Introduction
Periodontal disease is a chronic inflammatory disease resulting in destruction of tissues and structures surrounding the teeth thus, if left untreated causes loss of teeth and ultimately results in edentulism, posing a great negative impact on individuals’ quality of life. Hence the global epidemiological data suggests periodontal disease to be one of a major burden on oral diseases. To reduce this burden it is necessary to know the true prevalence of the disease according to which proper initiatives can be formulated. India being home to nearly 1.2 billion people and one amongst the rapidly developing country, its population requires being systemically as well as orally healthy to lead a good quality of life. However due to large heterogenecity amongst its residing population in terms of geographical area, culture, education, socioeconomic status, a variety of oral diseases like periodontal diseases are prevalent here. Even though the early studies suggested that the population is highly susceptible to the disease, the true prevalence of periodontal disease has not been found yet due to paucity in literature available.
Aim
To systematically review the available literature taken from various parts of India and find the prevalence rate of periodontal disease amongst the general population of India.
Materials and Methods
A literature search was performed using PUB MED, COCHRANE and EMBASE databases on August 6, 2015. Following full text assessment a thorough references search was made and potential studies were included. A Quality assessment of retrieved articles from 2nd round was done using a self designed questionnaire and only field survey studies were included in the systematic review.
Results
The literature search yielded six studies which had performed field surveys to find the prevalence of periodontal disease in their respective areas. These studies have observed different sets of age groups and the same has been accomplished by using Community Periodontal Index (CPI) or Community Periodontal Index of Treatment Needs (CPITN). It was also found that no prevalence studies have been carried out in few North and North Eastern states and Union Territories of India.
Conclusion
Due to non-availability of same age groups in selected studies an overall prevalence rate could not be obtained. However, it was observed that few areas of states like West Bengal, Uttar Pradesh and Assam have reported a prevalence rate of periodontal disease of more than 85% in their general population. The data from the present systematic review calls for a combined initiative from the Government of India and Dental council of India to have a nationwide multicentric prevalence studies to obtain the true prevalence rate of periodontal disease in India and interventions should be provided for the same to maintain the oral health and quality of life of the affected population.
Chronic periodontitis, Community periodontal index, Dental health surveys
Introduction
Periodontal disease is a chronic inflammatory disease resulting in destruction of tissues and structures surrounding the teeth and manifests as a wide variety of inherited and acquired conditions affecting the periodontium, gingival diseases and destructive periodontal diseases (e.g., chronic periodontitis). Plaque induced gingivitis is confined to the gingival tissues, whereas the various other forms of periodontitis affect all of the components of the periodontium i.e., gingival, periodontal ligament, cementum and alveolar bone. In general, both conditions demonstrate all of the classic signs and symptoms of chronic inflammation, including redness and swelling of the tissues, loss of architectural form and reduced function. If the inflammatory response is not balanced by the host, or is left untreated, inflammatory destruction can be so severe as to put the teeth at risk and tooth loss can be the ultimate outcome of the periodontal disease. The prevalence of periodontal disease dates back to early human civilization as it was indicated by Paleopathological studies and recently the global epidemiological data suggests periodontal disease to be one of a major burden on oral diseases [1–5].
The current demographic data of India shows a population of over 1.2 billion people making it the second most populous country in the word contributing around 17.5% of the total world population [6]. An array of cultural, ethnic and demographic diversities is found amongst the people inhabiting here. Owing to this blending of cultural, ethnic and geographic factors there has been development of various pathologic differentiation and oral pathologies amid the individuals [7]. Also the difference in socioeconomic pattern midst the masses creates entirely different strata of healthcare exposure among the population of India.
The studies on the prevalence of periodontal disease in different populations are useful for not only determining the extent and severity of the disease, but also describe the rate of progression of the underlying condition and identifying the possible etiological factors of the disease. Thus the aim of this systematic review was to specify the prevalence of periodontal disease in the general population of India and same is accomplished by reviewing the literature on prevalence of periodontal disease systematically, combined with a quality assessment of the included studies.
The main objective of prevalence studies is to obtain the prevalence of the disease in a respective area and by assessing all the available studies on prevalence of periodontal disease carried out in various parts of India the authors have tried to obtain an overall prevalence rate of periodontal disease amongst the general population of India.
Materials and Methods
Focused Question: The focused question of the present systematic review was: What is the prevalence of periodontal disease amongst the general population of India?
