Intracranial tuberculoma may occur in intra-axial or extra-axial locations, but is frequently located intraparenchymally in the brain [1–3]. En-plaque tuberculoma is a rare form of central nervous system tuberculoma and may mimic meningioma on imaging [2]. It results from hematogenous spread of infection to the dura, or confinement of the leptomeningeal tubercles (without rupturing into the subarachnoid space forming a Rich’s foci as occurs usually) to the meninges forming a hard fibrous mass attached to the dura [1–3]. Literature review regarding this entity is sparse and even among earlier reports, majority have described Computed Tomography (CT) findings. There are very few case reports addressing the Magnetic Resonance Imaging (MRI) diagnosis of en-plaque tuberculoma [4–8].
In this paper, we describe the profile of a cohort of eight patients in whom the diagnosis of en-plaque tuberculoma was made on the basis of Magnetic Resonance Imaging (MRI) findings and subsequently confirmed by Polymerase Chain Reaction (PCR) assay of cerebrospinal fluid (CSF) for Mycobacterium tuberculosis.
Materials and Methods
This is a descriptive paper about the clinical presentation and radiological observations in a cohort of eight patients in whom a diagnosis of en-plaque tuberculoma was made based on the MRI brain and subsequently confirmed by Polymerase Chain Reaction (PCR) assay of Cerebrospinal Fluid (CSF) for Mycobacterium tuberculosis. The patients were seen at the Neurology Department of Victoria and Bowring Hospitals, attached to Bangalore Medical College and Research Institute, Bangalore during a period from March 2010 to March 2016. Written informed consent was obtained from all the patients. A detailed clinical history and complete examination (general physical, neurological and other systemic) was carried out in all the patients. All patients underwent haematological and blood biochemical tests, chest X-ray, MRI brain and CSF examinations.
Results
A total of eight adult patients (two women and six men) with an MRI diagnosis of en-plaque tuberculoma were seen. It was intriguing to note that none of the patients had past history of tuberculosis or history of contact. The systemic examination including the respiratory system, cardiovascular system and per abdomen examination were normal in all. Investigations revealed normal haemogram, urine analysis, blood glucose, serum creatinine and liver function tests in all the patients and HIV I and II were negative in all. Chest X-ray was normal in all the patients. Mantoux test was negative in all.
All patients were investigated with MRI brain (T1W, T2W, FLAIR sequences, gradient echo, Gadolinium contrast and MR Venogram). All patients demonstrated extra axial dural based lesions and none had cerebral ooedema, parenchymal lesions, mass effect or midline shift. None except one had mild hydrocephalus. None exhibited blooming and only one demonstrated mild narrowing with irregular margins of mid third of superior sagittal sinus adjacent to the lesion on MR venogram [Table/Fig-1]. Dural based thick sheet like lesion in bilateral corresponding regions was noted in two patients and the rest six had unilateral lesions. The lesion extended along falx cerebri [Table/Fig-2] in one patient and along tentorium cerebelli in another patient. The notable feature on MRI is its plaque-like extension in the meninges together with marked nodular enhancement on contrast administration [4]. Various patterns of enhancement were noted in our patients: thin peripheral (n=3), homogenous (n=3), varied enhancement (n=1) and open ring enhancement (n=1). The detailed MRI findings in all 8 patients are depicted in [Table/Fig-3].
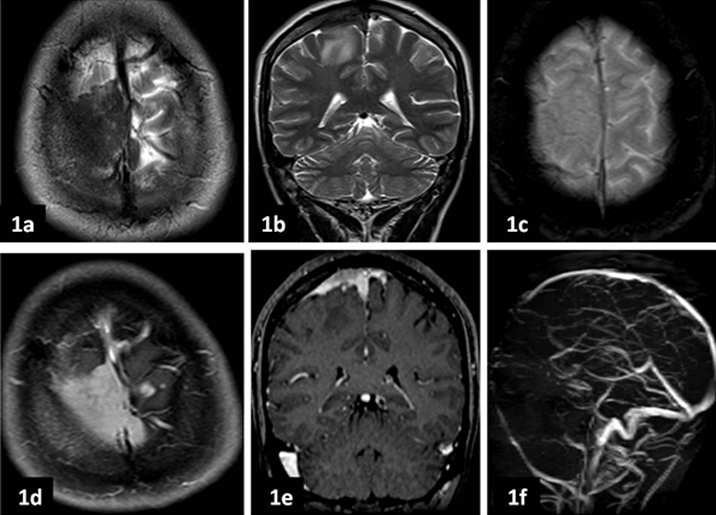
a, b. Axial and coronal T2 weighted images show extra axial dural based plaque like hypointense lesion along meninges in right high frontal region. c. Axial Gradient image at this level shows no blooming in the centre or periphery to suggest haemorrhagic foci. d, e. Post contrast axial and coronal T1 weighted images show moderate homogenous enhancement of the lesion suggesting absent caseation necrosis within the lesion. f. Non contrast MR venogram shows mild narrowing with irregular margins of mid third of superior sagittal sinus adjacent to the lesion.
