Dengue is an arboviral infection transmitted by Aedes mosquitos. Clinically dengue infection varies from asymptomatic infection or mild fever to severe Dengue Haemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS) [1,2]. Although the disease with clinical features similar to dengue has been reported in India since 19th century but Dengue virus was first isolated and reported in India in1945 [3]. Thereafter there have been many outbreaks of dengue with increased cases of DHF and DSS [4]. Dengue is now an endemic disease in India especially in urban populations like Delhi [5]. In Delhi large number of dengue cases is reported every year in the months July to December, with a peak in mid-September to mid-October [6]. The first outbreak of dengue in Delhi was reported in 1967 [7], thereafter Delhi has faced many outbreaks in the years 1996, 2003, 2005 and 2006 [8,9].
In the year 2015 Delhi has suffered one of the worst dengue outbreaks, with the highest number of positive cases in recent years. There were more than 15000 dengue confirmed cases, which has been reported by the government agencies [10]. The toll of death due to dengue was also highest among recent years with number of deaths reaching up to 60 [10]. Most common hypothesis for the pathogenesis of severe dengue (DHF and DSS) is the antibody mediated immune enhancement in a secondary dengue case, which results due to the presence of non-neutralizing antibodies in patient’s serum from a past infection of Dengue with different serotype [11]. The present study analyzes the seroepidemiological aspects of this outbreak in context with the dengue cases in previous six years and reviews our one test strategy of performing either NS1 antigen or IgM antibody test for the confirmation of Dengue. The ratio of primary and secondary dengue cases during this outbreak was also determined in this study.
Materials and Methods
A cross-sectional study was performed at the Department of Microbiology, Maulana Azad Medical College and associated Lok Nayak hospital from January to December 2015. A total of 7177 serum samples from suspected dengue cases attending OPD or admitted in the wards of Lok Nayak Hospital were tested for the confirmation of Dengue. Cases included of adults as well as pediatric patients and the age group varied from less than one year to 65 years. A suspected case of dengue was considered a patient with acute febrile illness and signs and symptoms suggestive of Dengue; headache, retro-orbital pain, myalgia, arthralgia, rash and haemorrhagic manifestation, etc. [12].
Dengue NS1 antigen and dengue IgM antibody detection tests for the confirmation of dengue cases were performed. Dengue Early ELISA kits (PenBio) and Dengue NS1 Ag Microlisa (J.Mitra & Co) were used for the detection of NS1 antigen and NIV Den IgM Capture ELISA kits were used for the detection of IgM antibodies. Considering the kinetics of the appearance of dengue NS1 antigen and IgM antibody in serum, the patients were segregated on the basis of number of days after the onset of the fever. We performed NS1 antigen ELISA for the patients (4661) who had fever for less than 5 days, and IgM antibody ELISA for the patients (2516) who had fever for five or more days. In order to review this strategy, after the end of the outbreak randomly selected, 100 NS1 negative samples were retested for IgM antibody and 100 randomly IgM negative samples were retested for NS1 antigen. ELISA tests were performed as per the manufacturer’s instructions.
Seventy six random samples from laboratory confirmed dengue cases in 2015 were selected for IgG avidity ELISA in order to determine the ratio of primary and secondary dengue cases. For avidity tests Pen Bio IgG ELISA kit with some modifications in the method which is also described for IgG antibody for cytomegalovirus infection was used [13]. All serum samples were tested in duplicates. After initial incubation for 30minutes at 37oC, the wells were washed six times with the wash buffer and then 100 μl of 8 M urea in PBS was added to second well of each sample, whereas 100μl of PBS was added to the first well. Plate was kept at room temperature for 5 minutes and then was washed twice with the wash buffer. Rest of the procedure was followed as per the manufacturer’s instruction. An avidity index was calculated by dividing the OD value of the well exposed to urea solution with the OD value of the well not exposed to urea. Serum samples with Avidity index less than 0.8 were considered as primary dengue and with avidity index more than 0.8 were considered as secondary dengue.
Results
A total samples 7177 were tested out of them 2358 were positive either by NS1 antigen or for IgM antibody. Positivity rate of the NS1antigen test was remarkably higher, 37.1% (1732/4661) than that of the IgM antibody tests, which was 24.8% (626/2516) [Table/Fig-1&2].
Percentage positivity rate of NS1 antigen and IgM antibody detection.
| Tested | Positive |
|---|
| IgM antibody | 2516 | 626 (24.8%) |
| NS1 antigen | 4661 | 1732 (37.1%) |
| total | 7177 | 2358(32.8%) |
Overview of the study and the results.

