Successful endodontic therapy in an immature tooth is challenging, as it does not have definite apical stop to achieve complete debridement and to limit the obturation [1]. Traditionally, treatment method used for teeth with open apices has been cleaning and filling the canal with a temporary paste like calcium hydroxide to induce the formation of calcified tissue at the apex. The process is termed as apexification [2]. Most commonly used material for apexification is calcium hydroxide [3]. Though multiple visit apexification procedure using calcium hydroxide creates physiological hard tissue barrier but it has its own drawbacks like increased duration of treatment procedure [1], which leads to susceptibility to root fracture [4] and coronal microleakage [5]. To overcome these drawbacks of traditional apexification procedure, placement of artificial hard tissue barrier using different materials like Dentinal chips, Hydroxy appetite crystals, Portland cement, calcium sulphate, Mineral Trioxide Aggregate (MTA), Biodentine were suggested [6]. Among them, MTA is most commonly used due to its biocompatibility, good sealing properties and ability to induce hard tissue formation. But it is observed that single visit apexification using MTA has some clinical disadvantages like prolong setting time and poor handling characteristics [7].
The newer material such as Biodentine is now used as apical barrier, having the same composition like MTA. However, the poor handling characteristics and prolong setting time of MTA is overcome by adding setting accelerators and softeners to the powder which makes it more user-friendly [8].
When it comes to intracanal medicaments, calcium hydroxide is one of the most widely used intracanal medicament in endodontics today and remains the best medicament available to reduce residual microbial flora. It is a strong alkaline substance, which has a pH of approximately 12.5. In an aqueous solution, calcium hydroxide dissociates into calcium and hydroxyl ions that will lead to a lowered oxygen tension and an increase in the pH in the inflamed periapical tissues. With a high pH, calcium hydroxide has an excellent broad antimicrobial effect [9].
Other medicaments such as chlorhexidine digluconate when used as intracanal medicament have shown potent results in root resorption cases. The antibacterial mechanism of chlorhexidine is related to its cationic bisbigunide molecular structure. The cationic molecule is absorbed on the negatively charged cell membrane and cause leakage of intracellular components. Chlorhexidine also increases the pH of dentine, and therefore inhibits the activity of osteoclastic acid hydrolases in the periodontal tissues and activates alkaline phosphatase. Moreover chlorhexidine if applied to dentin binds effectively to hydroxapatite, providing a lasting reservoir of chlorhexidine after the completion of treatment [10].
Another medicament used was CMCP, which consists of 35% parachlorophenol in camphor. Phenol and phenol-derivative compounds have bactericidal activity. They disrupt bacterial cytoplasmic membranes, denature proteins and inactivate enzymes. They also liberate chlorine, a strong oxidizing agent that inactivates enzymes with sulphydryl groups [11,12].
Hence the purpose of this study was to evaluate the effect of calcium hydroxide, chlorhexidine digluconate and CMCP as an intracanal medicament on the sealing ability of the biodentin as an apical plug.
Materials and Methods
This invitro study was conducted in the Department of Conservative Dentistry and Endodontics, Mahatma Gandhi Dental College and Hospital, Jaipur from May 2015 to September 2015 after the approval by ethical committee of the university. In the present study recently extracted 72 human permanent teeth with single root were selected for the study. The teeth were stored in saline at room temperature at all times. Remaining periodontal tissues and calculus was removed. The teeth were radiographed and the teeth possessing internal and external resorption were not used in the study. To facilitate instrumentation, the crown portion of each tooth was removed at the level of Cemento Enamel Junction and to eliminate root length as a variable, 14mm root length was taken as standard length and kept in saline. All the roots were submerged in 20% sulfuric acid upto 3mm from the apex, and kept for 4 days for root resorption. One sample was cut longitudinally to look for root resorption under stereo microscope.
The canals were prepared up to appropriate working length using crown down technique with K file (Dentsply Maillefer, Tulsa, OK) and K3 system (Sybron Endo, Kerr Dental, California). Coronal flaring was done using #1, #2, #3 Gates Glidden drill (Dentsply Maillefer, Tulsa, OK). The roots were kept in moist gauge after instrumentation.