Literature Search: Our literature search was performed on December 24, 2014, in the PUBMED and COCHRANE Library databases, because earlier search in EMBASE had not retrieved any additional results. PUBMED was searched with the following search strategy: “Periodontal disease” OR “Epidemiology” OR "Prevalence” AND "India". The search was updated on August 06, 2015, and supplemented by automatically weekly derived updates from PUBMED until August 10, 2015. No limits were implemented in our search queries. Owing to lack of sufficient studies, after assessing the full text, a comprehensive search of the references was carried out of retrieved articles.
Assessment of Relevant Studies: The authors independently assessed the studies in three rounds using PRISMA protocol [Table/Fig-1], based on a predefined criteria [Table/Fig-2], and Cohen’s kappa was calculated for each round. If in the first-round inclusion or exclusion criteria could not be assessed from the title and abstract, a full-text analysis was performed. After each round, discrepancies were discussed among the authors to reach consensus. A Fifth author was consulted if no consensus could be reached.
Assessment of the studies in three rounds using PRISMA protocol.
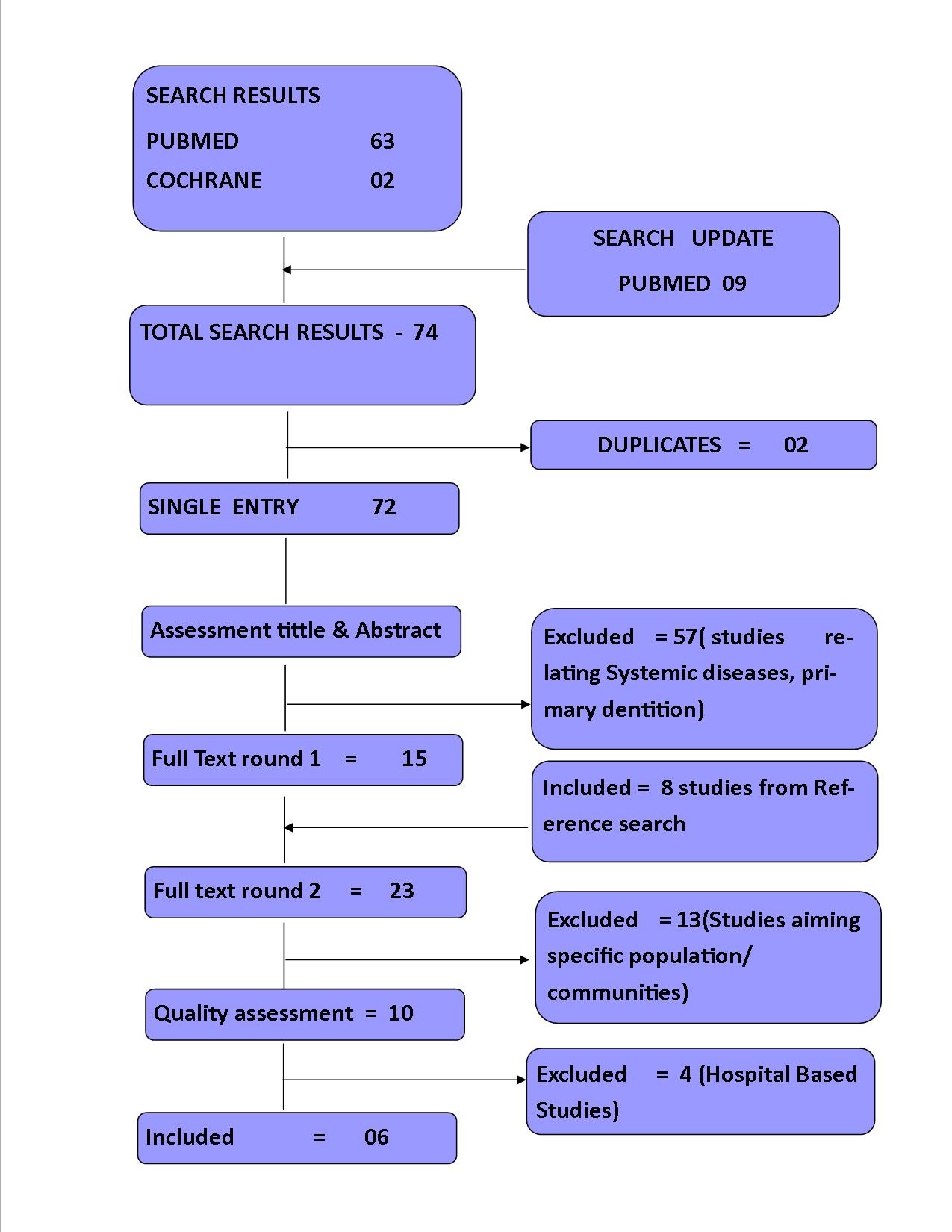
Independent assessment of the studies by the authors in three rounds using PRISMA protocol based on predefined criteria.
