professor, Department of Orthopaedics, GGS Medical College, Faridkot, India.
3 Additional Professor, Department of Orthopaedics, AIIMS, New Delhi, India.
4 Additional Professor, Department of Orthopaedics, AIIMS, New Delhi, India.
5 Junior Resident, Department of Orthopaedics, MGMC, Jaipur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Devendra Lakhotia, Assistant Professor, Department of Orthopaedics, Jaipur National University, Jagatpura, Jaipur, India.
E-mail: drdevendra.ortho@gmail.com
Bilateral clavicle fractures are uncommonly reported in the literature with the incidence being less than 0.5% of all the clavicle fractures. Bilateral clavicle fractures are caused either by high-energy transfer of compression forces across both shoulder girdles or by a direct trauma to one clavicle followed by that to the other clavicle. These fractures could be missed due to their association with more severe chest injuries or a more symptomatically displaced fracture on one side or due to inadequate chest radiographs. We report three cases of traumatic bilateral clavicle fractures with three modes of injuries in different age groups. All the fractures were treated conservatively with good functional outcomes without any sequelae. Bilateral clavicle fractures should be actively sought by every trauma team with proper clinical examination and chest radiographs including both shoulder joints in high-energy trauma cases or with bilateral shoulder compression injuries.
Compression, Incidence, Shoulder, Trauma
Case Series
We have encountered three cases of bilateral clavicle fractures with different modes of trauma in three different age groups. One of these patients had a high-velocity roadside accident while the other case suffered a crush injury between a wall and a tractor. In the third case, a motorcycle fell over the patient. All of the fractures united well after conservative treatment with the return of normal functional activity. With the increasing incidence of high-energy trauma, we may encounter more of these injuries in the future.
Case 1
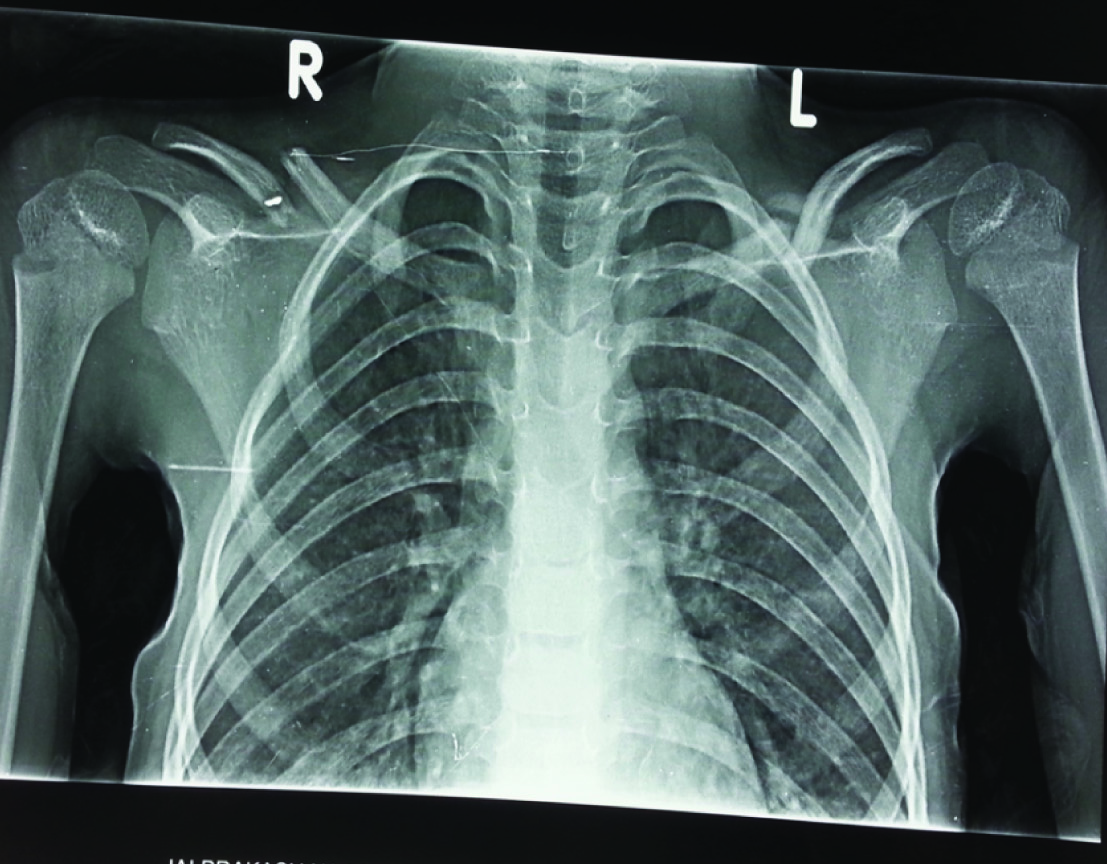
A 6-year-old girl presented to our hospital with pain swelling and bony instability over both the midclavicular regions. She was unable to move both of her shoulder girdles due to pain. She fell off from a stationary motorcycle and then the motorcycle fell over her. The patient had a history of a short period of unconsciousness followed by one episode of vomiting. Her GCS score was to be normal when brought to the hospital after few hours of the injury. CT scan head was found normal. X-ray chest with bilateral shoulders revealed displaced mid-clavicle fractures on both the sides [Table/Fig-1]. She had no neurovascular injuries in any of her upper limbs. The