Then all the teeth were randomly divided into three groups. In group 1, calcium hydroxide (RC CAL Prime Dental products Ltd, India) was placed in root canals. In group 2, chlorhexidine digluconate (R4 Septodont, St. Maur-des-Fossés, France) was placed and in group 3, CMCP (Ammdent, India) was placed. The cotton pellets were placed in the access opening and the same was sealed with zinc oxide eugenol temporary restoration and were stored at 100% humidity and 37°C for seven days in all three groups. After seven days medicaments were removed with stainless steel hand files (Dentsply Maillefer, Tulsa, Switzerland) and 0.5% sodium hypochlorite (PT Asahimas chemicals Ltd, Indonesia) irrigation.
After removal of medicament, Biodentine (Septodont, St. Maur-des-Fossés, France) was mixed and placed with the help of finger plugger in apical third of resorbed roots. All apical plugs had the same thickness (4mm). Then, 40 K-file is placed 4mm short of root canal length with the help of a rubber stopper to remove the excess material. Radiographs were taken to ensure the proper placement and thickness of the Biodentine apical plug and teeth were stored at 100% humidity and 37°C. After complete set of Biodentine, the remaining portion of canals were obturated with gutta-percha using lateral condensation technique and the access cavities were sealed with composite resin restorative material after 24 hours.
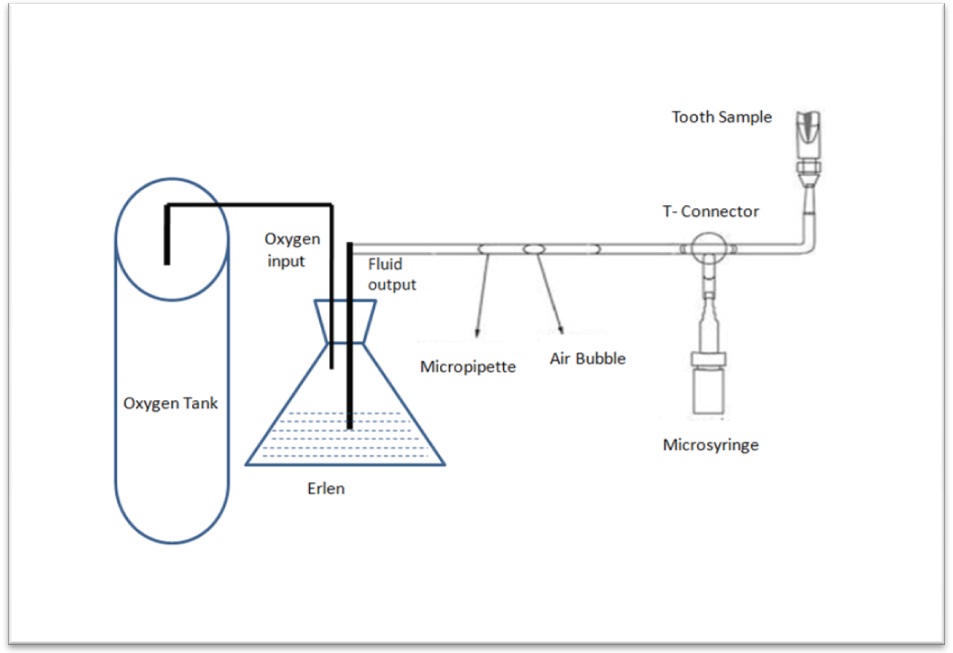
Then the roots were dried with compressed air and coated with two layers of varnish. All the 71 roots were connected with fluid filtration method for evaluating microleakage and bubbling movement in milliliter [Table/Fig-1]. After achieving balance in the system for 30 seconds, the first value of the bubble position in the micropipette was taken. Four subsequent values were taken with 2-minute time intervals (2, 4, 6 and 8 minutes). The same steps were repeated for the all remaining samples and the average value for all the time intervals were tabulated for statistical analysis.
A schematic representation of fluid filtration method.