| Round 1 : Title and Abstract |
|---|
| Inclusion criteria |
| Periodontal disease in India as research theme |
| General (Adult population) as sample |
| Exclusion criteria |
| Case report |
| Review article |
| Case series |
| Systemic disease |
| Studies focusing special communities |
| Primary dentition |
| Round 2 : First Full Text Assessment |
| Inclusion criteria |
| Prevalence of periodontal disease in India as research theme |
| Exclusion criteria |
| Age is not reported |
| Lack of sufficient data for full text assessment |
| Round 3 : Second Full Text Assessment |
| Inclusion criteria |
| Prevalence is calculated |
| Data were provided to calculate prevalence |
| Exclusion criteria |
| Unclear how periodontal disease was diagnosed |
| Diagnostic index/test was not mentioned |
Quality Assessment of Included Studies: We used self designed guidelines to evaluate the quality of prevalence studies [Table/Fig-3]. The guidelines consist of 10 questions about sampling design, measurement methods and analysis carried out. For each question, the answers were given as “YES”, “PARTIAL” and “NO” to obtain an overall quality score for each article and accordingly points were awarded as 2, 1 and 0 respectively. The total points awarded for the 10 questions were divided by the total possible points i.e., the sum of the maximum possible points (the maximum possible point for one question here is 2). This was done to obtain the score in a fraction between 0 and 1. A score of 1 represents the highest quality. All articles that were included after the second full-text round were scored with these guidelines by the authors independently.
Guidelines to evaluate the quality of prevalence studies.
| Sampling |
| (1) | Are the samples obtained through field survey? |
| (2) | Does the survey design yield a sample of respondents representative of a defined target population? |
| (3) | Is the target population defined clearly? |
| (4) | Do the characteristics of respondents match the target population? |
| Measurement |
| (5) | Do the survey instruments yield reliable and valid measures of disease? |
| (6) | Are the data collection methods standardised? |
| (7) | Are the survey index reliable? |
| (8) | Are the survey index valid? |
| Analysis |
| (9) | Were special features of the sampling design accounted for in the analysis? |
| (10) | Do the data include confidence intervals for statistical estimates? |
Landmark Studies: The population of India has witnessed many epidemiologic studies on the prevalence of periodontal disease by many worldwide and national research scholars since 1940’s. Also India was the focus of World Health Organization (WHO) survey studies [11,12] during this period. These landmark studies were mentioned below [Table/Fig-4].
| Author | Year | Place | Observation | Conclusion |
|---|
| Marshall-Day and Shourie [8] | 1949 | Punjab Province | 568 people from 9 to 60 years of age | Periodontosis present in about 35% of the cases. |
| Mehta et al., [9] | 1953 | Bombay and Ratnagiri district | 2219 male subjects of low socioeconomic level in the age group 19-55 years | Periodontal disease is very high among this population. |
| Sanjana MK and Mehta FS [10] | 1956 | Bombay | Residents including 1,445 population in age group of 16-50 years | 83.2% generalized periodontal disease. |
| S. Ramfjord [11] | 1957-1963(as a part of WHO surveys) | Bombay and Bassein (present ’Vasai’) region | 1,677 urban and rural population using Ramfjord periodontal disease index | Prevalence of periodontal disease was close to 100% and starts after age 15; and at 17 years, 10% of Indian boys had periodontitis. |
| Greene JC [12] | 1960 (in parallel to WHO surveys with the aid of U.S. public health service | Bombay and Bassein (Vasai) region | 1,676 urban plus rural population using Russells’ periodontal index | 97% of the 11-17 year-old persons examined, had high prevalence of periodontal disease. |
| S. Rao and S. Tewani [13] | 1968 | Bombay | 1,200 males and females | 6.83% population were suffering from periodontosis. |
| Anil S and Hari S [14] | 1990 | Trivandrum (Kerala) | 2756 subjects | 36 % population was having periodontal disease. |
National Surveys: Two national surveys [15,16] were carried out in India to assess the oral health status of different states of India. These surveys were mentioned below [Table/Fig-5].