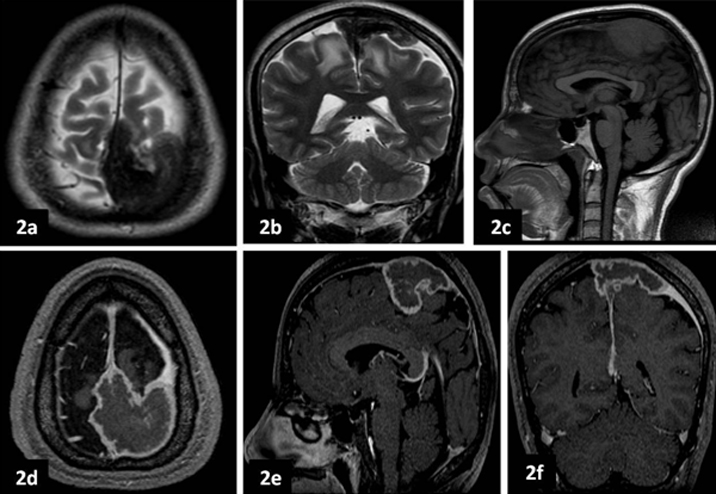
a, b. Axial and coronal T2 weighted images show dural based thick sheet like hypointense lesion in bilateral high fronto-parietal regions (left >right) along falx cerebri and extending along convexity meninges. c. Sagittal T1 weighted image shows well defined isointense lesion along mid third of falx cerebri. d, e, f. Post contrast axial, sagittal and coronal T1 weighted images show thin rim of peripheral enhancement of the lesion with central non enhancing necrotic areas.
MRI Brain – characteristics of the lesions in the patients.
| Patient | Lesion location | T1W Image | T2W Image | FLAIR sequence | MR Contrast | Blooming if any | MR Venogram |
|---|
| 1 [Table/Fig-1] | Extra axial dural based plaque like lesion along the meninges in right high frontal region | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Moderate homogenous enhancement suggesting absent caseation necrosis within the lesion | No blooming in the centre or periphery | Mild narrowing with irregular margins of mid third of superior sagittal sinus adjacent to the lesion |
| 2 | Dural based plaque like lesion along the meninges in right frontoparietal region | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Thin peripheral enhancement noted | No blooming in the centre or periphery | Normal |
| 3 | Dural based plaque like lesion along the meninges in left high frontal region | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Thin rim of peripheral enhancement noted | No blooming in the centre or periphery | Normal |
| 4 | Dural based plaque like lesion along the meninges in right frontopaietal region | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Moderate homogenous enhancement | No blooming in the centre or periphery | Normal |
| 5 [Table/Fig-2] | Dural based thick sheet like lesion in bilateral high fronto-parietal regions (left >right) along falx cerebri and extending along convexity meninges | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Thin rim of peripheral enhancement of the lesion with central non enhancing necrotic areas | No blooming in the centre or periphery | Normal |
| 6 | Dural based plaque like lesion along the meninges in bilateral high frontal regions | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Varied Peripheral enhancement noted | No blooming in the centre or periphery | Normal |
| 7 | Dural based plaque like lesion along the meninges in left parietal region; mild hydrocephalus noted | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Open ring peripheral enhancement noted | No blooming in the centre or periphery | Normal |
| 8 | Dural based plaque like lesion along the meninges in right parieto-occipital region and extension on to tentorium cerebella | Isointense | Hypointense | Central Hypointense with peripheral hyperintensity | Homogenous Peripheral enhancement noted | No blooming in the centre or periphery | Normal |
All patients were admitted and underwent CSF examination. All demonstrated mild to moderately raised protein content with lymphocytic pleocytosis. CSF gram’s stain, acid-fast staining and India ink preparation were negative in all. CSF culture and enzyme-linked immunosorbent assay for Mycobacterium tuberculosis were negative in all 8 patients. CSF PCR was positive for Mycobacterium tuberculosis DNA in all. [Table/Fig-4] depicts the CSF findings of all the patients along with their clinic-demographic profile and other relevant laboratory results.