Statistical Analysis
The data obtained were collected and entered into Microsoft Excel worksheet. Analysis of variance (ANOVA) test was applied and the statistical analysis was performed.
Results
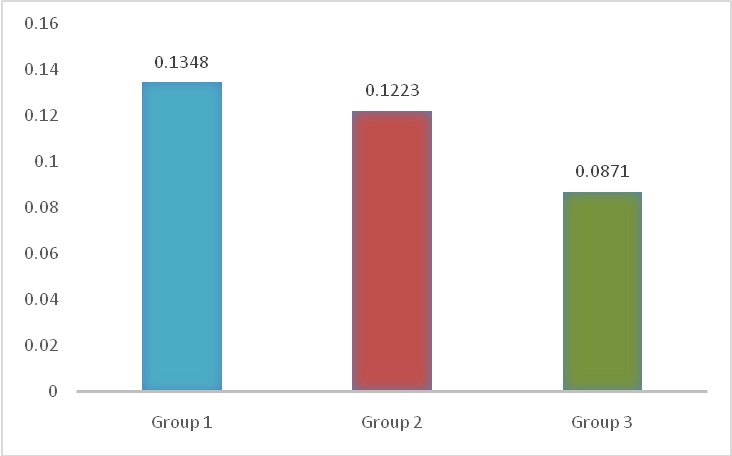
The results showed that there was presence of microleakage in all the three groups. In group 1 where calcium hydroxide was used as an intracanal medicament showed maximum microleakage followed by group 2 in which chlorhexidine digluconate was used and the least microleakage was seen in group 3 in which CMCP was used [Table/Fig-2].
Graphically represent the comparison of microleakage in milliliter between the three groups, group 1 represents calcium hydroxide; group 2 represents chlorhexidine digluconate and group 3 represents CMCP.
However, the results showed that there was no statistically significant difference between the three groups studied. On applying ANOVA, the p-value was found to be 0.419 which is definitely more than the reference level of 0.05. Hence p-value was not found to be statistically significant [Table/Fig-3].
All the 3 groups showed presence of microleakage with calcium hydroxide showing maximum microleakage with a mean of 0.1348(± 0.121 sd) and least was seen in CMCP with mean of 0.0871(± 0.075 sd). The p-value was not found to be statistically significant (ANOVA).
| Groups | Size | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | p value |
|---|
| Lower Bound | Upper Bound |
|---|
| Calcium Hydroxide (Group 1) | 24 | 0.1348 | 0.12189 | 0.02488 | 0.0834 | 0.1863 | 0.419 |
| Chlorhexidine Digluconate (Group 2) | 23 | 0.1223 | 0.16891 | 0.03522 | 0.0493 | 0.1954 |
| CMCP(Group 3) | 24 | 0.0871 | 0.07579 | 0.01547 | 0.0551 | 0.1191 |
| Total | 71 | 0.1146 | 0.12710 | 0.01508 | 0.0846 | 0.1447 |
Discussion
The present experimental study was designed to evaluate the effect of removal of previously placed calcium hydroxide, chlorhexidine digluconate and CMCP dressing and on the sealing ability of biodentine which is placed as an apical plug in immature simulated teeth.
For invitro studies, several methods have been used to create open apex teeth, so as to best simulate invivo conditions. They include over instrumentation with large files or the retrograde application of NiTi rotary files [13,14]. The disadvantages of these methods are that they create round apical foramen that may not resemble the natural resorption. In this invitro study, the method suggested by Ghoddusi et al., was used to create open apex teeth. In this method, 20% sulfuric acid resorbes root surface irregularly in a manner that may best simulate invivo conditions [15].
To disinfect non-vital immature tooth it is necessary to use a suitable intracanal medicament before placing apical barrier to ensure periapical healing [1]. However, the complete removal of intracanal medicament from dentinal walls is difficult as it can lead to micro leakage in apical plug [16]. In the present study, light instrumentation and copious irrigation with 0.5% sodium hypochlorite were used for removal of intracanal medicament.
Bani M et al., evaluated that 4mm apical plug of biodentine gave satisfactory result against apical leakage in comparison with 1 and 2mm of apical plug [17]. So in this present study 4mm apical plug of biodentine was placed to evaluate the apical leakage.