National surveys carried out in India to assess the oral health status of different states of India.
| Author | Year | Place | Findings |
|---|
| Mathur B and Talwar as a part of National Oral Health Survey aided by Dental Council of India, New Delhi [15]. | 2002-2003 | A three-stage sampling design was adopted to select 210 rural and 110 urban subjects in each of the age groups, viz. 5, 12, 15, 35-44, 65-74 years, from each homogeneous region comprising of a number of districts of each state and on the basis of geographical factors used by the Planning Commission. CPI index was used for disease assessment. | The prevalence reported was 57%, 67.7%, 89.6% and 79.9% in the age groups 12, 15, 35-44 and 65-74 years, respectively. |
| Shah N et al., [16] A multicentric study under the Directorate General of Health and as a collaborative programme between World Health Organization and Ministry of Health and Family Welfare, Government of India. | 2005 | 3,200 samples of age group 12, 15, 35-44 and 65-74 years from total of 22,400 persons in rural and urban areas of the selected districts of Arunachal Pradesh, Delhi, Maharashtra, Puducherry, Rajasthan, Orissa and Uttar Pradesh. | The highest prevalence in 65-74 years group was recorded in Maharashtra (96%), followed by Orissa (90%), Delhi (85.5%), Rajasthan (75%), Uttar Pradesh (68%) and Puducherry (55%). |
Results
Literature Search: The search resulted in 74 articles and after following the PRISMA protocol [Table/Fig-1] six studies were included [Table/Fig-6]. Two main reasons led to exclusion: first, the prevalence of periodontal disease was taken in patients with systemic disease or primary dentition; and second, the study population was not a general population but taken from “isolated” communities [Table/Fig-7], also four studies were excluded owing to their hospital based sample [Table/Fig-8]. Following full text assessment (Round 1) eight studies were included from the reference search. To quantify the decisions in the selection process, we performed a Cohen kappa analysis for each round of assessment: title and abstract ([kappa] = 0.721, p <0.001), full-text round 1 ([kappa] = 0.529, p = 0.001), and full-text round 2 ([kappa] = 0.691, p = 0.001). As shown in [Table/Fig-6], articles were published between 2000 and 2015. The total number of participants in the included studies ranged from 438 to 22,452 and were aged between 15 to 60 years and above.
| Author | Sample size | Age (years) | State | Prevalence Rate | Method of Assessment |
|---|
| Doifode VV et al., 2000 [17] | 5061 | 15 – 60 and above | Nagpur, Maharashtra | 34.8% | House to house survey by subject specialist |
| D. Kundu et al., 2011 [18] | 22,452 | 15-65 and above | West Bengal | 97.51% | CPITN |
| A singh et al., 2012 [19] | 1026 | 26 -56 and above | Meerut, UP | 90 % | CPITN |
| KP Nanaiah et al., 2013 [20] | 1100 | 15-18 | Mangalore, Karanataka | AP - 0.36 and CP - 1.5%. | CPI and microbiologic examination |
| D Goswami, 2014 [21] | 438 | 15-64 & above | Kamrup, Assam | 85.62% | CPITN |
| TS Sekhon et al., 2015 [22] | 1680 | 15 and above | Belgaum, Karnataka | 61% | CPITN |
CPITN – Community Periodontitis Index of Treatment Needs; CPI – Community Periodontal index, AP – Aggressive periodontitis, CP – Chronic Periodontiti
Studies assessing specific groups/communities.
| Author | Place | Community Assessed |
|---|
| Rekha R et al., 2002 [23] | Banglore City, Karnataka | Confectionary Workers |
| Jain M et al., 2009 [24] | Udaipur, Rajasthan | Terapanthi Svetambar Jain monks |
| Chandra Shekhar BR et al., 2011 [25] | Mysore city, Karnataka | Municipal workers |
| Agrawal A et al., 2011 [26] | Udaipur, Rajasthan | Juvenile detention center |
| Reddy V et al., 2012 [27] | Karnataka | Life imprisoned inmates of central jails |
| Nagarajappa R et al., 2013 [28] | Jhalawar, Rajasthan | Kota stone workers |
| Kadanakuppe S et al., 2013 [29] | Ramanagar district, karnataka | Iruliga tribal community |
| Sanadhya S et al., 2013 [30] | Jaipur, Rajasthan | Salt workers (sambhar lake) |
| Gambhir RS et al., 2013 [31] | Chandigarh | Transport workers |
| Dayakar MM et al., 2014 [32] | Mangalore, Karnataka | Prison inmates |
| Torwane NA et al., 2014 [33] | Bhopal, Madhya Pradesh | Eunachs community |
| Solanki J et al., 2014 [34] | Jodhpur, Rajasthan | Stone mine workers |
| Aapaliya P et al., 2015 [35] | Kutch, Gujarat | Seafarers (mundra port) |
Studies assessing hospital based population.