trauma team managed the fractures with a figure-of-8 bandage with shoulder slings conservatively. The patient was observed for 24 hours for a minor head injury that she sustained and was discharged thereafter. She was reviewed in outdoor at 3 weeks, 6 weeks and 12 weeks respectively. Both clavicles united in acceptable positions with full, pain-free shoulder function bilaterally [Table/Fig-2a,b].
Radiograph of a six-year-old female shows displaced bilateral mid-clavicle fractures.
Clinical photographs of a six-year-old female shows full functional recovery of shoulder 6 weeks after the trauma.

Case 2
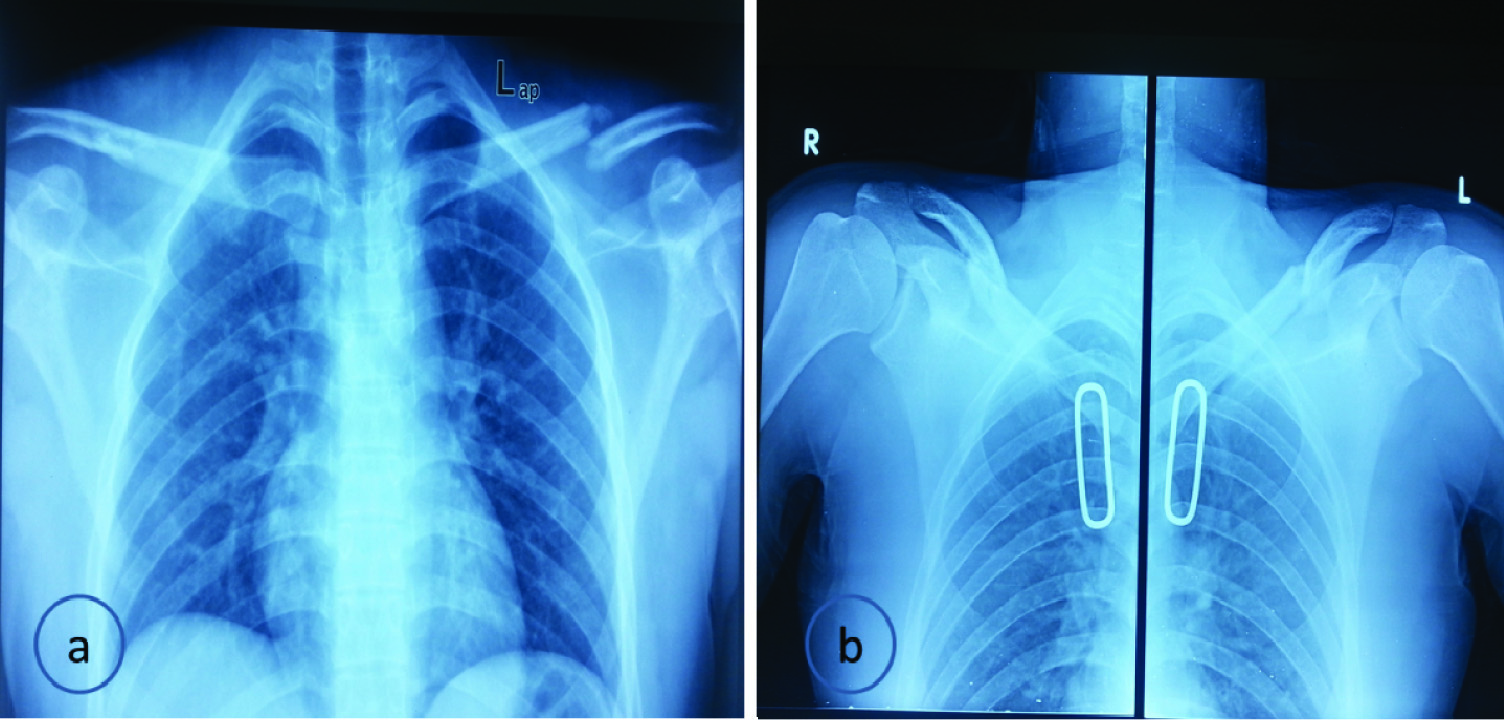
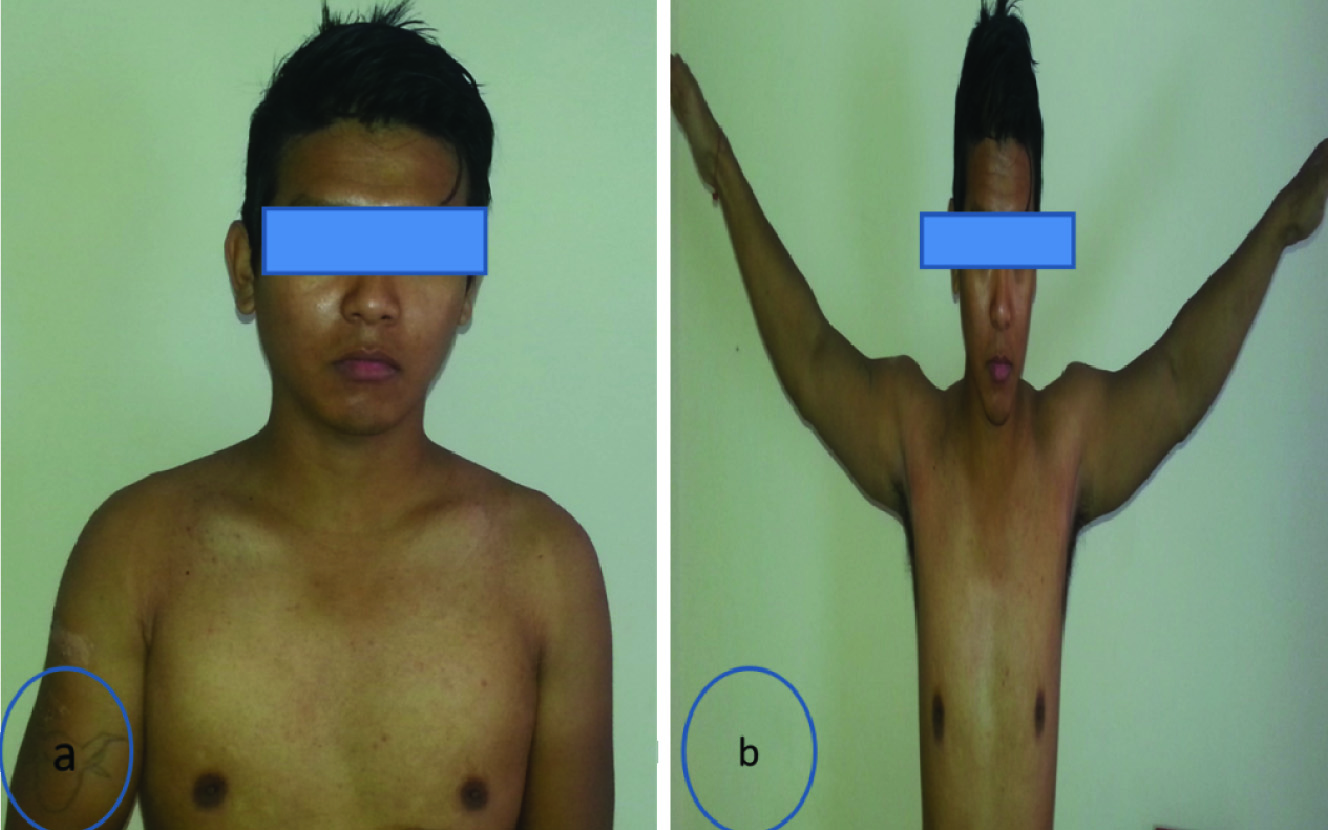
A 25-year-old man was involved in a high-velocity road traffic accident when his bike skidded on a road divider. He complained of pain on the left upper chest wall and in the left clavicle region. On examination he was found to be hemodynamically stable. He sustained a blunt chest injury with tenderness and bruises over the left upper chest wall. He was found to have multiple rib fractures on the left side along with a left clavicle fracture [Table/Fig-3a] on initial evaluation. The patient had no lung injuries and had a normal respiratory function. He was treated with analgesics, chest physiotherapy and mobilization for chest injury. A clavicle brace with arm sling was given for the