Introduction
Multiple sclerosis (MS) as a chronic disease could affect patients’ various domains of life.
Aim
This study was conducted to study the effect of yoga on the physiological indices, anxiety and social functioning of patients with MS in southwest, Iran.
Materials and Methods
In this clinical trial study, 60 MS patients were enrolled according to inclusion criteria and randomly assigned to two groups of 30 each. Prior to and after intervention, the patients’ vital signs were measured. For case group yoga exercises were performed three sessions a week for 12 weeks while control group performed no exercise. The data were gathered by questionnaire and analysed by descriptive and analytical statistics in SPSS.
Results
Prior to intervention, there was no significant difference in fatigue severity and pain between the two groups but the mean fatigue severity and pain in case group decreased compared to the control group after the intervention. Prior to intervention, there was no significant difference in mean physiological indices between the two groups but the mean physiological indices in case group decreased significantly after the intervention (p<0.05).
Conclusion
Yoga is likely to increase self-efficacy of MS patients through enhancing physical activity, increasing the strength of lower limbs and balance, and decreasing fatigue and pain, and finally to promote social functioning and to relieve stress and anxiety in these patients.
Introduction
Multiple sclerosis (MS) is an autoimmune disease, that through demyelinating the neurons in Central Nervous System (CNS) [1] causes symptoms including muscle weakness, fatigue, ataxia, troubled speaking, double vision, loss of cognitive functions, impaired vision, muscle paralysis, spastic paralysis of limbs, disturbance of sphincter control, sexual impotence especially in men, speech disorders, epilepsy, tremor during activity and depression [2]. MS is a chronic, progressive disease of CNS, which is mainly developed in the youth and imposes stupendous costs on family, community, and government [3]. In recent years, the MS prevalence has been increasing worldwide [4,5]. Although there are no definite figures of the patients with MS, per Iranian MS Society, about 40,000 are suffering from MS in Iran [3,4]. As a chronic disease, MS could affect patients’ various domains of life including social, physical, mental, and economic [6–8] and make the patients face many challenges in life. A common problem of MS patients is fatigue that affects quality of life (QOL), balance, and concentration and leads to declined energy and activity, lack of motivation, depression, anxiety, and disorders of sleep and motor systems [9]. Fatigue could be due to the course and/or the complications of the disease such as loss of appetite, infections, depression, sleep disorders, spasms, pain, anxiety, etc [10]. Pain affects various domains of QOL of patients. Study findings indicate that the patients suffer much pain due to central and peripheral nervous neuropathy, trigeminal neuralgia, painful spasms, and regional pain syndrome [11]. Most MS patients suffer from glossopharyngeal neuralgia and myelitis so that management and control of pain face many challenges. Use of medicine to relieve pain leads to many complications, than use of non-pharmacologic approaches such as massage therapy, could be appropriate for pain relief in MS patients [11,12]. On the other hand, MS is a stressful experience for the patient, throughout which the patient has a low control of its condition or outcomes both physiologically and mentally [4]. An important factor of anxiety is fear of the unknown. The patient is afraid of losing socioeconomic status, occupation or financial security, social and family roles, impaired lifestyle, being separated from relatives, and even death. Most patients suffer despair and hopelessness [5]. Anxiety affects all domains of the patients’ life and strongly influences how their needs are met [6]. In addition, anxiety causes increase in pulse rate and blood pressure, which could lead to irreversible complications. Continued anxiety increases metabolism in the body and hence further oxygen is consumed. Moreover, the body responds to anxiety by increasing the depth of breathing. High levels of anxiety intensify perception of pain, as well. Autonomic stimulation patterns of pain and anxiety are similar; stressful environment or the attitude of the individuals around may increase the patient’s anxiety and reduce pain tolerance [7].
Although pharmacotherapy is the first choice of treating MS, currently non-pharmacologic approaches such as massage therapy, programmed exercise, etc, have attracted great attention as complementary therapies for MS due to the low cost and ease of implementation [13]. Hassanpour-Dehkordi and Jivad study indicated that yoga contributed to improved general health and desire to live in MS patients [3]. Results of other studies showed that exercise could reduce fatigue and pain in MS patients [14]. Another study demonstrated that exercise caused psychological and social functioning, energy, self-esteem and QOL to enhance [15]. Due to the complications caused by MS, this disease could affect social functioning and QOL of the suffering patients [16]. Henricksson et al., reported that MS patients’ QOL declined considerably over time with escalating symptoms [12].