| Author | Sample size | Age | State | Prevalence Rate | Method of Assessment |
|---|
| Bansal M et al., 2015 [36] | 500 | 15-74 | Varanasi, Uttar Pradesh | the prevalence of periodontal disease was found to be 96.30% | CPITN |
| S fotedar et al., 2014 [37] | 351 | 21-70 | Shimla, Himachal Pradesh | 75 .1% | CPI |
| S. Sanadhya et al., 2015 [38] | 1200 | 30-49 | Udaipur, rajasthan | (51.1%) rural population and (43.1%)urban | CPI and loss of attachment |
| Peter KP et al., 2014 [39] | 700 | 30 or more | Aurangabad, Maharashtra | 72% of the individuals having at least one site with CAL ≥3mm. Almost 41% of population had at least one site with CAL ≥5mm almost 21% of individuals had at least three sites with CAL ≥5mm. | -Oral Hygiene Index (Greene and Vermillion)-Plaque Index (Turesky-Gilmore-Glickman modification of the Quigley Hein Plaque Index 1970)- Gingival Index (Loe and Silness 1967).-Probing Depth (PD)-Clinical Attachment Level (CAL) |
Results of Quality Assessment: The results of the quality assessment per question for all 10 Studies included after 2nd round and their respective score for each question was mentioned in [Table/Fig-9].
Quality assessment score of included studies and studies having hospital based population.
| Author | Questions | Maximum |
|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Points scored | Total possible score | Score (fraction) |
|---|
| TS Sekhon et al., [22] | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 0 | 15 | 20 | 0.75 |
| KP Nanaiah et al., [20] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 18 | 20 | 0.90 |
| D Goswami [21] | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 18 | 20 | 0.90 |
| A singh et al., [19] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 0 | 15 | 20 | 0.75 |
| D. Kundu et al., [18] | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 18 | 20 | 0.90 |
| Doifode VV et al., [17] | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 12 | 20 | 0.60 |
| Bansal M et al., [36] | 0 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 11 | 20 | 0.55 |
| S. Sanadhya et al., [38] | 0 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 11 | 20 | 0.55 |
| S fotedar et al., [37] | 0 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 11 | 20 | 0.55 |
| KP Peter et al., [39] | 0 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 11 | 20 | 0.55 |
The relationship between Age and Peridontal Disease: [Table/Fig-10] Shows the results of included studies assessing the relationship between Age and periodontal disease with their respective Community Periodontal Index of Treatment Needs (CPITN) Score .
CPITN score and age group of Included studies.
| Author | CPITN Score | Age Group | | Total |
|---|
| | 15 | 16 | 17 | 18 | | |
| KP, Nanaiah et al., [20] | 1 | 62 | 75 | 101 | 88 | | 326/1100 |
| 2 | 57 | 84 | 107 | 122 | | 370/1100 |
| 3 | 1 | 1 | 3 | 14 | | 19/1100 |
| 4 | 0 | 0 | 0 | 5 | | 5/1100 |
| Total | 120/193 | 160/221 | 211/333 | 229/353 | | |
| | 15-19 | 20-29 | 30-44 | 45-64 | 65 & above | |
| D Goswami [21] | 1 | 36 | 9 | 0 | 0 | 0 | 45/438 |
| 2 | 24 | 78 | 96 | 24 | 6 | 224/438 |
| 3 | 0 | 6 | 45 | 69 | 27 | 147/438 |
| 4 | 0 | 0 | 3 | 6 | 3 | 12/438 |
| Total | 60/66 | 93/93 | 144/144 | 99/99 | 36/36 | |
| | 15-19 | 20-29 | 30-44 | 45-64 | 65 & Above | |
| D kundu et al., [18] | 1 | 628 | 204 | 99 | 29 | 2 | 962/22452 |
| 2 | 2560 | 4787 | 5891 | 3511 | 505 | 17,254/22452 |
| 3 | 18 | 204 | 857 | 859 | 137 | 2,075/22452 |
| 4 | 14 | 69 | 330 | 479 | 81 | 973/22452 |
| Total | 3220/3948 | 5264/5503 | 7177/7296 | 4878/5008 | 725/787 | |
| | 25-33 | 36-45 | 46-55 | 56 & above | | |
| A Singh et al., [19] | 1 | 0 | 0 | 0 | 0 | | 0/1026 |
| 2 | 85 | 11 | 5 | 0 | | 101/1026 |
| 3 | 275 | 59 | 46 | 4 | | 384/1026 |
| 4 | 244 | 179 | 103 | 15 | | 541/1026 |
| Total | 604/604 | 249/249 | 159/159 | 19/19 | | |
| | 15-19 | 20-29 | 30-44 | 45-60 | 61 & Above | |
| TS Sekhon et al., [22] | 1 | 31 | 47 | 15 | 08 | 4 | 105/1680 |
| 2 | 46 | 148 | 169 | 33 | 26 | 422/1680 |
| 3 | 03 | 52 | 300 | 207 | 122 | 684/1680 |
| 4 | 01 | 13 | 100 | 91 | 136 | 341/1680 |
| Total | 81/116 | 260/300 | 584/617 | 339/349 | 288/298 | |
Discussion
