Detection of Salivary IgA Antibodies Against the HlyE Antigen as a Diagnosis of Typhoid Fever
Kai Ling Chin1, Nur Eliyana Mohd Redhuan2, Prabha Balaram3, Kia Kien Phua4, Eugene Boon Beng Ong5
1 PhD Student, Institute for Research in Molecular Medicine, Universiti Sains, Malaysia, 11800 Pulau Pinang, Malaysia.
2 PhD Student, School of Veterinary Medicine, Universiti Malaysia Kelantan, Kota Bharu, Kelantan, Malaysia.
3 Former Professor, Institute for Research in Molecular Medicine, Universiti Sains, Malaysia, 11800 Pulau Pinang, Malaysia.
4 Professor, Institute for Research in Molecular Medicine, Universiti Sains, Malaysia, 11800 Pulau Pinang, Malaysia.
5 Lecturer, Institute for Research in Molecular Medicine, Universiti Sains, Malaysia, 11800 Pulau Pinang, Malaysia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Eugene Boon Beng Ong, Institute for Research in Molecular Medicine, Universiti Sains Malaysia, 11800 Pulau Pinang, Malaysia.
E-mail: eugene@usm.my
Introduction
The Salmonella typhi (S. typhi) haemolysin E protein (HlyE) has been shown to be a sensitive and specific antigen for the detection of typhoid fever through the detection of anti-HlyE antibodies in sera. Saliva can also be a useful diagnostic fluid as it also contains antibodies against bacterial pathogens.
Aim
This study aims to evaluate the potential detection of salivary anti-HlyE antibodies as a diagnosis of typhoid fever.
Materials and Methods
Saliva was collected from acute typhoid patients (n=16) who presented at Hospital Universiti Sains Malaysia with prolonged fever of more than five days and were positive for S. Typhi blood culture. Saliva was also collected from convalescent typhoid patients (n=11), patients with other febrile fevers (n=15), and from healthy individuals (n=25). An ELISA was developed to detect the presence of IgA antibodies against HlyE in the saliva of typhoid patients.
Results
The acute typhoid group had a higher mean absorbance value of 1.496 compared to the convalescent typhoid (0.538), other febrile fevers (0.678), and healthy individuals (0.457) group.
Conclusion
This study demonstrated the utility of salivary anti-HlyE IgA antibody as a biomarker for the diagnosis of typhoid fever. Follow-up studies with a larger sample size will allow the optimization of the sensitivity and specificity of the assay. This non-invasive method can be useful for mass screening programs.
Salmonella, ELISA, Saliva
Introduction
Typhoid fever is caused by Gram-negative bacteria, Salmonella enterica subspecies enterica serovar Typhi (S. typhi). Asia was reported to have the highest estimated rate of typhoid fever especially in south-central and southeastern Asia including India, Pakistan, Bangladesh and Malaysia [1]. In 2010, the worldwide burden of typhoid fever was estimated to be 26.9 million [2]. The association between the introduction of disease and migration has long been recognized [3]. With increasing travel and migration patterns worldwide, typhoid outbreaks can possibly occur when carriers or convalescent individuals that had recently arrived in non-endemic areas engage in food preparation activities.
The blood culture method which has been in practice for nearly a century is the ’gold standard’ for diagnosis of typhoid fever but no major improvement in its detection rate is reported. This is probably due to the limitations of the test itself, such as false negatives in cases with prior antibiotic treatment, delay in time of sample collection i.e. not during the acute phase of infection, lack of expertise and culture facilities in low-resource settings, and the time required for confirmation of the bacteria [4]. Due to the drawback of the culture method, many rapid diagnostic tests such as Widal test, Typhidot™ and TUBEX™ were developed [4]. Although, these tests provided an alternative to the conventional culture method, they each have their own limitations such as inconsistent results in different geographical areas (Keddy et al., 2011; Fadeel et al., 2011; Mehmood et al., 2015) or a high positive rate due to shared antigenic determinants [5]. Hence, there is still a need for new assays that can help clinicians make accurate and timely diagnosis for typhoid fever.