Various methods can be used to measure leakage around apical plug, such as dye penetration, light microscopic methods, fluid filtration method and Scanning Electron Microscope (SEM). But fluid filtration method has an advantage as it can quantify the amount of microleakage while other methods can only show the presence or absence of microleakage [18]. Other added advantages of fluid filtration method are that sample remains intact for future analysis, permitting the evaluation of sealing efficiency over time; the results are automatically recorded avoiding any operator bias; the results are very accurate because very small volumes can be recorded and no tracer is needed with the related problems of molecular size, affinity for dentin, or pH as major problems in the dye penetration method [19]. No intricate materials are required as in bacterial penetration studies or radioactive tracer studies [20]. Therefore, the fluid filtration method has been used to measure the leakage of apical plugs in this study. The result of our study showed some amount of microleakage is there in all the groups but are not significantly different.
In a study by Kim and Kim [21], calcium hydroxide medicated root canals showed significantly more apical leakage than ones without medication. Because calcium hydroxide cannot be removed completely from the apical 4mm of canal, it is likely that the remaining calcium hydroxide may interfere with the sealing ability of fillings materials.
In a study by Barbizam et al., it was reported that after the use of calcium hydroxide as an intracanal medicament the bond strength between Epiphany℡ sealer (a resin-based sealer) and dentin was reduced, they also suggested that it is due to the residue of calcium hydroxide which interfered with sealer adhesion to root dentin [22].
In a study by Akman M et al., it was also reported that calcium hydroxide when used as intra canal medicament reduces the push out bond strength of Biodentine [23].
In the present study calcium hydroxide also showed maximum leakage which is in co-ordinance with the other studies [21–23]. This is because of the residue of calcium hydroxide may interfere with the sealing of biodentine which can lead to microleakage.
However, on the other hand Nagas et al., showed that prior placement of calcium hydroxide increases the push out bond strength of biodentine due to chemical reaction between calcium hydroxide and calcium silicate based cements (Biodentine) which result in improve marginal adaptation of Biodentine [24].
Summarizing the results of previous it can be concluded that calcium hydroxide definitely affect the bond strength and sealing ability of Biodentine when used as an apical plug studies [21–24].
Another intracanal medicament used in this study was chlorhexidine digluconate, which have both bacteriostatic and bactericidal properties. It also has a unique property called substantivity that is ability to be adsorbed in the dentin and gradually released over time [25]. In the present study, chlorhexidine digluconate was used in liquid form as it can be easily removed. So chlorhexidine digluconate showed less microleakage in comparison with calcium hydroxide.
Hamidi et al., found that there is no significant difference in the apical seal when the root canals were medicated with chlorhexidine and calcium hydroxide [26]. This is in agreement with our study.
CMCP showed least microleakage in this study. In a study done by Messer and Chen they showed that within 24 hour upto 95% of the CMCP was lost from the root canal, so does not effect on the sealing ability of the material [27].
However, not much research was done to compare the effect of three different forms of intracanal medicaments on the sealing ability of biodentine apical plug. Furthermore research has to be done to justify their effect on apical seal.
Limitations
Within the limitations of the present study, the invitro condition used to store the tooth sample might not mimic the invivo condition completely that might affect the sealing of biodentine to root dentin.
Clinical Implications
One of the challenging conditions for the clinician is to treat the non vital teeth with open apex as it is difficult to disinfect and obturate. In the present study commonly used intracanal medicament were used to disinfect the nonvital teeth and showed their effect on the sealing ability of biodentine apical plug which can affect the long term prognosis of teeth. Hence judicious use of intracanal medicaments, complimented with a proper biodentine apical plug is necessary for treating immature non vital teeth.
Conclusion
Under the experimental condition of this study, all the groups showed some amount of microleakage. In present study it was found that when calcium hydroxide was used as medicament, there was more microleakage. This was due to the effect of residual calcium hydroxide which was left on the canal walls. Further in vitro studies may be necessary to study the long term effects of intracanal medicament on sealing ability of apical plug.