The populations mostly studied in this systematic review had been taken from the field surveys and the hospital based studies were excluded so as to obtain a true prevalence of the periodontal disease in the studied survey population. Overall 31,757 individuals were examined through six included studies carried out in different parts of India [17–22]. The highest prevalence reported was found being 97.51% [18]. The two forms of periodontal disease i.e., chronic periodontitis and Aggressive periodontitis had not been separately assessed in five of the included studies. Both these entities exhibit different rate of disease progression and severity and should be assessed separately so as to provide strategic interventions accordingly. Only KP Nanaiah et al., [20] reported the prevalence of these two forms as 1.5 % and 0.36 % respectively.
We have used a quality assessment of the included studies to check the quality level of the studies taken into consideration and it was found that none of the study has scored ’1’. Thus it could be interpreted that none of the included study was of high quality. Future studies should be designed of high quality so as to reduce the bias and obtain the true prevalence rate.
On assessing the relationship of gender and periodontal disease, it was found that studies by Doifode et al., Kundu D et al., and TS Sekhon et al., have reported that periodontal disease was more common in males and the reason suggested being the deleterious oral habits which are more prevalent in male population [17,18,22].
Furthermore, when the relationship of age and periodontal disease was assessed it was observed that, in all the included studies it was seen that the severity of periodontal disease was increased with the advancing age [17–22]. These findings could be attributed to the general deterioration in immune function and tissue integrity in the older age that may increase the vulnerability to the periodontal disease.
India has a vast geographic area divided into different states, differing in cultural, socioeconomic, educational, and behavioral aspects. These factors significantly affect the oral health status of different regions [7]. Our result also confirmed the same findings. The included studies [17–22] emphasized on the role of cultural and social determinants like low socioeconomic status, low level of education and deleterious oral habits on high prevalence of periodontal disease.
It was found during our literature search that there were many parts in India where no studies have been carried out to judge the oral status of its residing population, these regions are mainly Northern, North Eastern and Eastern parts of India. Thus a nationwide multicentric studies are required to assess the true percent prevalence of periodontal disease affecting the Indian population.
Future Directions: Nationwide multicentric studies are required to assess the true prevalence rate of periodontal disease amongst the general population of India and interventions should be provided for the same to the affecting individuals so as to increase the quality of oral health life of the individuals. A proper study design should be formulated so as to assess the extent and severity of the disease in complete dentition.
Limitations
All the studies included used CPI or CPITN index as a means to observe the oral health status of the individuals. However, the use of CPITN for population surveillance has a limitation to be observed as a case definition for periodontitis. As it is a treatment need–based index, meant to find out the prevalence of persons requiring treatment. It does not give true prevalence rates in terms of severity and extent of the disease.
Also the recording of index teeth gives an underestimation of actual prevalence.
The case definitions proposed for population based surveillance of periodontitis either by Centre for Disease Control and Prevention (CDC)/American Academy of Periodontology(AAP) or European Federation of Periodontology (EFP) joint recommendations has not been taken into consideration in majority of the studies of these review [40].
Tooth loss or tooth mortality has not been assessed in any of the included studies as tooth loss could be a consequence of extent and severity of periodontal disease.
Conclusion
Due to non-availability of same age groups in selected studies an overall prevalence rate could not be obtained. However it was observed that few areas of states like west Bengal, Uttar Pradesh and Assam has reported a prevalence rate of periodontal disease of more than 85% in their general population. The results of this systematic review brings about the current alarming situation of periodontal health prevailing in this subcontinent and suggests a nationwide interventions for treating this disease. This task can be accomplished by more than 200 dental colleges spreading across the country, to reduce the early tooth loss and maintain the quality of oral health amongst each individuals.