Clinical characteristics and laboratory findings of the patients.
| Patient | Age/sex | Presenting Symtoms | Symptom duration | Neurologic deficits | Meningeal signs | ESR | CSF |
|---|
| 1 | 28 years/ Male | Bifrontal headache and vomiting | 4 months | Mild papilloedema in both eyes | nil | 15 mm/hr | Protein – 86 mg/dl; sugar – 66 mg/dl and 100 lymphocytes/ cumm. |
| 2 | 36 years/ Male | Holocranial dull aching intermittent headache associated with infrequent vomitings. | 6 months; worsening of headache accompanied by blurring of vision for both near and far objects since 1week | Bilateral papilloedema | Terminal neck stiffness present; Kernig’s sign - negative | 24 mm/hr | Protein – 50 mg/dl; sugar – 74 mg/dl; 44 lymphocytes /cumm. |
| 3 | 42 years/ Male | Dull headache and myalgia | 3 months; worsening headache with vomiting since 1 week | Mild gait ataxia | Neck stiffness present; Kernig’s sign - negative | 36 mm/hr | Protein – 60 mg/dl; sugar – 64 mg/dl; 48 lymphocytes /cumm |
| 4 | 20 years/ Female | Headache, vomiting, | 1 month; binocular diplopia for far objects since 3 days | Bilateral papilloedema and right sixth nerve palsy | Nil | 38 mm/hr | Protein – 76 mg/dl; sugar – 40 mg/dl; 40 lymphocytes /cumm |
| 5 | 38 years/ Male | Dull holocranial headache with nausea | 2 months | Bilateral papilloedema | Neck stiffness present; Kernig’s sign - negative | 68 mm/hr | Protein – 60 mg/dl; sugar – 54 mg/dl; 36 lymphocytes /cumm |
| 6 | 40 years/ Female | Moderately severe bifrontal and bitemporal Headache | 1 month; drowsiness since 2 days | Drowsy, but arousable patient with Brisk deep tendon reflexes and extensor plantars | Neck stiffness present; Kernig’s sign – positive | 44 mm/hr | Protein – 74 mg/dl; sugar – 56 mg/dl; 52 lymphocytes /cumm |
| 7 | 48 years/ Male | Dull holocranial headache | 6 weeks | Bilateral papilloedema | Nil | 50 mm/hr | Protein – 80 mg/dl; sugar – 60 mg/dl; 88 lymphocytes /cumm |
| 8 | 39 years/ Male | Occipitonuchal pain | 2 months; worsened headache with vomiting since 1 week | Nil | Neck stiffness and Kernig’s sign – positive | 38 mm/hr | Protein – 75 mg/dl; sugar – 61 mg/dl; 55 lymphocytes /cumm |
Based on the CSF PCR result, the patients were treated with 4 drug antitubercular treatment (ATT), i.e., isoniazid (300mg), rifampin (450mg), pyrazinamide (1,500mg), and ethambutol (800mg), in combination with tapering doses of steroids for 4 weeks. The patients showed steady improvement in clinical status with subsidence of headache and amelioration of symptoms at the time of discharge after about 2 weeks of hospital stay. Two months later, ethambutol and pyrazinamide were withdrawn; the other two antitubercular drugs were continued for a period of 1 year.
A repeat MRI study performed after 6 months of initiation of ATT in 5 patients showed disappearance of the lesion as well as of the meningeal enhancement. One patient was lost to follow-up and two did not give consent for follow-up MRI as they had improved symptomatically.
Discussion
The pathologic presentation of central nervous system tuberculosis is varied with meningeal involvement (pachymeningitis being the most common) and/ or intraparenchymal tuberculomas [1–3,9,10]. En-plaque tuberculoma is an extremely rare presentation of intracranial tuberculosis [2,3,9,10]. The fact that we have seen only eight such cases over six years as described in the present paper reiterates its rarity. Literature search reveals only isolated case reports of this entity. In fact, eight patients is not so less a number over six years and this degree of pickup rate cannot be dismissed as chance or coincidence and may be attributed to the fact that our institute is a tertiary referral centre for various neurological ailments and is equipped with good MRI facility. This might be one of the reasons for picking up such a rare entity and the other reason being we becoming wiser about this entity after diagnosing first few cases!
