Adenolipoma of the Breast: A Clinicoradiological Entity and Pathologist’s Dilemma!
Dharma Ram1, Veda Padama Priya Selvakumar2
1 Resident, Department of Surgical Oncology, Rajiv Gandhi Cancer Institute, Delhi, India.
2 Consultant, Department of Surgical Oncology, Rajiv Gandhi Cancer Institute, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dharma Ram, Rajiv Gandhi Cancer Institute & Research Centre, Rohini Sec 5, New Delhi-85, India.
E-mail: drdharmapoonia@gmail.com
Breast hamartomas are benign lesions composed of variety of normal breast components arranged in disorganized manner. These are rare and classified as adenolipoma, fibrolipoma, adenofibrolipoma, etc. Clinically these present as painless well-circumscribed, mobile lumps of breast. Incidence and etiology remain obscure due to its rarity. These have been described in women in their 40’s or 50’s. Mammographically they appear non homogenous mass with circumscribed fatty masses. Histologically they appear as circumscribed masses with variable amount of fat, fibrous and glandular tissue. Here we are presenting adenolipoma in 29-year-old woman with review of literature.
Benign breast disease, Hamartomas, MR mammography
Case Report
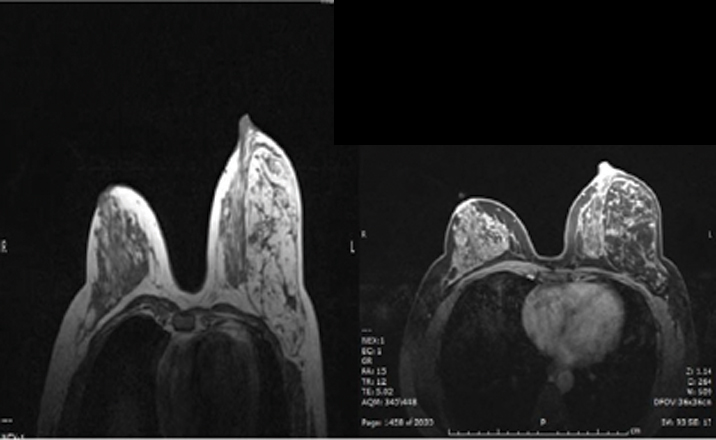
A 29-year-old unmarried premenopausal female presented to our institute with self-detected painless lump breast of four-year duration. She noticed sudden enlargement in size in last 6 months. On physical examination a firm, rounded, mobile lump of 8x9 cm size with defined margin at upper outer quadrant of left breast. No palpable axillary lymphadenopathy on left side was present. Contra lateral breast and axilla were unremarkable. On evaluation MR mammogram showed a huge 9.8x9.1x5.8 cm well circumscribed fatty mass predominantly in outer quadrants with enhancing thickened septae and small irregular soft tissue component showing type 1 (persistent) kinetics suggestive of hamartoma [Table/Fig-1]. Her Tru-cut biopsy from the lump showed stromal and adipose tissue hyperplasia. Stromal tissue was composed of spindle cells in collagenous stroma with no evidence of nuclear atypia or mitosis suggestive of benign phylloides tumour.
MR mammogram showing well curcumscribed fatty mass with type 1 kinetics.
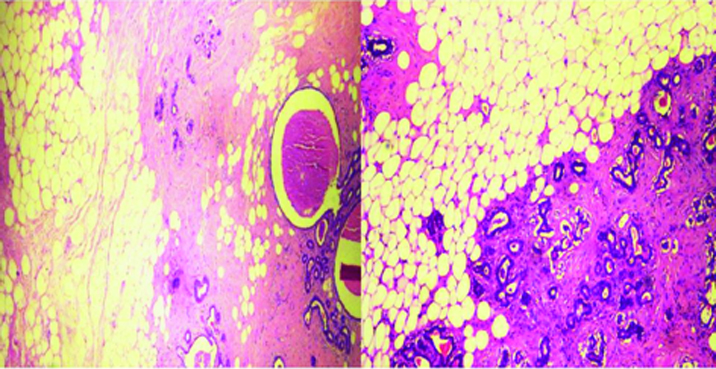
Hence with a clinical diagnosis of benign breast disease, she underwent lumpectomy. Specimen on gross appearance showed encapsulated yellow soft mass measuring 9x9 cm. On pathological examination a solid homogenous and lobulated mass with white streaks throughout was present. On microscopic examination well circumscribed mass with psuedocapsulated lesion composed of mature adipose tissue, breast duct and lobules surrounded by fibro collagenous tissue was seen. Features were suggestive of a hamartomatous lesion likely adenolipoma [Table/Fig-2]. She is on regular follow-up since than and currently disease free past 2-year of surgery.