CPITN – Community Periodontitis Index of Treatment Needs; CPI – Community Periodontal index, AP – Aggressive periodontitis, CP – Chronic Periodontiti
[1]. Fujita H, Periodontal diseases in the Jomon peoplesThe Journal of the Archaeological Society of Waseda University 1990 107:65-76. [Google Scholar]
[2]. Inoue N, Ching HK, Ito G, Kamegai T, Dental diseases in Japanese skeletal remains. II: Later Jomon periodJournal of the Anthropological Society of Nippon 1989 89(3):363-78. [Google Scholar]
[3]. World Health OrganizationOral Health Surveys: Basic Methods 1997 4th edGenevaWorld Health Organization [Google Scholar]
[4]. Petersen PE, The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century - The approach of the WHO Global Oral Health ProgrammeCommunity Dent Oral Epidemiol 2003 31(Suppl. 1):3-24. [Google Scholar]
[5]. World Health Organization. The WHO Global Oral Health Data Bank. Geneva: World Health Organization; 2003 [Google Scholar]
[6]. Government of India Ministry of Home affairs. http://censusindia.gov.in/ [Google Scholar]
[7]. Chandra Shekar BR, Raja Babu P, Cultural factors in health and oral healthIndian Journal of Dental Advancement 2009 1(1):24-30. [Google Scholar]
[8]. Marshall Day CD, Shourie KL, A roetgenographic survey of periodontal disease in IndiaJ. Am. Dent. Assoc 1949 39:572 [Google Scholar]
[9]. Mehta F, Baretto MA, Raut RB, Sanjana MK, Shourie KL, The incidence of periodontal disease amongst Indian adultsJ. All India Assoc 1953 2:4 [Google Scholar]
[10]. Sanjana MK, Mehta FS, Docto RH, Baretto MA, Mouth hygiene habits and their relation to periodontal diseaseJ Dent Res 1956 35:645-47. [Google Scholar]
[11]. Ramfjord SP, Emslie RD, Greene JC, Held AJ, Waerhaug J, Epidemiological studies of periodontal diseasesAm J Public Health Nations Health 1968 58:17-22. [Google Scholar]
[12]. Greene JC, Periodontal disease in India: report of an epidemiological studyJ Dent Res 1960 39:302-12. [Google Scholar]
[13]. Rao SS, Tewani SV, Prevalence of periodontosis among IndiansJ Periodontol 1968 39(1):27-34. [Google Scholar]
[14]. Anil S, Hari S, Vijayakumar T, Periodontal conditions of a selected population in Trivandrum District, KeralaIndia Community Dent Oral Epidemiol 1990 18(6):325 [Google Scholar]
[15]. Mathur B, Talwar C. India. New Delhi: Dental Council of India; 2004. National Oral Health Survey and Flouride Mapping 2002-2003 [Google Scholar]
[16]. Shah N. Oral and dental diseases: Causes, prevention and treatment strategies —Burden of Disease in India. National Commission on Macroeconomics and Health, Ministry of Health and Family Welfare. New Delhi: Government of India; Sep 2005; p 275–98 [Google Scholar]
[17]. Doifode VV, Ambadekar NN, Lanewar AG, Assessment of oral health status and its association with some epidemiological factors in population of Nagpur, IndiaIndian J Med Sci 2000 54:261-69. [Google Scholar]
[18]. Kundu D, Mehta R, Rozra S, Periodontal status of a given population of West Bengal: An epidemiological studyJ Indian SocPeriodontol 2011 15(2):126-29. [Google Scholar]
[19]. Singh A, Agarwal V, Tuli A, Khattak BP, Prevalence of chronic periodontitis in Meerut: A cross-sectional surveyJ Indian Soc Periodontol 2012 16:529-32. [Google Scholar]
[20]. Nanaiah KP, Nagarathna DV, Manjunath N, Prevalence of periodontitis among the adolescents aged 15-18 years in Mangalore City: an epidemiological and microbiological studyJ Indian SocPeriodontol 2013 17(6):784-89. [Google Scholar]
[21]. Goswami D, Periodontal treatment needs of a rural population of North East IndiaThe Clarion 2014 3(1):8-12. [Google Scholar]
[22]. Sekhon TS, Grewal S, Gambhir RS, Periodontal health status and treatment needs of the rural population of India: a cross-sectional studyJ Nat SciBiol Med 2015 6(1):111-15. [Google Scholar]