Blood is the most frequently used bio-fluid in daily clinical and laboratory diagnosis. However, this invasive technique requires expert phlebotomist, correct blood collecting and handling procedures, and it is often problematic especially when sampling from young paediatric patients [6]. Studies show that saliva contains a plethora of putative proteins related to an infection and a major proportion of saliva consists of antibodies, i.e. secretory-immunoglobulin A (s-IgA) (90-98%), IgG (1-10%) and small fractions of IgM, IgD and IgE [7]. Thus, saliva can be used as an alternative to serum as a source of antigens for biomarker discovery, or as a diagnostic bio-fluid (in antibody-based tests) for infections including typhoid fever [8–14]. In addition, this non-invasive technique is rapid, economical, painless and safe compared to blood sampling, and thus has the potential to be used in point-of care-diagnostics in laboratories with minimal infrastructure [15], fulfilling WHO’s AAAQ criteria [16]: 1) Availability (a simple and convenient method for mass screening, does not require specialized personnel for collection, and can be used immediately after collection without processing); 2) Accessibility (suitable for high risk groups, i.e. children and the elderly, and during epidemic outbreaks); 3) Acceptability (non-invasive, painless, and non-hazardous); and 4) Quality (sensitive and specific).
Current studies to identify new biomarkers for typhoid fever using various proteomic approaches, such as microarray, immunoaffinity proteomics-based technology and mass spectrometry have showed that HlyE is an important antigen in typhoid fever [17–19]. A previous study by our group using the recombinant haemolysin E (rHlyE) protein from S. typhi showed the usefulness of this antigen in the detection of typhoid fever with a sensitivity of 70%, and a specificity of 100% [20]. The sensitivity of the test is comparable to current available diagnostic tests for typhoid fever. Taking into consideration the limitations of serodiagnostic techniques, this preliminary study aims to evaluate the potential detection of salivary IgA antibody against the S. Typhi rHlyE antigen using an indirect ELISA for diagnosis of typhoid fever. When developed, such an assay would provide an alternative to diagnose typhoid fever in a non-invasive, rapid manner and can lend itself to mass screening programs during an outbreak.
Materials and Methods
Samples
Human saliva used was obtained from the Institute for Research in Molecular Medicine (INFORMM), Universiti Sains Malaysia (USM), Malaysia. Individual samples were collected in accordance with the guidelines approved by the Human Ethical Committee of USM in the year 2010. Acute typhoid (n=16) were patients who had fever for more than five days and were positive for S. Typhi blood culture. Convalescent typhoid (n=11) were typhoid fever patients who had recovered within one year post-infection. Other febrile fever subjects (n=15) were patients who had prolonged fever but were negative for S. typhi blood culture. Healthy normal individuals (n=25) were volunteers who did not have a history of typhoid fever and had no symptoms of any other infection at the time of sample collection. All participants’ saliva was collected as described previously [21]. Participants rinsed their mouth by gargling at least three times with distilled water before drooling 3-5 ml of saliva into sterile containers. The salivary samples were centrifuged at 13,000 g and the supernatants were stored in aliquots at -20°C until use in ELISA.
Elisa
The rHlyE antigen was purified and ELISA was performed as previously described [20,22]. Briefly, each well on the ELISA plate (Greiner Bio-One, Belgium) was coated with 100 μl/well of 0.5 μg purified rHlyE antigen (diluted in 50 mM carbonate/bicarbonate buffer, pH 9.6) overnight at 4°C. After removing the antigen solution, the plate was washed thrice with PBS-T (phosphate-buffered saline with 1% Tween 20). The plate was then blocked by adding 200 μl/well of blocking buffer (PBS with 5% skim milk) which was incubated for one hour at 37°C. After removing the blocking solution, the plate was washed thrice with PBS-T as before. One hundred microliters of saliva (undiluted) to be tested was added to each well (in duplicate). For each plate, positive and negative serum controls diluted in PBS-T buffer (1:100) were also added. After incubation for one hour at 37°C, the plate was washed thrice and 100 μl/well of peroxidase-labeled goat anti-human IgA conjugate (Sigma-Aldrich, USA) diluted 1:1000 in PBS-T was added. After incubation for one hour, a final washing step was carried out and 100 μl of 2,2′-Azino-bis(3-ethylbenzothiazoline-6-sulfonic acid) diammonium salt (ABTS) solution was added into each well. The plate was incubated at 37°C for 30 minutes before absorbance (OD405) was measured with a microplate reader (SpectraMax® Microplate Reader, Molecular Devices, USA). The cut off value was the midpoint between the mean absorbance of the typhoid positive saliva and the mean absorbance of healthy normal controls [9].
