Giant Sialolith of Wharton’s Duct Treated Economically in a Poor Patient
Preetkanwal Singh1, Sumita Singh2, Mayank Vermani3, Sunny Garg4, Ashok Gupta5
1 Professor, Department of Oral and Maxillofacial Surgery, National Dental College, Derabassi, Punjab, India.
2 Senior Resident, Department of Oral and Maxillofacial Surgery, National Dental College, Derabassi, Punjab, India.
3 Senior Resident, Department of Oral and Maxillofacial Surgery, JCD Dental College, Sirsa, Haryana, India.
4 Private Practitioner, Maur Mandi, India.
5 Reader, Department of Oral and Maxillofacial Surgery, JCD Dental College, Sirsa, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mayank Vermani, House no. 91, Sector 16, Hisar, Haryana-125001, India.
E-mail: mayank.vermani@gmail.com
Salivary gland pathology, Sialolithotomy, Salivary stone, Swelling on floor of mouth
A 35-year-old male was referred to the Department of Oral and Maxillofacial Surgery with a chief complaint of pain and swelling in the floor of the mouth on the left side. He also complained of thick fluid discharge from the floor of the mouth [Table/Fig-1]. History dated back to 4-5yrs when the patient first noticed the swelling. Since two months, the patient experienced an exacerbation of the symptoms along with associated swelling in the left submandibular region during meal times.
Intraoral photograph showing swelling in the floor of the mouth.
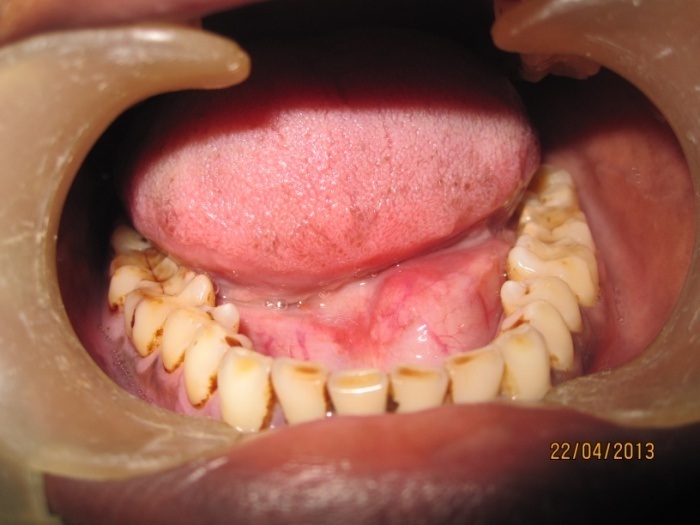
Extraorally there was no swelling or asymmetry at the time of examination. Intraorally, bimanual palpation revealed inflammation and a hard stone like structure along the left Wharton’s duct in the premolar region. There was thick turbid fluid discharge from the duct orifice. The left submandibular gland was tender on palpation. Occlusal radiograph revealed a large radiopacity located in the region of left Wharton’s duct [Table/Fig-2]. A diagnosis of sialolithiasis of the left Wharton’s duct was achieved. Under local anaesthesia, transoralsialolithotomy was performed via intraoral approach [Table/Fig-3].
Mandibular occlusal view X-ray showing a large radiopaque mass in the left floor of the mouth.

Sialolith from left Wharton’s duct explored out and removed.

Traction suture was placed behind the sialolith to prevent its posterior displacement. An antero-posterior incision was made in the mucosa parallel to the duct extending from the canine to the first molar region on the left side. After reflection of tissue, the large stone became visible and blunt dissection was done around it. The giant sialolith was removed and the surgical wound was thoroughly irrigated and checked for any satellite stones. Sutures were placed at the level of mucosa and no attempt was made to suture the duct lining [Table/Fig-4].
Surgical wound sutured with interrupted 3-0 silk.

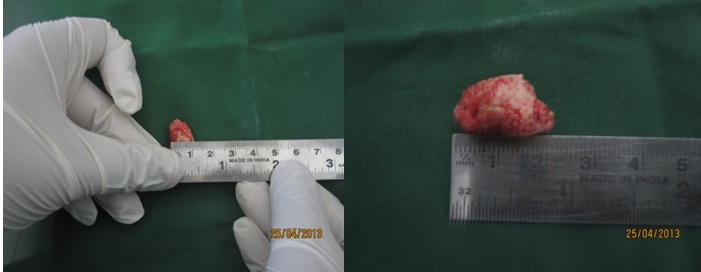
The obtained sialolith was a hard, oval, rough and yellowish mass. It measured 22x16mm and weighed 7gms. The patient was followed up for six months and was asymptomatic [Table/Fig-5].
Excised giant sialolith, measuring 22x16mm.
Discussion
Calculi greater than 15mm in size are considered giant sialoliths. The largest sialolith reported in the literature was 70mm in length in the Wharton’s duct and described as having Hen’s egg size [1]. According to Briddle RJ et al., the submandibular gland hosts the largest stones with the largest reported being 6cm in length [2]. The submandibular gland is more susceptible to the development of salivary calculi. Common radiographic techniques used to diagnose sialolithiasis are panoramic and occlusal views. In contrast to small sized calculi, 20%-30% of which are radiolucent, giant sialoliths are mostly radiopaque and are easily depicted on radiographs. Occlusal view was chosen for radiographic examination because of the poor economic status of the patient, which confirmed the diagnosis. Differential diagnosis of a sialoliths may include ranula, sialadenitis, calcified lymph node, impacted tooth or a foreign body, phlebolith or myositis ossificans [3]. Effective treatment depends upon the location of the stone. It is generally agreed that calculi in the anterior and middle parts of the submandibular duct up to the lingual nerve should be removed intraorally as transoralsialolithotomy is less traumatic and allows avoidance of gland excision. If the stone is not palpable, it is advised to wait until the stone increases in size or may even be removed spontaneously. Occasionally stones located more proximally behind the posterior border of mylohyoid muscle (with recurrent episodes of obstruction) may require extraoral approach [4]. Restoration of normal salivary secretion is the treatment objective for giant as well as standard sized stones. Disadvantage of the new techniques are very high cost of equipment. Therefore, surgical removal by transoralsialolithotomy by intraoral approach is still easy and time tested method for patients who cannot afford costly treatments.
[1]. Saluja H, Kasat VO, Mahindra U, Giant Sialolith in the Wharton’s duct causing sialo-oral fistula: a case report and review of literatureJ Orofac Sci 2012 4:137-42. [Google Scholar]
[2]. Briddle RJ, Arora S, Giant sialolith of the submandibular glandRadiology Case Reports 2008 3:101-05. [Google Scholar]
[3]. Mandel L, Hatzis G, The role of computerized tomography in diagnosis and therapy of parotid stones: a case reportJ Am Dent Assoc 2000 131:479-82. [Google Scholar]
[4]. Miloro M, Peterson’s Principles of oral and maxillofacial surgery Second edition 2004 1:671-77. [Google Scholar]