Improvement of social functioning and QOL of MS patients are particularly important so that mental and physical ability, anxiety, fatigue and pain are directly correlated with social functioning in MS patients [3]. Therefore, many efforts are being made to promote social functioning and to relieve fatigue and anxiety of MS patients. Physical and mental exercise such as yoga as non-pharmacologic approaches could enhance biological, psychological, and social functioning of these patients by reducing the intensity of MS symptoms. Therefore, this study was aimed to investigate the effects of yoga on physiological indices, anxiety, and social functioning in MS patients.
Materials and Methods
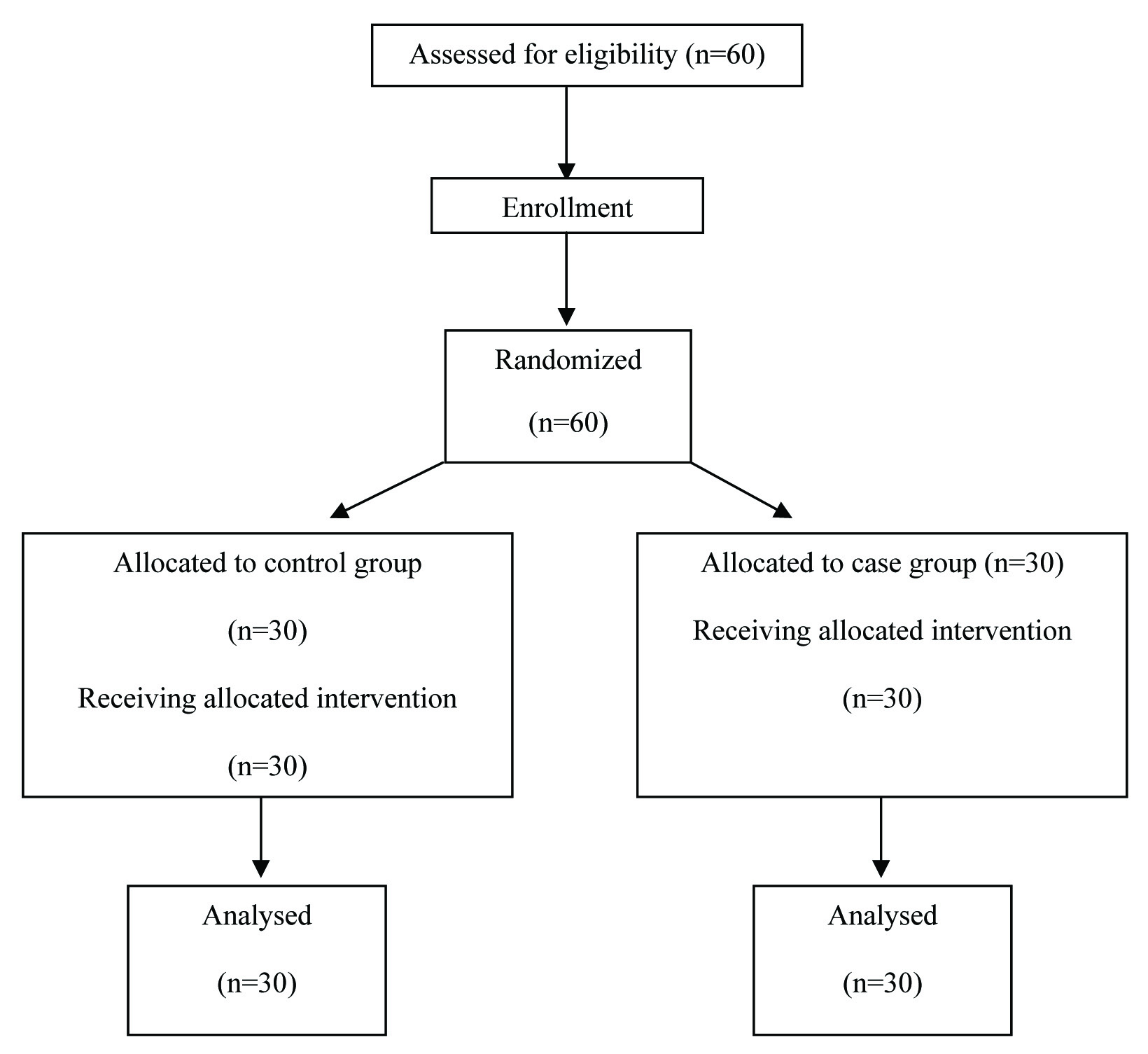
This clinical trial study is single-blind and holds the approval of Research and Technology Deputy of Shahrekord University of Medical Sciences. In view of the previous studies and the formula of sample size calculation, 60 patients were enrolled [3]. For data gathering, convenience, random method was adopted. At first, the units of study population were numbered and the numbers were recorded on small, similar cards. Then, we sent all cards in a box and after shaking the box took a card randomly out of the box each time and registered its number. This process continued until the desired sample size was derived [Table/Fig-1]. The participants were randomly assigned to two groups of case and control. The inclusion criteria into the study consisted of definite diagnosis by McDonald criteria of MS [17], patients consent to participate in the study, and the ability to speak and move, and to perform daily activities. Exclusion criteria were: inability to do exercise yoga or unwillingness to cooperate. During the study, 10 from case group and 10 from control group were excluded because of failure to cooperate, exacerbation of the disease, and family problems. The participants were enrolled per their medical file by systematic randomization and then they were randomly assigned to two groups.