fractured clavicle. He complained of pain in the right clavicular region during the follow-up after three days. Clavicle fractures were detected on both sides when a repeat roentgenogram was taken to include both clavicles. He made an uneventful recovery from his chest injuries. Both clavicles united well [Table/Fig-3b] on conservative treatment with minimal deformity [Table/Fig-4a]. He had excellent shoulder function at 12 weeks follow-up [Table/Fig-4b].
Radiograph of a 25-year-old male showing: (a) displaced left mid-clavicle fracture; and (b) follow-up radiograph at 12 weeks showing healing of bilateral clavicle fractures.
Clinical photographs showing: (a) minimal deformity of bilateral clavicles; and (b) full functional recovery of shoulders at12 weeks after trauma.
Case 3
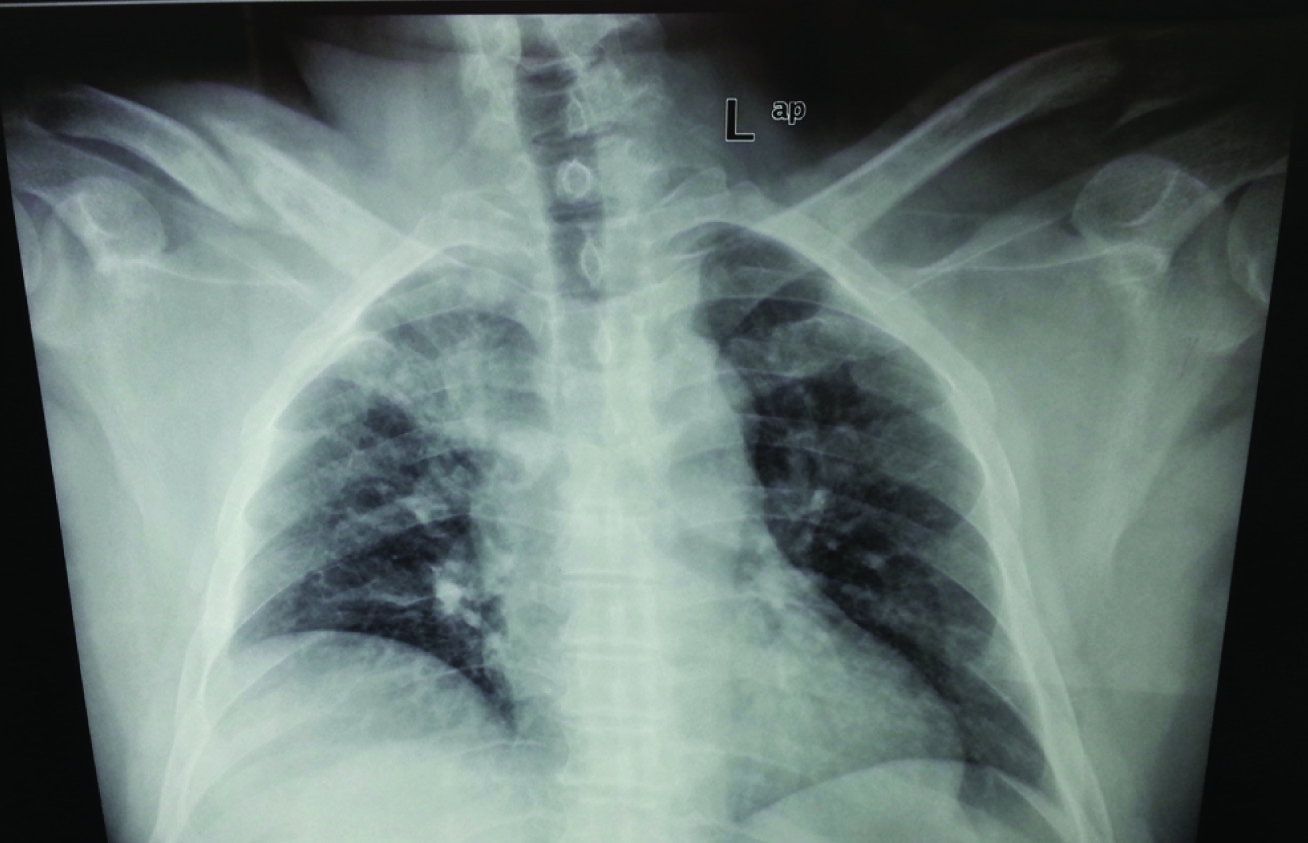
A 45-year-old man was crushed between a tractor and a wall while working in the field. He was conscious when he came to the hospital complaining of pain and swelling in bilateral clavicular regions. The patient had contusion and superficial bruises on the left shoulder which faced the wall at the time of injury. On radiological examination he was found to have bilateral clavicular fractures [Table/Fig-5]. On the right side, there was a mid shaft fracture and on the left, the fracture was at the lateral end of the clavicle. The chest and pelvis were screened for injuries and were found to be normal. Bilateral arm slings were applied. Radiological and clinical union of the fractures was evident at 12 weeks with normal shoulder function bilaterally.
Discussion
Clavicle fractures are common injuries in all age groups [1]. They account for 2% to 5% of all the fractures with the incidence in children being >10% [2,3]. Although unilateral clavicle fractures are commonly encountered, bilateral clavicle fractures have been reported extremely rarely in the literature [4,5]. The incidence of bilateral involvement is less than 0.5% of all the clavicle fractures [2,6,7]. Conservative management has been the preferred treatment modality for most of the clavicle fractures because of the high complication rates reported after surgical treatment [8]. But there are evidences in the literature that suggest a high risk for nonunion or shoulder dysfunction after non-operative treatment in bilateral clavicle fractures [9–11]. The mechanism of sustaining bilateral clavicle fractures is different from that of a unilateral clavicle fracture. They are often caused by a compressive force across both shoulder girdles, direct blows to both shoulder girdles or an indirect blow such as a fall onto the shoulder [5,9]. Bilateral clavicle fractures are usually associated with high-energy trauma and therefore are associated with other concomitant injuries.