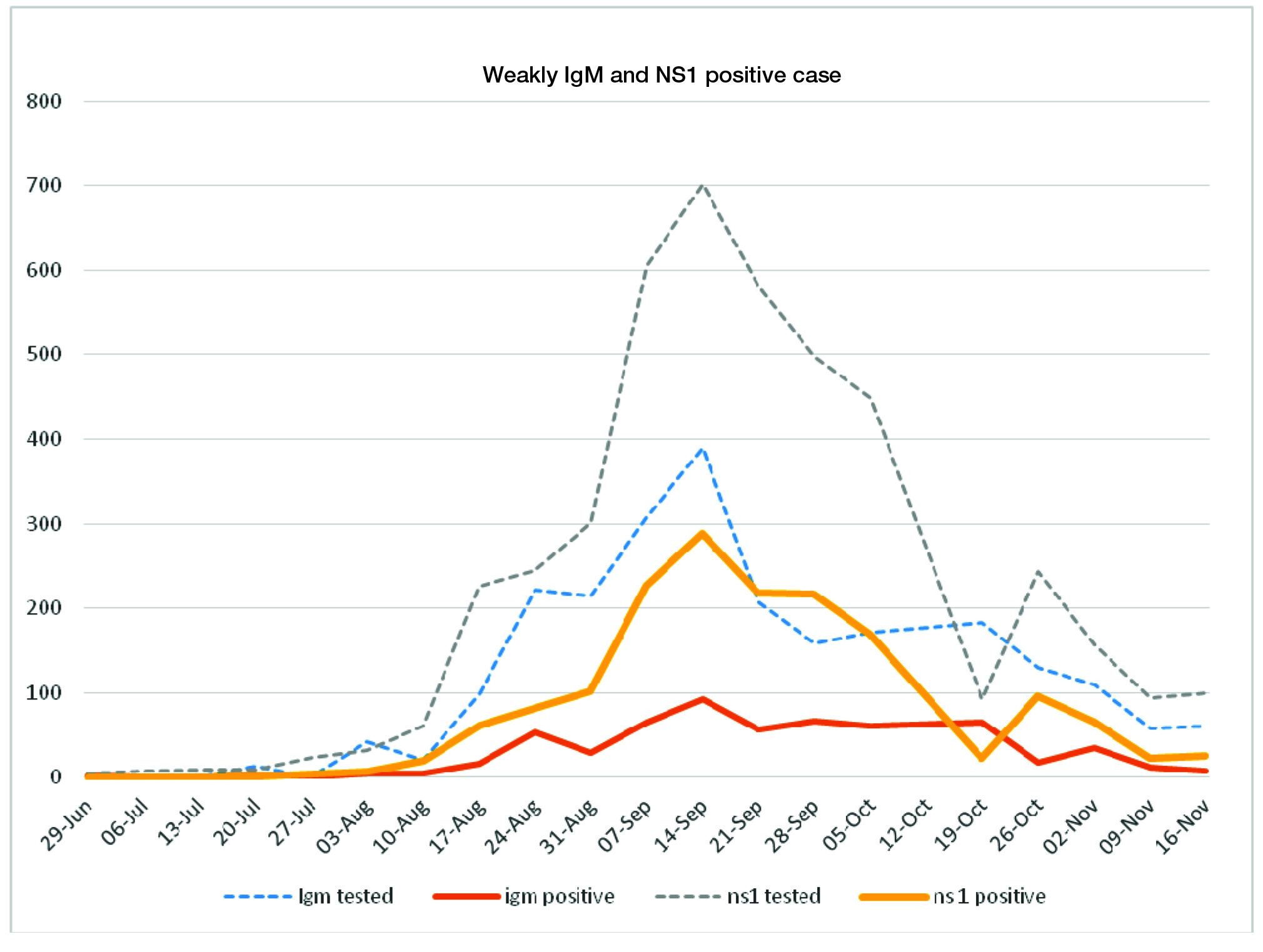
Number of positive dengue cases gave a peek in the middle of September with highest number of positive cases in the week 14 Sep to 20 September (391 positive out of 1092 tested). There after number of dengue cases started to decline and there was a second upraise of dengue cases in the last week of the October [Table/Fig-3].
NS1 antigen and IgM samples tested and positives during the outbreak.
Out of 76 random samples tested for dengue IgG Avidity ELISA 52 (68.4%) were found to be of secondary dengue.
Among the negative samples those were tested for confirmation, out of 100 NS1 negative samples 8 were positive for IgM antibody and out of 100 IgM negative samples 6 were positive for NS1 antigen.
Discussion
At our institute in 2015 the first case of dengue was confirmed as positive in the last week of June. Thereafter no sample was tested positive for two consecutive weeks. After 20th July dengue samples were tested positive regularly.
Delhi faces large number of dengue cases every year in the months July to November which is ascribable to the growing population of the city and the rapid urbanization [14]. But there was a remarkable rise in the number of dengue cases in the year 2015 as we compare it from the previous year’s case at our institute [Table/Fig-4].
