Resistant Hypertension due to Fibromuscular Dysplasia in a Young Male: A Rare Case Report
Hossein Vakili1, Isa Khaheshi2, Mehdi Memaryan3, Roxana Sadeghi4, Mohammadreza Naderian5
1 Associate Professor, Department of Cardiology, Cardiovascular Research Center, Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2 Assistant Professor, Department of Cardiology, Cardiovascular Research Center, Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3 Resident of Cardiology, Department of Cardiology, Cardiovascular Research Center, Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4 Associate Professor, Department of Cardiology, Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5 Non-Communicable Diseases Research Center, Endocrinology and Metabolism Population Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran, Students’ Scientific Research Center (SSRC), Tehran University of Medical Sciences, Tehran, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Isa Khaheshi, Assistant Professor, Cardiovascular Research Center, Department of Cardiology, Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Modarres Hospital, Kaj sq., Sa’adat Abad, Tehran, Iran.
E-mail: isa.khaheshi@gmail.com, isa_khaheshi@yahoo.com
Fibromuscular Dysplasia (FMD) is a sporadic non-atherosclerotic disease. FMD has been established in nearly every arterial bed. However, the most frequent arteries affected are the renal and carotid arteries. Disease presentation may vary broadly, depending upon the arterial bed complication and the severity of illness. Hypertension, particularly resistant type, headache and dizziness are the most common presentations. String of beads appearance in angiographic views due to post-stenotic aneurysms is the characteristic view. It is most commonly described in young aged females; but in rare male cases has also been reported. Moreover, balloon angioplasty is standard and effective therapy for FMD. We present a young 28-year-old man who was referred for evaluation of resistant hypertension for nearly 3 years without comprehensive workup. The patient underwent renal artery angiography which confirmed beading narrowing of the right renal artery with significant stenosis at mid portion compatible with FMD; and balloon angioplasty was done. This case highlights that FMD should be kept in mind as a rare cause of resistant hypertension in young males; although it is most common in young females.
Angiography, Beading narrowing, Renal artery stenosis
Case Report
A 28-year-old previously healthy man was referred to our hospital for evaluation of resistant hypertension. He had no remarkable medical history or family background. He had uncontrolled hypertension for nearly 3 years without comprehensive work-up. Physical examination revealed resistant hypertension with Blood Pressure (BP) of 165/100 mmHg in right and 170/110 mmHg in left arm. He had a regular pulse rate of 76/min. The rest of his physical examination had no significant finding. No bruit was auscultated in abdomen examination and bilateral pulses in upper and lower extremities were all symmetric and well-palpable. Fundoscopic examination of retina revealed no major abnormalities.
His blood pressure was uncontrolled despite the use of 50mg of Metoprolol twice a day, 50mg of Captopril three times a day, 10mg Amlodipine daily and 25mg of Hydrochlorothiazide daily.
His ECG demonstrated normal sinus rhythm with strain pattern in leads I and aVL consistent with LVH. Transthoracic echocardiography showed normal ejection fraction of 60%, mild LVH and grade 1 diastolic dysfunction.
Laboratory data included complete blood count, serum electrolytes, thyroid, renal and hepatic function tests, urine analysis, urine Vanillylmandelic Acid (VMA), serum renin and aldosterone level were all within normal limits.
Doppler study of renal arteries revealed significant stenosis of the right renal artery (right renal artery index (RI) =0.4). The patient underwent renal artery angiography which confirmed beading narrowing of the right renal with significant stenosis at mid portion compatible with fibromuscular dysplasia [Table/Fig-1a].
Selective angiography of right renal artery which showed beading narrowing of the right renal with significant stenosis at mid portion compatible with fibromuscular dysplasia. Final result of balloon angioplasty of right renal artery with NC Trek balloon.
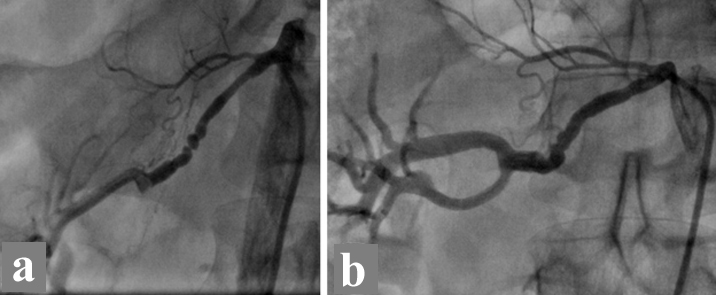
According to resistant hypertension on four antihypertensive drugs, the decision was made to proceed with percutaneous intervention. After wiring of right renal artery with Sionblue wire, balloon angioplasty with NC Trek balloon (3-20 mm) and NC Trek balloon (4-15 mm) at mid portion and NC Trek balloon (4-12 mm) at proximal portion was performed [Table/Fig-1b].
The patient was treated with antiplatelet therapy (Aspirin 81mg and Clopidogrel 75mg daily) for one month. He was well with post angioplasty-evaluations with improvement of his resistant hypertension. In follow-up visits (1,3 and 6 months later) his blood pressure remained in normal range of 115/70 mmHg to 125/75 mmHg without any need for antihypertensive drugs and he had no substantial complaint. An informed consent was signed by the patient.
