Comparison of K-loop Molar Distalization with that of Pendulum Appliance - A Prospective Comparative Study
Nagam Reddy Shashidhar1, S.Rama Koteswara Reddy2, Madhukar Reddy Rachala3
1 Professor, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
2 Professor Emirates, Department of Orthodontics, SIBAD Institue of Dental Sciences, Guntur, Andhra Pradesh, India.
3 Associate Professor, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Madhukar Reddy Rachala, Associate Professor, Department of Orthodontics, SVS Institute of Dental Sciences, Appanapally, Mahabubnagar, Telangana- 509002, India.
E-mail: mrachalaortho@yahoo.co.in
Introduction
Molar distalization is the non extraction method of managing Class II malocclusions.
Aim
The purpose of this study was to evaluate the skeletal and dentoalveolar effects of maxillary molar distalization with K-loop appliance, and to compare these effects with that of pendulum group.
Materials and Methods
Class I and dental Class II malocclusions were divided into two groups of 15 each: In Group 1 (nine females and six males; mean age, 16.0±2.6 years) patients were treated with K-Loop molar distalization supported palatally by Nance button, while in Group 2 (seven females and eight males; mean age, 15.4±4.7 years), the patients were treated with conventional pendulum appliance. Standardized lateral cephalograms were taken at the beginning of treatment (T0) and at the end of molar distalization (T1) and the changes were statistically analyzed with paired t-test.
Results
The results showed no statistically significant difference in the amount of molar distalization in either of the appliance groups: the mean amount of molar distal movement of 5.1±0.8 mm and 4.93±1.68 mm was observed in the Group 1 and 2 respectively. The incisors moved mesially by 1.3±0.63 mm in Group 1 and 1.57±0.58 mm in Group 2.
Conclusion
K-Loop molar distalizing appliance has similar skeletal and dentoalveolar effects as that of pendulum appliance, with the advantages of simple yet efficient to control the moment-force ratio to produce all types of tooth movements and also requires minimal patient co-operation.
Class II malocclusion, Dento-aveolar effects, Non extraction treatment, Vertical dimension
Introduction
Correction of Angle’s Class II malocclusion is one of the commonest, yet challenging problem confronting the orthodontic profession. The space required for correction of such cases vary considerably from a few millimeters to several millimeters depending on the severity of crowding and amount of profile convexity reduction required and hence no single space gaining procedures can be universally applied [1]. Two common procedures that are traditionally used to gain space are extractions and expansion. The controversy surrounding the extraction of teeth for orthodontic purposes is well known. Edward H Angle was emphatic about non extraction line of treatment and advocated expansion in all cases [2]. However, in 1930’s his thinking was met with severe criticism by Charles Tweed when relapse following non-extraction expansion treatment was frequently observed and that occlusion was much more stable with less relapse when treated with extraction of teeth [3].
In recent years, number of orthodontic patients treated with extraction procedures has once again come down significantly. Experiences have shown that premolar extraction does not necessarily guarantee stability of teeth alignment, but indiscriminate extraction of teeth in the so-called borderline cases resulted in dishing in of the profile with premature aging appearance [4]. Presently, dentists have realized that the general public often prefers fullness and prominent lips than the orthodontic standards of earlier days. With careful case analysis and treatment planning, it is now possible to treat some of these patients with non-extraction method, which was thought of extraction cases previously. This has led to a “Neo-Angle” school of treatment planning with modified techniques to facilitate non-extraction treatment.
One such technique in the treatment of Class II malocclusion in growing patients with good facial balance and jaw relationship, but with minimum to moderate crowding having hypo to normo divergent growth pattern, is the distalization of maxillary molars. The ability to effectively distalize the maxillary first molar to gain space for correcting the discrepancy is an extremely useful clinical tool. However, case selection is critical, since the space that can be gained to achieve Class I molar and canine relationship and to relieve crowding, if any, by distally moving the maxillary first molars is more or less limited. Working to this end, various types of techniques and devices have been developed like headgears, magnets, pendulum appliance, NiTi coil springs, Jones jig, distal jet appliance etc., [5–10]. Although, all these molar distalizing appliances reduced the need for patient co-operation and produced satisfactory amount of distal movement of molars, they all lacked the ability for bodily distal movement of maxillary molars and crown tipping could not be avoided.