[23]. Rekha R, Hiremath SS, Oral health status and treatment requirments of confectionery workers in Bangalore city. A comparative studyIndian J Dent Res 2002 13(3-4):161-65. [Google Scholar]
[24]. Jain M, Mathur A, Kumar S, Duraiswamy P, Kulkarni S, Oral hygiene and periodontal status among Terapanthi Svetambar Jain monks in IndiaBraz Oral Res 2009 23(4):370-76. [Google Scholar]
[25]. Chandra Shekar BR, Reddy C, Oral health status in relation to socioeconomic factors among the municipal employees of Mysore cityIndian J Dent Res 2011 22(3):410-18. [Google Scholar]
[26]. Agrawal A, Bhat N, Shetty S, Sharda A, Singh K, Chaudhary H, Oral hygiene and periodontal status among detainees in a juvenile detention center, IndiaOral Health Prev Dent 2011 9(3):281-87. [Google Scholar]
[27]. Reddy V, Kondareddy CV, Siddanna S, Manjunath M, A survey on oral health status and treatment needs of life-imprisoned inmates in central jails of Karnataka, IndiaInt Dent J 2012 62(1):27-32. [Google Scholar]
[28]. Nagarajappa R, Sanadhya S, Sharda AJ, Asawa K, Tak M, Batra M, Assessment of the periodontal status among kota stone workers in Jhalawar, IndiaJ Clin Diagn Res 2013 7(7):1498-503. [Google Scholar]
[29]. Kadanakuppe S, Bhat PK, Oral health status and treatment needs of Iruligas at Ramanagara District, Karnataka, IndiaWest Indian Med J 2013 62(1):73-80. [Google Scholar]
[30]. Sanadhya S, Nagarajappa R, Sharda AJ, Asawa K, Tak M, Batra M, The oral health status and the treatment needs of salt workers at sambhar lake, Jaipur, IndiaJ Clin Diagn Res 2013 7(8):1782-86. [Google Scholar]
[31]. Gambhir RS, Sogi GM, Veeresha KL, Sohi RK, Randhawa A, Kakar H, Dental health status and treatment needs of transport workers of a northern Indian city: a cross-sectional studyJ Nat Sci Biol Med 2013 4(2):451-56. [Google Scholar]
[32]. Dayakar MM, Shivprasad D, Pai PG, Assessment of periodontal health status among prison inmates: A cross-sectional surveyJ Indian Soc Periodontol 2014 18(1):74-77. [Google Scholar]
[33]. Torwane NA, Hongal S, Saxena E, Rana PT, Jain S, Gouraha A, Assessment of periodontal status among eunuchs residing in Bhopal city, Madhya Pradesh, India: a cross-sectional studyOral Health Dent Manag 2014 13(3):628-33. [Google Scholar]
[34]. Solanki J, Gupta S, Chand S, Oral health of stone mine workers of Jodhpur city, Rajasthan, IndiaSaf Health Work 2014 5(3):136-39. [Google Scholar]
[35]. Aapaliya P, Shinde K, Deswal AK, Mohapatra S, Saleem S, Mangal R, Assessment of oral health among seafarers in Mundra Port, Kutch, Gujarat: a cross-sectional studyInt Marit Health 2015 66(1):11-17. [Google Scholar]
[36]. Bansal M, Mittal N, Singh TB, Assessment of the prevalence of periodontal diseases and treatment needs: a hospital-based studyJ Indian Soc Periodontol 2015 19(2):211-15. [Google Scholar]
[37]. Fotedar S, Sharma KP, Fotedar V, Bhardwaj V, Chauhan A, Manchanda K, Relationship between oral health status and oral health related quality of life in adults attending H.P government dental college, Shimla, Himachal Pradesh, IndiaOral Health Dent Mang 2014 13(3):661-65. [Google Scholar]
[38]. Sanadhya S, Aapaliya P, Jain S, Sharma N, Choudhary G, Dobaria N, Assessment and comparison of clinical dental status and its impact on oral health-related quality of life among rural and urban adults of Udaipur, India: a cross-sectional studyJ Basic Clin Pharma 2015 6:50-58. [Google Scholar]
[39]. Peter KP, Mute BR, Pitale UM, Shetty S, Shashikiran HC, Satpute PS, Prevalence of periodontal disease and characterization of its extent and severity in an adult population – an observational studyJ Clin Diagn Res 2014 8(12):ZC04-07. [Google Scholar]
[40]. Paul I. Eke, Roy C. Page, Liang Wei, Gina Thornton-Evans, Robert J. Genco, Update of the case definitions for population-based surveillance of periodontitisJ Periodontol 2012 83:1449-54. [Google Scholar]