Flow chart showing the recruitment of participants.
Prior to any interventions, the patients’ vital signs and anxiety intensity were measured by Spielberg Anxiety Inventory [18], pain was measured by Bayer numerical scale, and fatigue was measured. Each patient underwent the assigned intervention. Vital signs of patients were measured in the supine position and uniformly by researcher-owned sphygmomanometer. Each patient’s radial pulse was counted in supine position in full one minute. For case group (n=30) yoga exercises were performed three sessions a week for 12 weeks. Yoga exercise sessions were three 60- to 70-minute sessions per week. Hatha yoga has three basic components, postures (asanas), breathing techniques (pranayama) and meditation (dhyana). The postures started with stretching techniques followed by standing, supine and prone-lying and sitting postures [19]. Each pose was held for approximately 10-30 seconds with rest periods between poses lasting 30 seconds to one minute [19]. Exercise started with a light music. There was an emphasis on breathing for concentration and relaxation during the session. Each session ended with a 10-minute deep relaxation. Practice in home was strongly encouraged. Participants’ were given a pamphlet indicating the specific poses to aid in their home practice. The yoga class was set up in a sport facility or gym near the hospital and supervised by a nurse and neurologist. All poses were planned based on individual needs [20].
The patients of control group (n=30) received no intervention. The yoga exercise was performed with the assistance of trained individuals under the supervision of one of the author in the sports hall of the university. The study instrument was a questionnaire consisting of six sections: the first section for individual and disease characteristics including place of residence and economic status, the second section, Spielberg Anxiety Inventory, consisting of 20 items. The anxiety was measured before and after the intervention, with 20 representing the lowest and 80 the highest level of anxiety. The third section concerned with physiological indices (blood pressure, respiration, pulse rate, and temperature). The fourth section was Bayer numerical scale to measure pain, including a graph ranging from 0 (the lowest level) to 10 (the highest level) plotted by pain intensity. The scientific authenticity was determined by content validity and reliability of measures was derived 0.95 by Cronbach’s alpha. For scientific reliability [15], sphygmomanometer, stethoscope, and thermometer used at both steps of the study were reliable and their accurate functioning was already checked. In addition, Rotten Fatigue Severity Scale was administered to measure fatigue intensity. This scale contains nine statements that rate the severity of fatigue symptoms by seven-point Likert Scale [10].
The sixth section of the questionnaire was QOL questionnaire SF-36 investigating QOL in terms of physical, mental, psychological, and social domains. The validity and reliability of Persian version of the used questionnaire have been already reported as satisfactory. The content validity of the questionnaire was confirmed by 10 faculty members of Department of Nursing and Midwifery. For reliability, the correlation coefficient was calculated as 0.91 [19]. The QOL questionnaire was administered at two steps: prior to study and 12 weeks after completion of the study. To obtain the patients’ consent to participate in the study, we completely explained the study purposes for them and then asked them to fill out the relevant letter of consent. Moreover, the patients were ensured that all study data are kept by the researcher as confidential and used only for research purposes. Author-administered instruments and all study procedures were monitored by a neurologist. All testing was performed and the data were analysed by the individuals blind to the group of patients.