In 1995 Varun Kalra introduced “K-Loop” appliance for molar distalization in Class II malocclusion, which he claimed to have been developed in accordance to certain biomechanical principles as out lined by Charles Burstone and has the ability to move the maxillary molars distally with total bodily control which is of great clinical significance [11]. He concluded that “K-Loop” appliance has several advantages over other appliances such as: Simple yet efficient, control the moment of force ratio to produce bodily movement, controlled tipping or uncontrolled tipping as desired, easy to fabricate and place, hygienic and comfortable for the patient, requires minimal patient co-operation.
Yet, till now, very few studies have been published in the literature to substantiate the validity of K-Loop molar distalization appliance with that of Pendulum appliance. Hence, this study was done to evaluate the skeletal and dental effects of the K-Loop appliance.
Materials and Methods
This was a prospective study, which included 30 patients from the Department of Orthodontics and Dentofacial Orthopaedics, College of Dental Sciences, Davangere, India, who needed molar distalization in the maxillary arch. The inclusion criteria were: Class I skeletal pattern with Class II or end on molar relationship, mild maxillary dental protrusion, mild to moderate crowding, straight profile, low to moderate mandibular plane angle and good expectations for patient cooperation. The exclusion criteria were: Retrognathic profile (Class II skeletal with orthognathic maxilla and retrognathic mandible), skeletal and dental open bite; excessive lower anterior face height. The patients were randomly divided into two groups of 15 each: In Group 1 (nine females and six males; mean age of 16.0 ± 2.6 years) patients were treated with K-Loop molar distalization supported palatally by Nance button, while in Group 2 (seven females and eight males; mean age of 15.4 ± 4.7 years), the patients were treated with conventional pendulum appliance. The duration of the study was approximately six months.
K-loop molar distalization: As described by Kalra, K-Loop was fabricated with 0.017"x0.025" TMA wire [11]. The main advantage of TMA wire over SS is that, the amount of activation can be twice before it undergoes permanent deformation. The size of each loop was 8mm long, 1.5mm wide with legs of loop bent 20o down. Stops (1.5 mm long) were bent into the wire 1mm distal to the distal mark (mesial of the molar tube) and 1mm mesial to the mesial mark (distal of the premolar bracket) which helps to keep the appliance away from the soft tissue and also allows 2mm activation [Table/Fig-1]. For anchorage control Nance button was used.
K-Loop distalization: Top row- before distalization; Bottom row- after distalization.

After two months the appliance was reactivated 2mm to further distalize the molars. Since the distal end of the wire was not bent, it was easy to remove from the molar tube. In most cases, one reactivation was sufficient to get the molars into super Class I relationship with duration of approximately 5-6 months. Once the molars were distalized, K-loop was removed and the molars were stabilized in their new positions with transpalatal bar and a stopper in the arch wire just mesial to buccal tube.
Pendulum appliance: The patients in this group were treated with pendulum appliance as described by Hilgers. It consists of spring made of 0.036" TMA wire that produces a light continuous force on molars and a large acrylic button in the pre-maxillary area as an anchor component. The anchor component is secured to the premolars with bands or bonding. This design incorporates an inverted horizontal loop placed half way between the helix and the molar tubes. By opening the horizontal loop, a buccal or distal uprighting force was created producing a bodily movement of the molars [Table/Fig-2].
Pendulum appliance: Top row- before distalization; Bottom row- after distalization.

Cephalometric measurements: The skeletal and dental effects of the molar distalization with K-Loop and Pendulum appliances were evaluated with, serial lateral cephalograms taken before treatment (T0) and at the end of molar distalization (T1) for all the patients in both the study groups. Angular and linear measurements were made to determine anchorage loss, molar movement and vertical changes. The cephalometric profile analysis included (eight skeletal and seven dento-alveolar,) six linear and six angular variables [Table/Fig-3]. Descriptions of the measured parameters are given in [Table/Fig-4].
Left: Linear measurements used in the study (1)U6A-Y (2)UIA-Y (3)U6MB-Y(4) UIE-Y (5)LAFH (6)UI-PP. Right: Angular measurements used in the study (1) GoGn-Sn (2) U6-PP (3)UI-PP (4) ANB (5) SNA (6) SNB.