Results
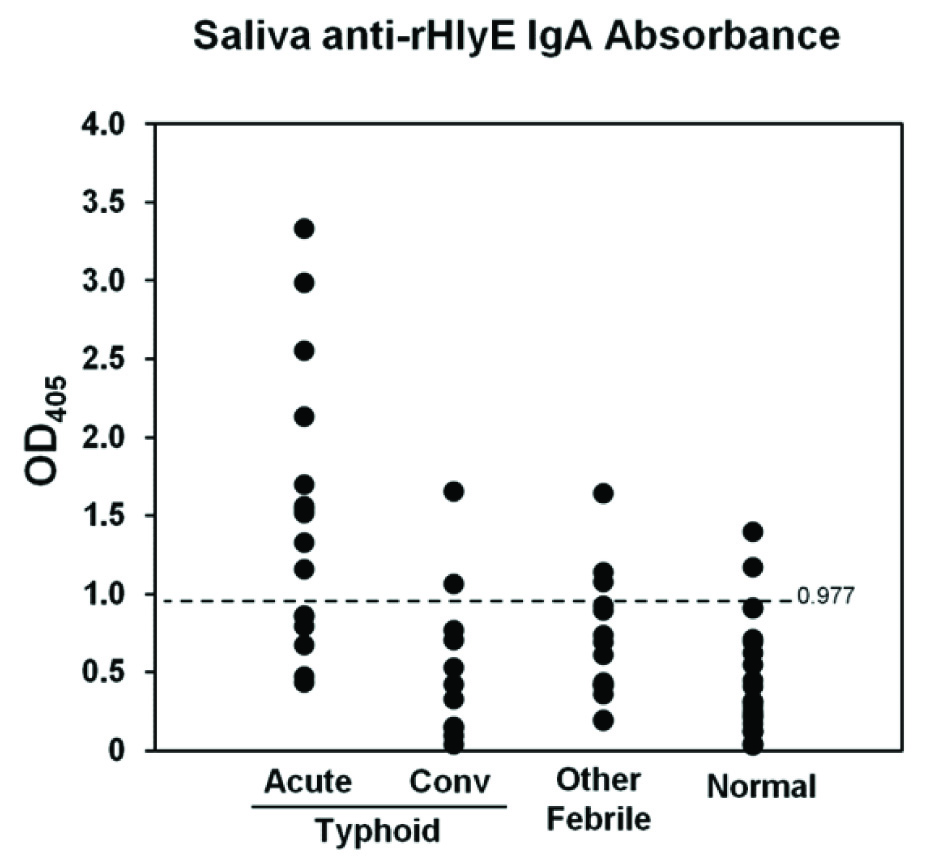
In this study, the results of haemoculture were referenced as the gold standard. The ELISA results showed a clear distinction between acute typhoid samples compared to the convalescent, other febrile and normal samples that were tested [Table/Fig-1]. The positive cut off titer for salivary IgA antibodies was 0.977. Ten of the 16 saliva samples from acute haemoculture confirmed cases were IgA ELISA positive. The acute typhoid group had a mean absorbance value of 1.496, which was approximately thrice the mean absorbances of the convalescence (0.538) and normal (0.457) groups, and twice that of the other febrile group (0.678). This showed the potential of salivary anti-rHlyE IgA antibody in diagnosis of acute typhoid fever as it enables early diagnosis of the infection in the acute stage.