This study obtained ethical approval no. 87-1-2 from Ethics Committee of Shahrekord University of Medical Sciences and the code IRCT2013063013768N2 from Iranian Registry of Clinical Trials. The study’s data were analysed by SPSS 18 using descriptive {mean and Standard Deviation (SD)} and analytical statistics such as independent t-test, paired t-test, and one-way ANOVA. For all tests, p<0.05 was considered as the level of significance.
Results
In this study mean age of the patients in both case and control groups was 30 years. All patients received insurance services. For economic status, most patients reported a moderate economic status [Table/Fig-2].
Demographics characteristics of study population.
| Variable | Case group | Control group |
|---|
| Marital status | % | No. | % | No. |
|---|
| Single | 3 | 15 | 2 | 10 |
| Married | 17 | 85 | 18 | 90 |
| Total | 20 | 100 | 20 | 100 |
| Custody |
| Yes | 17 | 85 | 18 | 90 |
| No | 3 | 15 | 2 | 10 |
| Total | 20 | 100 | 20 | 100 |
| Education level |
| Preliminary | 5 | 25 | 4 | 20 |
| Guidance | 5 | 25 | 5 | 25 |
| High school | 8 | 40 | 9 | 45 |
| Academic | 2 | 10 | 2 | 10 |
| Total | 20 | 100 | 20 | 100 |
| Employment |
| Housewife | 18 | 90 | 18 | 90 |
| Employed | 2 | 10 | 2 | 10 |
| Total | 20 | 100 | 20 | 100 |
| Insurance Services |
| Yes | 20 | 100 | 20 | 100 |
| No | - | - | | |
| Total | 20 | 100 | 20 | 100 |
| Economic status |
| Poor | 4 | 20 | 2 | 10 |
| Moderate | 14 | 70 | 16 | 80 |
| Good | 2 | 10 | 2 | 10 |
| Total | 20 | 100 | 20 | 100 |
Mean score of QOL of the patients before the study was 1533±759.10 in the case group and 1385.75±600.04 in the control group. There was no significant difference in mean score of QOL between the two groups before the study, but the difference in mean score of QOL between the two groups was significant after the intervention, so that the mean score of QOL and social functioning of the patients was higher in the case group than the control group [Table/Fig-3].
Mean score of quality of life of patients before and after intervention in case and control groups.
| Group | Mean score of quality of life of patients before and after intervention | p-value |
|---|
| case group | Before intervention | 1533±759.10 | <.05 |
| After intervention | ± 540.76 2446 |
| Intra-group p-value | <.05 |
| Control group | Before intervention | 1385/75±600.04 |
| After intervention | 1255.75±600.22 |
| Intra-group p-value | <.05 |
In addition, the study findings indicated that there was no significant difference in fatigue intensity between the two groups before intervention, but fatigue intensity decreased in case group compared to the control group after the intervention [Table/Fig-4].
Mean score of anxiety of patients before and after intervention in case and control groups.
| Group | Anxiety | Mean | Standard deviation | t | p-value |
|---|
| Case | Before and after | 3.3 | 5.63 | 3.4 | <0.05 |
| Control | Before and after | 3.9 | 4.4 | 4.6 | >0.05 |
t-test indicated no significant difference in mean physiological indices (pulse rate, blood pressure, temperature, and respiratory rate) between the two groups (before the study). But a significant difference was derived in mean physiological indices of case group between before and after the intervention so that pulse rate and blood pressure decreased significantly in case group after the intervention but no change in physiological indices (pulse rate, blood pressure, respiration, and temperature) was derived in the control group. In addition, study findings indicated no significant difference in mean score of anxiety between case and control groups before the intervention. But, mean score of anxiety exhibited a significant difference between the two groups after the intervention (p<0.05), so that anxiety level declined in case group. But, in the control group, no statistically significant difference in anxiety level was seen between before and after the intervention [Table/Fig-5].