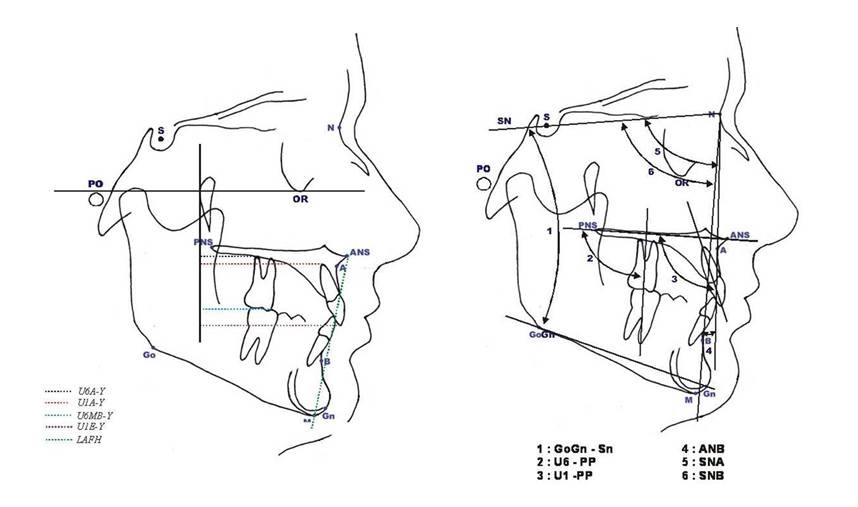
Description of cephalometric parameters used in the study.
| S.No | Molar Movement | Description |
|---|
| 1 | U6-PP | Upper first molar long axis (U6) to Palatal Plane (PP) (Angular) |
| 2 | U6MB-Y | Upper first molar mesio-buccal cusp (U6MB) to Y (Linear). |
| 3 | U6A-Y | Upper first molar disto-buccal root apex (U6A) to Y (Linear). |
| Anchorage Loss: |
| 4 | U1-PP | Upper central incisor long axis (U1) to Palatal Plane (PP) (Angular). |
| 5 | U1A-Y | Upper central incisor edge (U1 E) to Y (Linear). |
| 6 | U1E-Y | Upper central incisor apex (U1A) to Y (Linear). |
| Vertical Changes: |
| 7 | U6MB-PP | Upper first molar mesial buccal cusps (U6MB) to Palatal Plane (PP) (Linear). |
| 8 | GoGn - SN | Angle formed between anterior cranial base and mandibular plane (Angular). |
| 9 | LAFH | ANS to Gn (Linear) |
| Skeletal Changes: |
| 10 | SNA | Anterio-posterior position of the maxilla |
| 11 | SNB | Anterio-posterior position of the mandible |
| 12 | ANB | Difference between SNA and SNB |
Statistical Analyses
Mean and standard deviations were calculated for all cephalometric measurements at pre-treatment (T0) and post-treatment (T1) in both the groups. Paired t-test were used to analyze differences between the T0 and T1 cephalometric variables of the two groups, and unpaired t-test to evaluate differences between the groups. A p-value of <0.05 was considered statistically significant. Fifteen randomly selected cephalograms from T0 to T1 were retraced and re-measured by the same investigator after a period of two weeks.
Results
[Table/Fig-5] shows the statistics (mean and standard deviations) for observations at T0 and T1 and also changes during the treatment interval as measured from the cephalometric radiographs.
Comparison (Paired and unpaired t-test) of changes with a K-Loop appliance (Group 1) and Pendulum Appliance (Group 2).