Dengue samples tested in last seven years (positive/tested).
| Months | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 |
|---|
| Jan | 0/5 | 0/6 | 0/8 | 0 | 0/15 | 0/10 | 0/33 |
| Feb | 0/3 | 0/3 | 0/9 | 0 | 0/19 | 0/36 | 0/34 |
| Mar | 0/16 | 0/7 | 0/12 | 0/18 | 0/18 | 0/20 | 0/38 |
| Apr | 0/10 | 0/5 | 0/15 | 0/20 | 0/13 | 0/11 | 0/19 |
| May | 0/8 | 4./9 | 0/25 | 0/9 | 0/4 | 0/66 | 0/46 |
| Jun | 0/9 | 1./20 | 0/20 | 0/13 | 0/40 | 1/58 | 0/30 |
| July | 0/21 | 4./28 | 0/52 | 0/18 | 12/78 | 1/114 | 7/69 |
| Aug | 2./19 | 82/251 | 6./92 | 5/75 | 40/202 | 4/367 | 248/952 |
| Sept | 3./36 | 151/530 | 25/201 | 37/221 | 601/1934 | 53/432 | 1220/3383 |
| Oct | 131/265 | 330/820 | 52/313 | 379/1020 | 580/1952 | 158/576 | 701/1895 |
| Nov | 60/154 | 73/254 | 32/166 | 172/695 | 187/482 | 122/344 | 175/590 |
| Dec | 10/36 | 5/25 | 1./47 | 4/46 | 7/40 | 5/72 | 7/88 |
| Total | 206/582 | 646/1978 | 116/935 | 597/2135 | 1427/4915 | 344/2097 | 2358/7177 |
To make it easy to understand in the graph [Table/Fig-5], we included only the data of four months (Aug – Nov) for seven years. The year wise graph in the figure shows that with the exception of 2011 and 2014 dengue cases are constantly on a rise every year. This type of epidemiological change has also been reported earlier [15]. Although it is difficult to determine why the incidence of dengue cases increases after every few years, but there are many factors which can be attributed as important, like rainfall, preventive measures taken by people and the authority, immune status for the prevalent dengue serotype in the population, strategy for the case confirmation and the reliability of the Dengue notification system etc.
Dengue positive cases in last seven years.

Rainfall and the source of fresh water in which the mosquito breeds are two important contributing factors. In 2010 there were a significant rise in dengue cases and was mostly attributed to the heavy rain fall in that year. But the contribution of rainfall is only conditioned with the availability of breeding places and to the fact that how effective preventive measures are being practiced to reduce the mosquito population. A very large no. of cases in the year 2015, when the rainfall was not remarkably higher than the previous years, tells us that in urban area most of the breeding places for mosquito are artificial and manmade like coolers, empty pots, construction sites, etc. These urban type breeding places largely remain unaffected by the presence and absence of the rainfall. Moreover these breeding places can easily be identified and destroyed with proactive measures.
There was remarkable difference between the positivity rates of NS1antigen and IgM antibody tests, percentage of samples tested positive for IgM and NS1 were 24.8% (626) and 37.1% (1732) respectively and this difference was maintained during the outbreak except in the last week of October; when positivity rate of the NS1 test started to decline while that of the IgM test increased [Table/Fig-3]. This might have happened owing to the fact that more early and acute phase samples were received while the outbreak was going on due to the widespread apprehension whereas at the beginning and at the end of the outbreak more of the convalescent phase samples were received and in convalescent samples NS1 antigen levels starts to fall [16].
These results clearly tell us that if we confirm dengue cases only by NS1 antigen or IgM antibody alone, we may miss many cases, as dengue IgM antibody starts developing only after 4-5 days and after antibodies are developed NS1 antigen starts declining. To overcome this problem the proposed cost- effective method is that we segregate the patients on the basis of onset of fever and perform NS1 antigen test for acute cases and IgM for convalescent cases [17] (fever more than five days).
Among the negative samples tested for confirmation, out of 100 NS1 negative samples 8 were positive for IgM antibody and out of 100 IgM negative samples 6 were positive for NS1 antigen. One possible explanation, for the missed dengue cases by IgM testing even in convalescent cases, can be that sensitivity of the IgM testing for the diagnosis of dengue cases with secondary infection is not as good as for the primary dengue infection [18]. For NS1 antigen test also sensitivity is not same for all the serotypes [19]. It shows that the ideal method for the serodiagnosis of dengue is that every suspected case should be tested for both NS1 antigen and IgM antibody.
In Delhi more than 25% population has been reported to have a past infection of Dengue [20]. Very high percentage of secondary dengue is reported in the area where incidence of dengue is very high. A study from Thailand reports 96 (81.4%) out of 118 dengue cases as secondary dengue cases [21]. Severe dengue infection is often attributed to the non-neutralizing antibodies present in plasma from the past infection of dengue. This indicates an alarming state that in future outbreaks of dengue, there may be higher number of secondary dengue cases with severe manifestations.
Limitation
This study does not tell about the serotypes of the dengue virus circulated in the outbreak. Further studies are required to confirm the cause of missed cases by IgM antibody and NS1 antigen.
Conclusion
The study concludes that dengue is still a serious health problem in Delhi as the number of cases in Delhi is on constant rise with the exception of 2011 and 2014, which may be attributed to rapid urbanization and demands necessity of strict and vigorous vector control programs. The study also concludes that if we perform only IgM antibody and NS1 antigen detection test for patients, we may miss many positive cases and both the tests should be performed for each patient. Due to the increased prevalence of past infection of dengue, percentage of secondary dengue cases is also increasing in Delhi.