Mean score of pain of patients before and after intervention in case and control groups.
| Pain severity | Pain (before intervention) |
|---|
| Very low | Low | Moderate | Severe |
|---|
| Group | Numbers (%) | Numbers (%) | Numbers (%) | Numbers (%) |
|---|
| case | 3(15) | 5 (25) | 9 (45) | 3 (15) |
| Control | 3(15) | 6(30) | 10(50) | 1(5) |
| t-test result | p-value > 0.05 |
| Pain severity | Pain (after intervention) |
| Very low | Low | Moderate | Severe |
| Group | Number (%) | Number (%) | Number (%) | Number (%) |
| case | 4 (20) | 6 (30) | 10 (50) | 0 (0) |
| Control | 3 (15) | 7 (35) | 7 (35) | 3 (15) |
| t-test result | p-value < 0.05 |
Discussion
As a chronic and progressive disease of neurological system, MS adversely affects social functioning, anxiety, pain intensity, fatigue, and QOL of the patients. Several studies have demonstrated lower level of QOL in MS patients than other patients [21]. The present study indicated that practicing programmed yoga exercise could significantly enhance social functioning of MS patients. Consistent with the present study, Najafi Doulatabad et al., study indicated that yoga caused improvement of general health, social functioning, and life expectancy in MS patients [5]. Another study has investigated yoga exercise effect on cognitive functioning, fatigue, pain intensity, mood, and QOL in the MS patients. The findings indicated that yoga exercise caused improvement of cognitive functioning and QOL in these patients [22]. Yoga is known as an exercise with lowest complications which has been addressed in India since thousands of years ago. This exercise is aimed to reach maximum coordination of body, mind, and soul [23]. The positive contribution of yoga in enhancing social functioning and QOL of the patients could be attributed to its effect on relieving mental and physical stress, increasing physical and motor strength and piece, and eliminating fatigue. Since MS has a chronic, progressive course and leads to physical, mental, economic, and social disabilities of the patients over time, they they grow isolated and depressed leading to divorce and disintegration in many families and finally probably to suicide in many suffering patients. Therefore, use of easy, inexpensive, and practical approaches could assist the MS patients in returning to the community and coping with the conditions. Consistently, yoga exercise has a positive contribution to skeletal system and leads to nervous-muscular and physical, mental balance. Moreover, yoga exercise effects on QOL and overall functioning by enhancing coping capability of psychological, nervous, immunity, and cognitive systems [24,25]. The findings have indicated that QOL and socioeconomic status are directly correlated [26].
The present study findings indicated that yoga led to relief of pain and anxiety of the patients. Consistent with the present study, Tarakci et al., indicated that regular group exercise caused improvement of functioning and balance, reduction of muscular spasms and fatigue, and relative promotion of QOL [25]. In addition, the findings of other studies indicated that short-term yoga exercises contributed greatly to low back pain, body flexibility, relief of stress and anxiety, and social and physical functioning [27]. Cornelissen et al., findings regarding the usefulness of yoga and meditation in the short-term reduction of anxiety are inconsistent with the present study [28]. However, some studies have shown a significant decline compared to baseline in participants’ anxiety scale after intervention [29]. However, the results suggest the beneficial effects of yoga for relieving anxiety in cancer patients [30]. There have been significant differences in psychological parameters (e.g., aggressiveness, excitability, somatic complaints) between the yoga practitioners, scoring higher on these measures, and the controls. In addition, the control group was more likely to respond to stress with anger than the yoga group [31]. These results suggest the possibility of long-term psychological benefits and short-term changes in coping response to stress resulting from yoga practice.
The mean physiological indices (systolic and diastolic blood pressure, pulse rate, respiration, and temperature) of patients exhibited no statistically significant difference between the case and control groups before the study, but yoga resulted in decreased blood pressure and pulse rate in the case group after the study; however, no change in physiological indices was seen in the control group. Another study demonstrated that the mean physiological indices (systolic and diastolic blood pressure, pulse rate, respiration, and temperature) exhibited no statistically significant difference before the study [32], but training programs reduced systolic blood pressure significantly and to a similar extent. Finally, the effect of training on heart rate at rest, during exercise and recovery was more pronounced with higher intensity training [32]. As previously reported, a significant increase of VO2 peak was observed after training [28]. The effects of improved fitness on blood pressure, heart rate and heart rate variability could, therefore, be examined in the present study. Fagard and Cornelissen observed an immediate reduction in blood pressure after a single bout of exercise [29].