Reactivity of IgA antibody present in typhoid (acute and convalescent), other febrile fevers and normal individuals’ saliva to rHlyE. Absorbance values of salivary anti-rHlyE IgA in an ELISA from ABTS absorbance (OD405) readings were taken from the average of duplicates. The dotted horizontal line represents the cut off titer of 0.977. The absorbance values that were used to derive the scatter dot graph are presented in the Supplementary Information.
Discussion
Till date, only two studies had been carried out to evaluate the usefulness of salivary IgA against S. typhi lipopolysaccharide (LPS) for the detection of typhoid fever [9,23]. In those studies, serial samples were collected during patients’ follow-up to determine the time frame of antibody production against LPS using ELISA. The authors in both the studies found that the anti-LPS IgA antibodies reached their peak during the second and third week of typhoid fever and subsequently decreased drastically in the following weeks. This corresponds to the overall absorbance pattern of the typhoid group in our study which showed higher absorbance values during the acute stage but subsequently reduced during the convalescent stage.
The immune system represents a remarkable mechanism of producing large amounts of antibodies against foreign antigens. Individual response to S. typhi in differing magnitudes and durations were multifactorial depending on the size of bacterial inoculum, our personal immune systems and perhaps previous exposure to the disease (especially populations in endemic areas). Also, the incubation period for typhoid fever is considerably longer than other diseases. Thus, the negatives observed in acute typhoid and the positives observed in convalescent typhoid individuals could be due to miscalculation of the stage of the disease when the patients presented themselves. It was also reported that 10% of the individuals convalescing from acute typhoid will become a convalescent or temporary carrier, 1-4% become chronic carriers and most relapses occurred at this stage at a rate of 5-10% [24]. However, this assumption could not be ascertained as follow-up on the two false positive patients were not conducted to eliminate their possibility as carriers.
Other febrile patients (n=15) that was diagnosed as other than typhoid fever was determined to be dengue (n=11), hepatitis, infective endocarditis, leptospirosis, and viral fever. The three other febrile patients with absorbance values higher than the cut off value were all dengue patients. A previous study reported that patients with dengue not only show similar signs and symptoms of infection with typhoid fever, but also a possibility of co-infection with typhoid fever [25]. These could have caused misdiagnosis and the cause of the disease overlooked if clinicians do not perform differential diagnosis to rule out other possibilities. All the normal individuals (n=25) showed absorbance values lower than the cut off value except for three samples. The false positive results observed in this study could not be clearly explained at this juncture. This was also observed in a previous study, whereby a normal individual who was excluded as a typhoid carrier based on stool culture showed a consistently high prolonged salivary anti-LPS IgA antibody level throughout a 120 day period [9].
Differences in types and profiles (quantity and quality) of antibodies are reported at difference stages of typhoid infection. For example, the serum antibody levels against O- and H-antigens in Widal test are low at the first week of illness but begin to rise subsequently between second to third weeks before declining subsequently [26]. In future, follow-up studies on each individual need to be carried out to determine the salivary anti-rHlyE IgA antibody profiles. Also, to obtain a better picture of the diagnostic value of the assay, a larger sample size of clinical typhoid samples (both haemoculture positive acute samples and haemoculture negative samples) need to be included. These will help determine the diagnostic sensitivity and specificity of the assay at different stages of infection and to overcome the limitation of the sensitivity of the blood culture method.
Conclusion
This preliminary study showed that salivary IgA antibody against rHlyE could be a good biomarker to detect immune responses during typhoid infection. Saliva contains a plethora of components and can be used as an alternative bio-fluid for diagnosis, fulfilling WHO’s AAAQ criteria. It is suitable for mass screening due to its non-invasive nature, ease of collection and acceptability among high risk patients. With further optimization of the assay and a larger sample size validation trial, the salivary anti-rHlyE IgA antibody can serve as an antibody-based detection test for diagnosis of typhoid fever.