| Parameter | Pre(T0) | Post(T1) | Change | Pre(T0) | Post(T1) | Change | Significance |
|---|
| 1 | U6-PP | 80.1±6.76 | 74.8±5.55 | 5.3±2.26 | 82.0±5.16 | 76.8±4.59 | 5.2±1.38 | NS |
| 2 | U6MB-Y | 26.3±3.20 | 21.2±3.08 | 5.1±0.88 | 27.6±2.54 | 22.67±3.08 | 4.93 ± 1.68 | NS |
| 3 | U6A-Y | 22.9±4.18 | 19.7±2.45 | 3.2±2.62 | 23.34±3.12 | 20.3±3.54 | 3.04±1.87 | NS |
| 4 | U1-PP | 115.4±5.44 | 121.1±7.42 | -5.7±4.72 | 118.8±4.14 | 124.3±5.34 | -5.5±3.45 | NS |
| 5 | U1A-Y | 47.3±4.15 | 45.7±4.53 | 1.6±1.07 | 46.2±3.92 | 44.6±4.72 | 1.74±2.15 | NS |
| 6 | U1E-Y | 57.6±4.18 | 58.9±4.21 | -1.3±0.63 | 57.93±3.29 | 59.5±3.87 | -1.57±0.58 | NS |
| 7 | U6MB-PP | 21.7±1.83 | 24±1.15 | -2.3±2.06 | 21.22±1.65 | 24.72±1.43 | -2.5±1.89 | NS |
| 8 | GoGn - Sn | 29.2±1.69 | 30.65±0.88 | -1.45±1.54 | 29.11±1.27 | 31.54±1.23 | -2.43±1.15 | NS |
| 9 | LAFH | 65.1±4.09 | 67.3±3.95 | -2.2±1.55 | 65.7±3.96 | 68.6±2.73 | -2.9±2.01 | NS |
| 10 | SNA | 80.7±3.06 | 79.1±2.19 | 1.6±1.65 | 80.7±3.06 | 79.1±2.19 | 1.6±1.65 | NS |
| 11 | SNB | 77.8±2.23 | 76.2±1.48 | 1.6±1.50 | 77.8±2.23 | 76.2±1.48 | 1.6±1.50 | NS |
| 12 | ANB | 2.9±1.37 | 2.95±1.74 | -0.05±1.12 | 2.9±1.37 | 2.95±1.74 | -0.05±1.12 | NS |
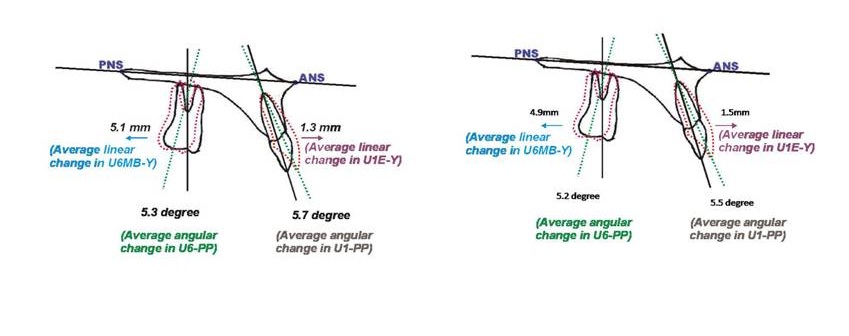
The K-Loop appliance primarily affected the maxillary dentition and to a minor extent the maxilla and mandible. The maxillary molar moved distally by 5.1mm (±0.8mm), in contrast the central incisors moved mesially by 1.3mm (±0.63mm) and the molars tipped distally by 5.3o (±2.26o). The amount of maxillary first molars intrusion was slightly (not statistically significant). Along with this, minor vertical increases in both mandibular molars and incisors were observed after molar distalization with K-Loop. Increase in the vertical dimension was indicated by a slight opening of the mandibular plane angle (GoGn-Sn) by 1.45o (±1.54o) and by an increase in lower anterior facial height 2.2mm (±1.55mm). The minimal sagittal skeletal effect of K-loop is reflected in the change in the ANB angle, which decreased by 0.05o ± 1.12o from T0 to T1 but was not statistically significant. Significant co-relation between the amount of distalization and degree of distal molar tipping was found. Minimal tipping with increased distalization was noted [Table/Fig-5].
In Group 2 (Pendulum Appliance) the maxillary molar moved distally by 4.93±1.68 mm and the incisors moved mesially by 1.57±0.58 mm, showing no significant difference between Group 1 and 2. Change in the vertical dimension was more in the patients treated with pendulum group, with an increased mandibular plane angle (GoGn-SN) of 2.43° (±1.15o) and by an increase in lower anterior facial height by -2.9 mm (±2.01mm). The sagittal skeletal effect of pendulum appliance is reflected in the change in the ANB angle, which increased 0.04°±1.84o from T0 to T1 which was statistically insignificant with that of the Group 1 [Table/Fig-6].