Discussion
Atherosclerotic Renal Artery Stenosis (RAS) and Fibromuscular Dysplasia (FMD) are the most prevalent diseases of the renal arteries that can result in resistant hypertension [1]. Fibromuscular Dysplasia (FMD) is an infrequent non-atherosclerotic disease that usually leads to stenosis of the renal and carotid arteries. It is defined as a string of beads appearance in angiographic views due to post-stenotic aneurysms and most commonly described in young aged females [2–4].
The prevalence of FMD in the general population is not well defined [5]. However, some reports indicated that the incidence of symptomatic renal FMD is about 4 in 1000 [6]. FMD is thought to be more prevailing in females than in males; representing 91% of patients in the US FMD registry; and hypertension as the most common sign of FMD, with a frequency of 63.8% [4].
A conclusive diagnosis of FMD can only be made with imaging studies. Catheter-based angiography remains as gold standard imaging technique; and angioplasty is the most acceptable option for correcting renal artery FMD who have resistant hypertension. FMD usually demonstrates favorable clinical and anatomical response to angioplasty. Technical success is nearly 100% in most series. Clinically, there is a cure rate in the order of 40% to 50% with an additional 40% to 50% regarded as improved, at last follow-up [6–11].
Resistant hypertension should be evaluated comprehensively and a variety of differential diagnoses may be investigated including FMD as an uncommon cause of renal artery stenosis that could be simply missed; although, atherosclerotic renal artery stenosis is more prevalent than FMD. Our patient had uncontrolled hypertension for nearly 3 years without comprehensive workup. On the other hand, this case highlights that FMD should be kept in mind as a rare cause of resistant hypertension in young males; although it is most common in young females. In almost all of previous studies, a high index of suspicion is crucial in early diagnosis and timely treatment, which can result in rapid and inclusive recovery [4,7,8,10,12,13].
Conclusion
It is essential, particularly for general cardiologists and emergency physicians to be familiar with fibromuscular dysplasia as one of differential diagnosis of resistant hypertension in young adults, which can be well cured with balloon angioplasty.
[1]. Safian RD, Textor SC, Renal-artery stenosisThe New England Journal of Medicine 2001 344(6):431-42. [Google Scholar]
[2]. Gottsater A, Lindblad B, Optimal management of renal artery fibromuscular dysplasiaTherapeutics and Clinical Risk Management 2014 10:583-95. [Google Scholar]
[3]. Meyers KEC, Sharma N, Fibromuscular Dysplasia in Children and AdolescentsCath Lab Digest 2007 15(10) [Google Scholar]
[4]. Olin JW, Froehlich J, Gu X, Bacharach JM, Eagle K, Gray BH, The United States Registry for Fibromuscular Dysplasia: results in the first 447 patientsCirculation 2012 125(25):3182-90. [Google Scholar]
[5]. Olin JW, Gornik HL, Bacharach JM, Biller J, Fine LJ, Gray BH, Fibromuscular dysplasia: state of the science and critical unanswered questions: a scientific statement from the American Heart AssociationCirculation 2014 129(9):1048-78. [Google Scholar]
[6]. Plouin PF, Perdu J, La Batide-Alanore A, Boutouyrie P, Gimenez-Roqueplo AP, Jeunemaitre X, Fibromuscular dysplasiaOrphanet Journal of Rare Diseases 2007 2:28 [Google Scholar]
[7]. Alhadad A, Mattiasson I, Ivancev K, Gottsater A, Lindblad B, Revascularisation of renal artery stenosis caused by fibromuscular dysplasia: effects on blood pressure during 7-year follow-up are influenced by duration of hypertension and branch artery stenosisJournal of Human Hypertension 2005 19(10):761-67. [Google Scholar]
[8]. Amar L, Azarine A, Carreira E, Vidal-Trecan T, Plouin PF, Renal artery fibromuscular dysplasiaPresse medicale (Paris, France : 1983) 2011 40:7-8.:720-25. [Google Scholar]
[9]. Baumgartner I, Lerman LO, Renovascular hypertension: screening and modern managementEuropean Heart Journal 2011 32(13):1590-98. [Google Scholar]
[10]. Sanidas EA, Seferou M, Papadopoulos DP, Makris A, Viniou NA, Chantziara V, Renal Fibromuscular Dysplasia: A Not So Common Entity of Secondary HypertensionJournal of Clinical Hypertension (Greenwich, Conn) 2016 18(3):240-46. [Google Scholar]
[11]. Trinquart L, Mounier-Vehier C, Sapoval M, Gagnon N, Plouin PF, Efficacy of revascularization for renal artery stenosis caused by fibromuscular dysplasia: a systematic review and meta-analysisHypertension 2010 56(3):525-32. [Google Scholar]
[12]. Kim ESH, Olin JW, Froehlich JB, Gu X, Bacharach JM, Gray BH, Clinical Manifestations of Fibromuscular Dysplasia Vary by Patient SexA Report of the United States Registry for Fibromuscular DysplasiaJournal of the American College of Cardiology 2013 62(21):2026-28. [Google Scholar]
[13]. Ralapanawa DM, Jayawickreme KP, Ekanayake EM, A case of treatable hypertension: fibromuscular dysplasia of renal arteriesBMC Research Notes 2016 9(1):6 [Google Scholar]