Conclusion
The studies suggest that yoga as a supplement to pharmacotherapy may improve stress and anxiety symptoms. As a chronic disease, MS could decline social functioning and QOL, and increase pain, fatigue, and anxiety in the patients. The present study findings indicated that yoga exercise caused social functioning and QOL of the MS patients to enhance. Yoga is likely to contribute to increasing self-efficacy and ultimately promoting social functioning and QOL of the patients with MS through enhancing physical activity, strength of lower limbs’ muscles, and balance and relieving fatigue and pain. Exercising yoga is very simple and carries very little probability of damage and can be done in many places including home and workplace. In view of the present study findings, the arrangements should be made for MS patients so that they can easily access sports facilities. Officials should help MS patients for employment because the more economically independent they are, the better they can participate in social, sports, and recreational activities. In addition, employment might lead to increased self-esteem and consequently life expectancy in MS patients. The use of yoga may be considered as a possible adjunctive therapy for those experiencing stress and anxiety. Due to its good compliance and lack of drug interactions, yoga appears to be safe and could be encouraged to improve QOL and, perhaps, the symptoms of stress and anxiety.
[1]. Koch-Henriksen N, Sorensen PS, The changing demographic pattern of multiple sclerosis epidemiologyLancet Neurol 2010 9(5):520-32. [Google Scholar]
[2]. Latimer-Cheung AE, Pilutti LA, Hicks AL, Martin Ginis KA, Fenuta AM, MacKibbon KA, Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults with multiple sclerosis: a systematic review to inform guideline developmentArch Phys Med Rehabil 2013 94(9):1800-28 e3. [Google Scholar]
[3]. Hassanpour-Dehkordi A, Jivad N, Comparison of regular aerobic and yoga on the quality of life in patients with multiple sclerosisMed J Islam Repub Iran 2014 28:141 [Google Scholar]
[4]. Elhami SR, Mohammad K, Sahraian MA, Eftekhar H, A 20-year incidence trend (1989-2008) and point prevalence (March 20, 2009) of multiple sclerosis in Tehran, Iran: a population-based studyNeuroepidemiology 2011 36(3):141-47. [Google Scholar]
[5]. Najafi Doulatabad SH, Nouryan KH, Malekzadeh GM, Ghaem H, Roozitalab M, Afraseyabifar A, Effect of yoga exercise on general health status (ghs) and sense of life in patients with multiple sclerosisArmaghan-e-Danesh 2011 16(3):245-53. [Google Scholar]
[6]. Dehkordi A, Heydarnejad MS, Fatehi D, Quality of life in cancer patients undergoing chemotherapyOman Med J 2009 24(3):204-07. [Google Scholar]
[7]. Dehkordi AH, Heydarnejad MS, Factors-related to quality of life in post myocardial infarction patientsHain Med Col 2009 7:010 [Google Scholar]
[8]. Heydarnejad MS, Hassanpour DA, Solati DK, Factors affecting quality of life in cancer patients undergoing chemotherapyAfr Health Sci 2011 11(2):266-70. [Google Scholar]
[9]. Motl RW, McAuley E, Snook EM, Gliottoni RC, Physical activity and quality of life in multiple sclerosis: intermediary roles of disability, fatigue, mood, pain, self-efficacy and social supportPsychol Health Med 2009 14(1):111-24. [Google Scholar]
[10]. Wood B, van der Mei IA, Ponsonby AL, Pittas F, Quinn S, Dwyer T, Prevalence and concurrence of anxiety, depression and fatigue over time in multiple sclerosisMult Scler 2013 19(2):217-24. [Google Scholar]
[11]. Nick ST, Roberts C, Billiodeaux S, Davis DE, Zamanifekri B, Sahraian MA, Multiple sclerosis and painNeurol Res 2012 34(9):829-41. [Google Scholar]
[12]. Henriksson F, Fredrikson S, Masterman T, Jonsson B, Costs, quality of life and disease severity in multiple sclerosis: a cross-sectional study in SwedenEur J Neurol 2001 8(1):27-35. [Google Scholar]
[13]. Bahraini S, Naji S, Mannani R, Bekhradi R, The comparison of the effects of effleurage massage with aromatic oil and non-aromatic oil on fatigue severity in women with multiple sclerosisJ Urmia Nurs Midwifery Faculty 2011 9(5) [Google Scholar]
