An Accelerated Multi-Modality Rehabilitation Protocol Combined with Botulinum Toxin-A Injection in Adult Idiopathic Toe Walking: Case Report
Sibel Kibar1, Ferdi Yavuz2, Birol Balaban3
1 The Clinic of Physical Therapy and Rehabilitation, FizyoCare Medical Center, Ankara, Turkey.
2 Assistant Doctor, Department of Anatomy, Ankara University School of Medicine, Ankara, Turkey.
3 Professor, Department of Physical Therapy and Rehabilitation, European University of Lefke Faculty of Health Sciences, Lefke, North Cyprus.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sibel Kibar, The Clinic of Physical Therapy and Rehabilitation, FizyoCare Medical Center, Alacaatlı Caddesi, 2857. Sokak, No:7, Çayyolu, 06810 Ankara, Turkey.
E-mail: sibelkbr@gmail.com
Diagnosis of Adult Idiopathic Toe Walking (AITW) is very rare in clinical practice. High quality studies regarding AITW and its treatment options have not been conducted previously. A 28-year-old male patient complaining of lower leg pain was referred to outpatient rehabilitation clinic. Physical examination revealed a gait abnormality of insufficient heel strike at initial contact. The aetiology was investigated and the patient’s walking parameters were assessed using a computerized gait analysis system. The AITW was diagnosed. Botulinum toxin-A (Dysport®) was injected to the bilateral gastrocnemius muscles. A combined 10-days rehabilitation program was designed, including a daily one-hour physiotherapist supervised exercise program, ankle dorsiflexion exercises using an EMG-biofeedback unit assisted virtual rehabilitation system (Biometrics) and virtual gait training (Rehawalk) every other day. After treatment, the patient was able to heel strike at the initiation of the stance phase of the gait. Ankle dorsiflexion range of motions increased. The most prominent improvement was seen in maximum pressure and heel force. In addition center of pressure evaluations were also improved. To the best of our knowledge this is the first case, of AITW treated with combined botulinum toxin, exercise and virtual rehabilitation systems. This short report demonstrates the rapid effect of this 10-days combined therapy.
Virtual, 3D, Gait training
Case Report
A 28-year-old male patient complaining of lower leg pain for three months was referred to outpatient rehabilitation clinic. The height of the patient was 184cm, and the patient’s weight was 91 kg (body mass index- weight (kg)/height (m)2= 26.87). The leg length was measured with a tape measure and it was 108cm (umbilicus to medial malleolus), no difference was found between two legs’ lengths. Thorough physical examination revealed a gait abnormality of insufficient heel strike at initial contact during high-speed walking. Active and passive ankle dorsiflexion Range Of Motion (ROM) was measured using an electrogoniometer (Biometrics- E-link system). Dorsiflexion ROM for the right and left ankles were 5 and 0 degrees, respectively. Neurological physical examination was normal. Cranial and cervical, thoracic and lumbar vertebral magnetic resonance imaging’s were normal. Laboratory parameters (myopathy and rheumatism disorder parameters, etc.) were also in the normal range. The patient’s walking parameters were assessed using a computerized gait analysis (Rehawalk Gait Analysis System). Diagnosis of AITW was made.
Botulinum toxin-A (Dysport®) was injected to the bilateral gastrocnemius muscles (500U left and 200U right). A combined rehabilitation program was designed, including a daily one-hour physiotherapist supervised exercise program (10-sessions), 40 minutes of active ankle dorsiflexion exercises using an EMG-biofeedback unit assisted virtual rehabilitation system (Biometrics, E-link) (5-sessions) and 40-minutes virtual gait training (Rehawalk) (5-sessions) every other day. The one-hour physiotherapy program consisted of stretching exercises of the gastrocsoleus and hamstring muscles, ambulation training focusing on heel strike, bilateral weight bearing, and balance exercises.