Changes in tooth positions before and after distalization with K-Loop (left) and Pendulum Appliance (right).
Discussion
The correction of Class II malocclusion has always been a challenge in Orthodontics. Distal movement of maxillary first molar is a common goal in the treatment of a Class II molar relationship and in the resolution of a tooth size/arch length discrepancy in the maxillary arch. The mechanics used to apply the force required to distalize the maxillary first molar include those that require patient cooperation as well as those that eliminate the need for patient compliance to activate the force system. The appliance that eliminate the need for patient cooperation to activate the force system are termed “noncompliance appliance” and include the repelling magnets, pendulum appliance, compressed stainless steel or nickel titanium springs, the distal jet appliance, and the K-Loop etc.
In the present study K-Loop efficiently distalized the maxillary molar teeth to a Class I molar relationship and its skeletal and dental effects are similar to that of Pendulum appliance. However, the effects of both the distalizing appliances on craniofacial skeleton and associated soft tissue are less pronounced.
Dentoalveolar effect: The maxillary molar moved distally by 5.1±0.8mm in K-Loop group and 4.93±1.68mm in Pendulum group over a period of six months at a mean monthly rate of 1.1mm/month. There was no statistically significant difference between the two groups. Reiner study on molar distalization using modified Nance appliance and showed approximately 0.76mm movement per month with uncooperative patients who missed the reactivation appointment whereas it was 0.96 mm/month in the other group [12]. Bondemark et al., conducted a study to compare two intraoral distal movement systems and found that average distal molar movement obtained with NiTi coils was 3.2mm, whereas with magnets it was 2.2mm after six months of treatment [13]. Molar tipping was very high (14.5o) in the study conducted by Byloff when compared with the 7.4o found in other studies [14–16]. In the present study the molar tipping was less (5.3o±2.26o) as compared to other studies [13], because the K-Loop is prepared in such a way that the activation produces the distal molar movement and the 20o bend in the horizontal arm produces the distal root movement. To achieve bodily distal molar movement enough time should be given after the crown movement to upright the molar root.
In most of the intra-oral molar distalizing appliances (pendulum, distal jet etc.) the anchorage is taken from palate. In the present study anchorage was taken from palate by Nance button and also the Class II elastics were used in both the groups in some of the cases to reinforce anchorage. The incisors moved mesially by 1.3mm (±0.63 mm) in K-Loop group where as it is 1.57±0.58 mm in pendulum group, showing no significant difference between them.
Skeletal effect: With regard to skeletal changes of the maxilla, SNA angle showed no statistical difference in both the groups, confirming previous findings. This finding may suggest that A point was not affected by anteriorly oriented forces with in a short period of time. Vertical changes revealed no significant changes as demonstrated by Bondemark [13], Muse [17] and Acar [18]. In the present study the palatal plane could not remain unchanged in both the groups during the treatment period. The occlusal plane opened as the mandibular plane (1.4o) and lower anterior facial height (2.2mm) increased in K-Loop distalization and in pendulum group it was 2.40 and 2.9mm. The mandible rotated down and backward and the overbite decreased. Once the distalization is completed, the K-Loop should not be removed for 3-4 months, which allows uprighting of molar root and premolars start moving distally due to transeptal fibre pull.
There are many ways to maintain the distalized space gained e.g., : insta-nance, utility arches, fixed functional appliance, headgears. Once the molars and premolars, become one unit, then by reinforcing the anchorage and maintaining the Class I molar relationship the anteriors are retracted. Although the results of this study indicate that the K-Loop is effective in moving the maxillary molars distally, the clinician should make sure that the diagnosis of the particular case selected for distalization is appropriate.
Limitation
The limitations of this study were limited sample size and accuracy of the study can be improved by using latest diagnostic aids like e-models and CBCT for evaluation of changes, inclusion of another group using mini-implants etc. Although the present study has some limitations, the results of this study are useful in choosing the appropriate appliance between the pendulum and K-Loop for molar distalization.