Pardee and Knox were the first to describe this entity in 1927 by as plaque like meningitic process without exudation, usually in the frontal and the parietal region [3,9]. Macroscopically, it has been described as a localized plaque-like lesion, globular or irregular in outline, very solid without calcified or caseous areas and situated deep in a sulcus in relation to the meninges [4,6,9,10]. It is considered to be a likely source of diffuse meningitis and is the result of bacillaemia that occurs during the development of the primary lesion or after primary progressive infection [1,3,9].
Review of literature reveals that en-plaque tuberculoma is usually seen in adults and characterized by a lengthy clinical course [9,10]. The clinical features depend on the location and include variable presence of headache, visual blurring, vomiting, focal seizures, limb weakness and neck tilt [9]. So broadly, the clinical presentation could be either of: a) raised intracranial pressure with or without localizing neurological signs; or b) progressive neurological disability in the absence of elevated intracranial pressure [2,9–12]. Fever was usually present and optic fundi were usually normal [9,12]. In contrast to their description, none of our patients had fever and five patients had symptoms of increased intracranial pressure along with papilloedema.
The exact location of en-plaque tuberculoma is described to be variable including frontal and parietal convexity, interhemispheric fissure, tentorium cerebelli and posterior fossa [4,6,7–9]. It is a great mimicker and simulates numerous dural-based lesions including benign to malignant neoplasms like meningioma, lymphoma and metastatic deposits, infections like empyema, arterio-venous malformations, granulomatous conditions like sarcoidosis. Though most of the times, the characteristic MRI features of en-plaque tuberculoma might aid in distinguishing these conditions, a preoperative diagnosis is essential to differentiate it from neoplastic lesions at least, which are usually amenable to surgical intervention in contrast to tuberculomas, which need only optimal chemotherapy in majority of the cases [2,4–7,9,10,13,14].
In our patients, like those described by Pardee and Knox [3] the lesions were located in the frontal and parietal regions. Dural based thick sheet like lesion in bilateral corresponding regions was noted in two patients and the rest six had unilateral lesions. All but one patient had lesions located in the supratentorial compartment; one had lesion extending along the tentorium cerebelli.
The notable feature on MRI is its plaque-like extension in the meninges together with marked nodular enhancement on contrast administration [4–8]. Various patterns of enhancement were noted in our patients: thin peripheral (n=3), homogenous (n=3), varied enhancement (n=1) and open ring enhancement (n=1). Gd-DTPA enhanced MRI has been shown to be superior in cases of meningeal tuberculosis by Chang et al., [5], which however was not done in our patients.
Though it is possible to diagnose en-plaque tuberculoma based on MRI characteristics like those described in our patients, in order to increase the confidence in the diagnosis of tuberculosis, confirmation by demonstration of acid-fast bacilli or caseating granuloma or demonstration of Mycobacterium tuberculosis DNA by CSF - PCR is desirable [15]. PCR assay is a sensitive test for detection of Mycobacterium tuberculosis DNA in CSF that may be both smear negative and culture negative and this has been well proven earlier [15]. In our patients the diagnosis was confirmed by the positive PCR results for Mycobacterium tuberculosis. While MRI provides an understanding of the topography of the lesion, PCR helps in establishing the diagnosis of tuberculosis as in our patients [15]. The patients also demonstrated good response to ATT, and this was reflected in the repeat MRI studies performed after treatment.
Limitation
This paper is strengthened by the number of patients seen with such a rare entity, though spread over a considerable study period. The limitations could be that Gd-DTPA enhanced MRI which is shown to be superior in such cases could not be done in our patients due to practical constraints. Another limitation could be a lack of meningeal biopsy and histopathology confirmation. However, the patients had positive PCR results for Mycobacterium tuberculosis and improved clinically with ATT and most of them had a follow-up MRI that showed disappearance of lesions after treatment which proves the point.
Conclusion
Awareness about en-plaque tuberculomas can heighten the index of suspicion and can thus prevent aggressive surgical resections and thereby reduce mortality and morbidity. MRI brain and CSF PCR assay for Mycobacterium tuberculosis are complimentary for timely diagnosis and treatment. This paper comprehensively depicts the clinico-radiological features in such patients and may serve not to miss this uncommon manifestation of a common central nervous system infection. A good clinical history, high index of suspicion and knowledge of the differentiating MRI features help in a proper timely diagnosis and optimal patient treatment.