[14]. McCullagh R, Fitzgerald AP, Murphy RP, Cooke G, Long-term benefits of exercising on quality of life and fatigue in multiple sclerosis patients with mild disability: a pilot studyClin Rehabil 2008 22(3):206-14. [Google Scholar]
[15]. Heydarnejad S, Dehkordi AH, The effect of an exercise program on the health-quality of life in older adults. A randomized controlled trialDan Med Bull 2010 57(1):A4113 [Google Scholar]
[16]. Kargarfard M, Eetemadifar M, Mehrabi M, Maghzi AH, Hayatbakhsh MR, Fatigue, depression, and health-related quality of life in patients with multiple sclerosis in Isfahan, IranEur J Neurol 2012 19(3):431-37. [Google Scholar]
[17]. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteriaAnn Neurol 2011 69(2):292-302. [Google Scholar]
[18]. Hasanpour Dehkordi A, SalehiTali S, Frouzandeh N, Naderipour A, Ganjei F, Kasiry K, The effect of progressive muscle relaxation on anxiety and stress in nursing students at the beginning of the internship programJ Shahrekord Univ Med Sci 2009 11(1):71-77. [Google Scholar]
[19]. Hassanpour Dehkordi A, Khaledi Far A, Effect of exercise training on the quality of life and echocardiography parameter of systolic function in patients with chronic heart failure: a randomized trialAsian J Sports Med 2015 6(1):e22643 [Google Scholar]
[20]. Ahmadi A, Arastoo AA, Nikbakht M, Zahednejad S, Rajabpour M, Comparison of the Effect of 8 weeks Aerobic and Yoga Training on Ambulatory Function, Fatigue and Mood Status in MS PatientsIran Red Crescent Med J 2013 15(6):449-54. [Google Scholar]
[21]. Oken BS, Kishiyama S, Zajdel D, Bourdette D, Carlsen J, Haas M, Randomized controlled trial of yoga and exercise in multiple sclerosisNeurology 2004 62(11):2058-64. [Google Scholar]
[22]. Rafeeyan Z, Azarbarzin M, Moosa FM, Hasanzadeh A, Effect of aquatic exercise on the multiple sclerosis patients’ quality of lifeIran J Nurs Midwifery Res 2010 15(1):43-47. [Google Scholar]
[23]. Velikonja O, Curic K, Ozura A, Jazbec SS, Influence of sports climbing and yoga on spasticity, cognitive function, mood and fatigue in patients with multiple sclerosisClin Neurol Neurosurg 2010 112(7):597-601. [Google Scholar]
[24]. Smith C, Hancock H, Blake-Mortimer J, Eckert K, A randomised comparative trial of yoga and relaxation to reduce stress and anxietyComplement Ther Med 2007 15(2):77-83. [Google Scholar]
[25]. Tarakci E, Yeldan I, Huseyinsinoglu BE, Zenginler Y, Eraksoy M, Group exercise training for balance, functional status, spasticity, fatigue and quality of life in multiple sclerosis: a randomized controlled trialClin Rehabil 2013 27(9):813-22. [Google Scholar]
[26]. Hekmatpou D, Jahani F, Behzadi F, Study the quality of life among elderly women in Arak in 2013Arak Med Univ J 2014 17(83):1-8. [Google Scholar]
[27]. Tekur P, Singphow C, Nagendra HR, Raghuram N, Effect of short-term intensive yoga program on pain, functional disability and spinal flexibility in chronic low back pain: a randomized control studyJ Altern Complement Med 2008 14(6):637-44. [Google Scholar]
[28]. Cornelissen VA, Arnout J, Holvoet P, Fagard RH, Influence of exercise at lower and higher intensity on blood pressure and cardiovascular risk factors at older ageJ Hypertens 2009 27(4):753-62. [Google Scholar]
[29]. Fagard RH, Cornelissen VA, Effect of exercise on blood pressure control in hypertensive patientsEur J Cardiovasc Prev Rehabil 2007 14(1):12-17. [Google Scholar]
[30]. Banerjee B, Vadiraj HS, Ram A, Rao R, Jayapal M, Gopinath KS, Effects of an integrated yoga program in modulating psychological stress and radiation-induced genotoxic stress in breast cancer patients undergoing radiotherapyIntegr Cancer Ther 2007 6(3):242-50. [Google Scholar]
[31]. Li AW, Goldsmith CA, The effects of yoga on anxiety and stressAltern Med Rev 2012 17(1):21-35. [Google Scholar]
[32]. Cornelissen VA, Verheyden B, Aubert AE, Fagard RH, Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variabilityJ Hum Hypertens 2010 24(3):175-82. [Google Scholar]