Conclusion
In the present study, the skeletal and dental effects of molar distalization with K-Loop appliance were compared with those of pendulum appliance to evaluate the effectiveness of former. K-Loop efficiently distalized the maxillary molar teeth to a Class I molar relationship with minimal anchorage loss and molar tipping and its skeletal and dento-alveolar effects are similar to that of pendulum group. K-Loop primarily affects the maxillary dentition; however there are secondary minor effects on the soft tissue and skeletal components. No significant vertical changes were observed during distalization. In comparison with pendulum appliance, the K-Loop molar distalization has the advantages of simple, less cumbersome, easy to fabricate and place, hygienic and comfortable for patient, requires minimal patient co-operation, and yet efficient to control the all types of tooth movements, make it as definitely preferable option for the effective molar distalization appliance.
[1]. Proffit WR, Diagnosis and treatment planning. In: Proffit WR, Fields HW Jr, edsContemporary Orthodontics 1986 StLouisCV Mosby:158 [Google Scholar]
[2]. Angle EH, Treatment of malocclusion of the teeth and fractures of the maxillae, Angle’s system. Ed 6, 1900 S.SPhiladelphiaWhite Dental Manufacturing Co [Google Scholar]
[3]. Tweed C, Clinical Orthodontics 1966 St LouisMosby [Google Scholar]
[4]. Proffit WE, Forty-year review of extraction frequency at a university orthodontic clinicAngle Orthod 1994 64:407-14. [Google Scholar]
[5]. Siatkowski RE, Assymetic headgear. In Nanda R (ed)Biomechanics in orthodonticsPhiladelphiaW B Saunders:130 [Google Scholar]
[6]. Gianelly AA, Vaitas AS, Thomas WH, Berger DG, Distalization of molars with repelling magnets. A case reportJ Clin Orthod 1988 22(1):40-44. [Google Scholar]
[7]. Hilgers J.J, The Pendulum appliance for class II non-compliance therapyJ Clin Orthod 1992 26(11):706-14. [Google Scholar]
[8]. Locatelli R, Bednar J, Dietz VS, Gianelly AA, Molar distalization with superelastic NiTi wireJ Clin Orthod 1992 26:277-79. [Google Scholar]
[9]. Jones R.D, White T.M, Rapid Class II molar correction with an open-coil jigJ Clin Orthod 1992 26(10):661-64. [Google Scholar]
[10]. Carano A, Testa M, The distal jet for upper molar distalizationJ Clin Orthod 1996 30:374-80. [Google Scholar]
[11]. Kalra V, The K-Loop molar distalizing applianceJ Clin Orthod 1995 29:298-301. [Google Scholar]
[12]. Reiner TJ, Modified Nance appliance for unilateral molar distalizationJ Clin Orthod 1992 26:402-04. [Google Scholar]
[13]. Bondemark L, Kurol J, Bernhold M, Repelling magnets versus superelastic nickel-titanium coils in simultaneous distal movement of maxillary first and second molarsAngle Orthod 1994 64(3):189-98. [Google Scholar]
[14]. Byloff FK, Darendeliler MA, Distal molar movement using the pendulum appliance. Part 1: Clinical and radiological evaluationAngle Orthod 1997 67(4):249-60. [Google Scholar]
[15]. Itoh T, Tokuda T, Kiyosue K, Hirose T, Matsumoto M, Charonas Molar distalization with repelling magnetsJ Clin Orthod 1991 25:611-17. [Google Scholar]
[16]. Mariani L, Maino G, Caprioglio A, Skeletal versus conventional intraoral anchorage for the treatment of class II malocclusion: dentoalveolar and skeletal effectsProg Orthod 2014 15:43 [Google Scholar]
[17]. Muse DS, Fillman MJ, Emmerson WJ, Mitchell RD, Molar and incisor changes with Wilson rapid molar distalizationAm J Orthod Dentofacial Orthop 1993 104(6):556-65. [Google Scholar]
[18]. Acar AG, Gürsoy S, Dinçer M, Molar distalization with a pendulum appliance K-Loop combinationEur J Orthod 2010 32(4):459-65. [Google Scholar]