A computerized evaluation and exercise device was used for virtual rehabilitation-assisted ankle dorsiflexion exercises. The device includes modules matched with a computer system for range of motion and muscle strengthening exercises. Maximum forced ROM and muscle contraction activity were measured. Ankle dorsiflexion was forced through training of tibialis anterior muscle contraction. The training program was applied using an EMG-biofeedback unit matched with a computer system. This unit was attached at the thickest part of the tibialis anterior muscle near to the proximal one third of the tibia. The patient was then instructed to practice ankle dorsiflexion with the assistance of the proper games chosen for the virtual rehabilitation, as these computer games stimulate the patient’s attention and encourage more careful participation in the exercise programs.
A 3D gait training was applied using a computerized system designed for gait analysis and treatment in walking disorders. The system works with a treadmill and projector that provides visual cueing by projecting optimal gait patterns or target gait patters that determined by the physician due to patient’s gait abnormality (step-by-step) on the treadmill. This visual cueing on the treadmill produces a visual feedback during treatment. In addition, a large monitor positioned in front of the treadmill allows for simultaneous virtual feedback training in a 3-D virtual walking environment which contains some obstacles and cognitive questions that stimulate the patients’ motor and mental activity.
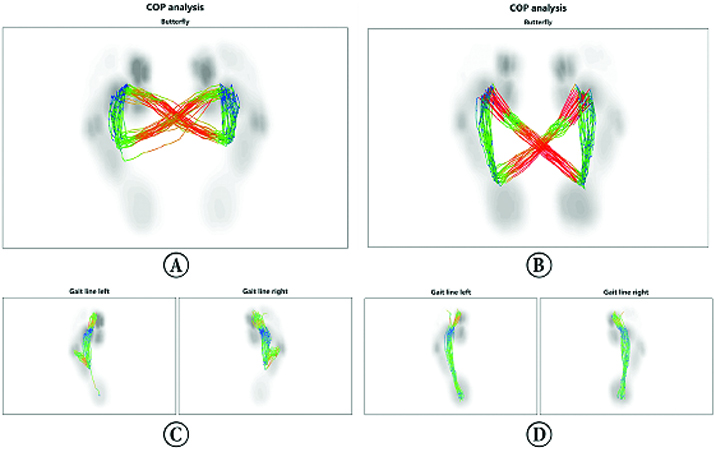
While the patient’s passive ankle dorsiflexion ROM increased by 10 degrees and 7 degrees in the right and left ankle respectively, active ROM of the swing phase in the gait analysis increased by 20 degrees and 10 degrees [Table/Fig-1]. The most prominent improvement was seen in walking parameters, especially maximum pressure and heel force. The improvements of walking parameters are demonstrated in [Table/Fig-2]. Center of pressure evaluations (gait lines and butterfly) were also improved and showed in [Table/Fig-3].
Active ankle dorsiflexion range of motion of the swing phase in the gait analysis. A and C pretreatment measurements, B and D posttreatment measurements.

Pressure distribution before rehabilitation; A, after rehabilitation;B. Backfoot and forefoot forces before rehabilitation; C, after rehabilitation; D.

Center of pressure analysis before rehabilitation; A and C, after rehabilitation; B and D.
Discussion
Toe walking is a gait pattern sometimes seen in developing children under two years of age during the learning of a normal gait [1]. Children who walk on the toes do not produce a heel strike throughout the initial contact phase [1]. This abnormal gait pattern is usually replaced with normal gait at the end of the independent walking practice period. Nonetheless, toe walking cannot be changed in some children. Toe walking without any medical condition in children older than three years old is called idiopathic (habitual) toe walking [2]. Previously, only two cases of adult patients with ITW were reported in the literature, one of which demonstrated the effect of visual feedback training on adult idiopathic toe walking (AITW) [3,4]. No controlled study has been conducted regarding the treatment of AITW in the literature. This case report aimed to present the results of the accelerated multi-modality rehabilitation of EMG-biofeedback assisted virtual rehabilitation and three dimensional (3D) gait training combined with botulinum toxin injection in AITW.
Accurate prevalence and incidence ratios of AITW have not yet been reported. In a study of 14 patients aged between 14 and 27 years with a 20-year follow-up period, only one patient with ITW did not gain normal gait pattern [5]. No consensus has been formed on ITW treatment methods and follow-up parameters. Furthermore, some investigators have reported ITW as a cosmetic problem that can be followed by a physician without treatment [6]. However, the primary complaint of the present patient and the other two AITW patients in the literature was leg pain [3,4]. Development of secondary pes planovalgus, leg pain, limbing and fatigue related with ITW has been previously reported [2]. We think that toe walking should be treated in order to gain a normal gait pattern and decrease the excessive energy expenditure during walking that may damage the joints and muscles [7].