Well circumscribed with pseudocapsulated lesion composed of mature adipose tissue, breast duct and lobules surrounded by fibro collagenous tissue.
Discussion
This hamartoma consistsed of a disorganized collection of mammary tissues including duct and lobules, fat and fibrous tissue as well as smooth muscles admixed in varying proportions. First literature description of adenolipoma was reported by Spalding in 1945 as an uncommon breast lesion variously called fibroadenolipoma, hamartoma or post lactational tumours [1]. This hamartoma consisted of a disorganized collection of mammary tissues including duct and lobules, fat and fibrous tissue as well as smooth muscles admixed in varying proportions. Adenohibernoma, myoidhamartoma and chondrolipoma represent other rare variants of hamartoma. Adenolipoma is usually a soft, mobile and well defined mass and can be misdiagnosed as other benign tumours [2–4].
They are uncommon entity and mostly reported as case reports. As of our knowledge largest single series featuring adenolipoma was reported by Arrigoni et al., with total 10 cases. He reviewed pathology of benign breast lesions. Reported incidence in literature is 0.1 to 0.7% of all benign breast lesions [5]. It is known that hamartomas result more from improper development in the organ rather than from tumorous process. The most characteristic histological feature of hamartomas is the presence of lobules within a fibrotic stroma. Coincidental malignancy, very rarely, can occur in mammary hamartomas. However, it is still not clear whether malignant lesion derives from the hamartoma itself, or is an incidental finding, that initiates nearby and extends into the hamartoma afterwards. The lesion generate the appearance of breast within a breast on histopathological examination [6].
Jones et al., reported their microscopical study of 17 cases of breast hamartomas and reported four different patterns: circumscribed fibrocystic changes with fat, smooth muscle or collagen, fibroadenoma with fat or cartilage, fibroadenoma with lobules and adenolipoma [7].
Clinical differential of adenolipoma includes fibroadenoma & phylloides tumour. Clinically it is not possible to differentiate but on pathology it’s rather simple. Lobular structure is not a common feature in fibroadenoma and the disorganized arrangement of lobular structures is helpful to distinguish adenolipoma from fibroadenoma. Adenolipoma shows less architectural organization compared to fibroadenoma, which also tends to have a less cellular stroma. Similarly, the stroma in adenolipoma is less cellular than those of phyllodes tumour and cleft like epithelium-lined spaces are not seen. Given that adenolipoma histologically resembles normal breast tissue or breast tissue with non-specific benign changes, it is very easy to make a diagnosis of fibroadenoma with knowledge of the clinical and/or mammographical findings [2,8].
Surgical removal is the curative method for breast hamartomas [9,10]. If there is a coincidental epithelial malignancy in the lesion, there is a potential for recurrence. Excision and histological examination is necessary for a differential diagnosis and also for any epithelial lesions of the hamartoma.
Conclusion
Adenolipomas are clinically and radiologically quiet characteristic disease but it deceive pathologist. Hence high index of suspicion needed to correctly diagnose it. We report this case for its unique clinicoradiological feature. In addition we want to draw awareness about this benign pathology.
[1]. Spalding JE, Adenolipoma and lipoma of the breastGuy’s Hosp Rep 1945 94:80-82. [Google Scholar]
[2]. Fatemeh NILI, parastoo GHABARI, Alireza GHANADAN, Adenolipoma of breastMalaysian j pathol 2015 37(1):67-70. [Google Scholar]
[3]. Feder JM, de Paredes ES, Hogge JP, Wilken JJ, Unusual breast lesions: radiologic-pathologic correlationRadiographics 1999 19:S11-S26. [Google Scholar]
[4]. Rosen PP, Rosen’s Breast Pathology 2001 2nd editionPhiladelphiaLippincott Williams & Wilkins:779 [Google Scholar]
[5]. Arrigoni MG, Dockerty MB, Judd ES, The identication and treatment of mammary hamartomaSurg Gynecol Obstet 1971 133:577-82. [Google Scholar]
[6]. Tavassoli FA, Devilee P, Pathology and Genetics: Tumours of the Breast and Female Genital Organs 2003 LyonIRCA press:103 [Google Scholar]
[7]. Jones MW, Norris HJ, Wargotz ES, Hamartomas of the breastSurg Gynecol Obstet 1991 173(1):54-56. [Google Scholar]
[8]. Brebner DM, Cosmann B, Shapiro J, Lipotoma of the breast diagnosed by lm and xeromammographyS Afr Med J 1976 50(18):685-88. [Google Scholar]
[9]. Barbaros U, Deveci U, Erbil Y, Budak D, Breast hamartoma: a case reportActaChir Belg 2005 105:658-59. [Google Scholar]
[10]. Guray M, Sahin AA, Benign breast diseases: classification, diagnosis, and managementOncologist 2006 11:435-49. [Google Scholar]