In the three cases described above, mode of trauma was different but all of them involved a high-energy transfer of forces across the shoulder joint. Of these patients who suffered bilateral clavicle fractures, one patient (case 1) had an associated minor head injury followed by an uneventful recovery whereas another had (case 2) chest injuries with multiple rib fractures which were treated conservatively. The third patient (case 3) with bilateral clavicle fractures (midshaft on one side and lateral-end on the other side) had a compression injury across the shoulder joint.
In one of these cases (case 2), the clavicle fracture on one side was missed on initial examination and was detected only when the patient was re-examined subsequently and radiographs were taken on large films that included both clavicles. When evaluating retrospectively, it was concluded that the undisplaced fracture was not detected on the initial radiograph [Table/Fig-3a].
Radiograph of a 45-year-old male show displaced right mid-clavicle fracture and minimally displaced left lateral-end clavicle fracture.
Previous literature favoured operative intervention for bilateral clavicle fractures, especially in cases with compromised ventilatory function [12,13], though Sutherland AG et al., showed good functional results with conservative management of bilateral clavicle fractures. In all of our three cases, conservative management was given. All the patients returned to normal shoulder function within 12 weeks [5].
Conclusion
Bilateral clavicle fractures are not as uncommon as has been illustrated in the previous literature. The trauma team should be more vigilant, especially in high-energy trauma cases to detect and treat such injuries. Although we achieved good functional results with non-operative treatment in all our cases, there is still a need of a comparative study as these injuries will be quite more common in the near future.
[1]. Nowak J, Holgersson M, Larsson S, Sequelae from clavicular fractures are common: a prospective study of 222 patientsActa Orthop 2005 76(4):496-502. [Google Scholar]
[2]. Postacchini F, Gumina S, De Santis P, Albo F, Epidemiology of clavicle fracturesJ Shoulder Elbow Surg 2002 11(5):452-56. [Google Scholar]
[3]. Nordqvist A, Petersson C, The incidence of fractures of the clavicleClin Orthop Relat Res1994(300):127-32. [Google Scholar]
[4]. Puranik G, Gillham N, Bilateral fractured clavicles with multiple rib fracturesEmerg Med J 2007 24(9):675 [Google Scholar]
[5]. Sutherland AG, Knight DJ, Bilateral fractured clavicles—a pair of casesActa Orthop Belg 2000 66(3):306-07. [Google Scholar]
[6]. Nowak J, Mallmin H, Larsson S, The aetiology and epidemiology of clavicular fractures. A prospective study during a two-year period in Uppsala, SwedenInjury 2000 31(5):353-58. [Google Scholar]
[7]. Throckmorton T, Kuhn JE, Fractures of the medial end of the clavicleJ Shoulder Elbow Surg 2007 16(1):49-54. [Google Scholar]
[8]. Rowe CR, An atlas of anatomy and treatment of midclavicular fracturesClin Orthop Relat Res 1968 58:29-42. [Google Scholar]
[9]. Hargan B, Macafee AL, Bilateral pseudarthrosis of the claviclesInjury 1981 12(4):316-18. [Google Scholar]
[10]. Kloen P, Bilateral clavicle non-unions treated with anteroinferior locking compression plating (LCP): a case reportActa Orthop Belg 2004 70(6):609-11. [Google Scholar]
[11]. O’Connor D, Kutty S, McCabe JP, Long-term functional outcome assessment of plate fixation and autogenous bone grafting for clavicular non-unionInjury 2004 35(6):575-79. [Google Scholar]
[12]. Bonnevialle N, Delannis Y, Mansat P, Peter O, Chemama B, Bonnevialle P, Bilateral clavicle fracture external fixationOrthop Traumatol Surg Res 2010 96(7):821-24. [Google Scholar]
[13]. Jubel A, Andermahr J, Schiffer G, Tsironis K, Rehm KE, Elastic stable intramedullary nailing of midclavicular fractures with a titanium nailClin Orthop Relat Res 2003 (408):279-85. [Google Scholar]