Studies regarding treatment of ITW have emphasized the injection of botulinum toxin, casting and lengthening surgeries [2,6]. A recent review concerning ITW treatment methods reported that complete improvement was not demonstrated despite the effectiveness of surgery and serial casting in gait kinetics [2]. Botulinum toxin-A has no additive effect on the results of casting. The most effective treatment modality reported was surgery. Exercise programs were added to these modalities in a few studies [2]. The effectiveness of only physical therapy treatment in patients with ITW was evaluated in one case series of five patients [8]. Increased passive ankle ROM was demonstrated following a 9-week exercise program performed in two one-hour sessions per week. In another case series in which botulinum toxin was applied followed by 20 sessions of physical therapy (two times per week), patients demonstrated a more normal strike pattern after 12 month follow-up period and the authors reported the effectiveness of botulinum toxin injection [9]. Studies conducted with botulinum toxin, casting, and surgery without regular exercise programs demonstrated no persistent effects on gait parameters and ankle dorsiflexion [2,6].
In the present study, marked improvements in gait parameters were determined in a very short time of ten days due to the botulinum toxin injection followed by intense physical therapy combined with virtual rehabilitation systems. The patient’s gastrocnemius muscles were very rigid and short. The botulinum toxin injection resulted in easier relaxing and stretching of the muscles and thus increased the effectiveness of the exercises. Botulinum toxin treatment without exercise therapy was not found to be sufficiently effective in patients with ITW in previous studies [2]. Therefore, we believe that an important overlooked subject in those treatment programs is the inclusion of personalized exercise programs. Despite the adult age of our patient, a proper dose of botulinum toxin injection combined with intense accelerated exercise program achieved the cessation of the toe walking pattern.
[1]. Sutherland DH, Olshen R, Cooper L, Woo SL, The development of mature gaitJ Bone Joint Surg Am 1980 62:336-53. [Google Scholar]
[2]. van Kuijk AA, Kosters R, Vugts M, Geurts AC, Treatment for idiopathic toe walking: a systematic review of the literatureJ Rehabil Med 2014 46:945-57. [Google Scholar]
[3]. Pelykh O, Klein AM, Feist-Pagenstert I, Schlick C, Ilmberger J, Treatment outcome of visual feedback training in an adult patient with habitual toe walkingEur J Phys Rehabil Med 2014 Oct 9 ahead of print [Google Scholar]
[4]. Pomarino D, Kühl A, Kühl F, Pomarino A. Case history and successful therapy of a toe walking 23-years old man. PDF presentation, December 2006. Available at http://www.zehenspitzengang.de/therapy_toe_walking.pdf. Accessed December 10,2015 [Google Scholar]
[5]. Hirsch G, Wagner B, The natural history of idiopathic toe-walking: a long-term follow-up of fourteen conservatively treated childrenActa Paediatr 2004 93:196-99. [Google Scholar]
[6]. Dietz F, Khunsree S, Idiopathic toe walking: to treat or not to treat, that is the questionIowa Orthop J 2012 32:184-88. [Google Scholar]
[7]. Peggy A Houglum, Dolores B, Functionla Activities, Stance and Gait. In Brown B, Aaron M (ed)Brunnstrom’s Clinical Kinesiology 2012 6th ednPhyledelphiaE.A. Davis Company:568 [Google Scholar]
[8]. Clark E, Sweeney JK, Yocum A, McCoy SW, Effects of motor control intervention for children with idiopathic toe walking: a 5-case seriesPediatr Phys Ther 2010 22:417-26. [Google Scholar]
[9]. Brunt D, Woo R, Kim HD, Ko MS, Senesac C, Li S, Effect of botulinum toxin type A on gait of children who are idiopathic toe-walkersJ Surg Orthop Adv 2004 13:149-55. [Google Scholar]