[1]. Crump JA, Luby SP, Mintz ED, The global burden of typhoid feverBull World Health Organ 2004 82(5):346-53. [Google Scholar]
[2]. Buckle GC, Walker CL, Black RE, Typhoid fever and paratyphoid fever: Systematic review to estimate global morbidity and mortality for 2010J Glob Health 2012 2(1):010401 [Google Scholar]
[3]. Gushulak BD, MacPherson DW, Globalization of infectious diseases: the impact of migrationClin Infect Dis 2004 38(12):1742-48. [Google Scholar]
[4]. Keddy KH, Sooka A, Ismail H, Smith AM, Weber I, Letsoalo ME, Molecular epidemiological investigation of a typhoid fever outbreak in South Africa, 2005: the relationship to a previous epidemic in 1993Epidemiol Infect 2011 139(8):1239-45. [Google Scholar]
[5]. Verma D, Kishore S, Siddique ME, Comparative evaluation of various tests for diagnosis of concurrent malaria and typhoid Fever in a tertiary care hospital of northern IndiaJ Clin Diagn Res 2014 8(5):DC41-44. [Google Scholar]
[6]. Madar R, Straka S, Baska T, Detection of antibodies in saliva – an effective auxiliary method in surveillance of infectious diseasesBratisl Lek Listy 2002 103(1):38-41. [Google Scholar]
[7]. Fábián TK, Fejérdy P, Csermely P, Saliva in Health and Disease Wiley Encyclopaedia of Chemical Biology 2008 4(1st ed):1-9. [Google Scholar]
[8]. Fabian TK, Hermann P, Beck A, Fejerdy P, Fabian G, Salivary defense proteins: their network and role in innate and acquired oral immunityInt J Mol Sci 2012 13(4):4295-320. [Google Scholar]
[9]. Herath HM, Early diagnosis of typhoid fever by the detection of salivary IgAJ Clin Pathol 2003 56(9):694-98. [Google Scholar]
[10]. Pfaffe T, Cooper-White J, Beyerlein P, Kostner K, Punyadeera C, Diagnostic potential of saliva: current state and future applicationsClin Chem 2011 57(5):675-87. [Google Scholar]
[11]. Zhang A, Sun H, Wang P, Wang X, Salivary proteomics in biomedical researchClin Chim Acta 2013 415:261-65. [Google Scholar]
[12]. Al Kawas S, Rahim ZH, Ferguson DB, Potential uses of human salivary protein and peptide analysis in the diagnosis of diseaseArch Oral Biol 2012 57(1):1-9. [Google Scholar]
[13]. Malathi N, Mythili S, Vasanthi HR, Salivary diagnostics: a brief reviewISRN Dent 2014 2014:158786 [Google Scholar]
[14]. Mandel ID, The diagnostic uses of salivaJ Oral Pathol Med 1990 19(3):119-25. [Google Scholar]
[15]. Lee YH, Wong DT, Saliva: an emerging biofluid for early detection of diseasesAm J Dent 2009 22(4):241-48. [Google Scholar]
[16]. WHO WHO. The right to health. Joint Fact Sheet WHO. 2007;323 [Google Scholar]
[17]. Ansong C, Yoon H, Norbeck AD, Gustin JK, McDermott JE, Mottaz HM, Proteomics analysis of the causative agent of typhoid feverJ Proteome Res 2008 7(2):546-57. [Google Scholar]
[18]. Liang L, Juarez S, Nga TV, Dunstan S, Nakajima-Sasaki R, Davies DH, Immune profiling with a Salmonella typhi antigen microarray identifies new diagnostic biomarkers of human typhoidSci Rep 2013 3:1043 [Google Scholar]
[19]. Charles RC, Sheikh A, Krastins B, Harris JB, Bhuiyan MS, LaRocque RC, Characterization of anti-Salmonella enterica serotype Typhi antibody responses in bacteremic Bangladeshi patients by an immunoaffinity proteomics-based technologyClin Vaccine Immunol 2010 17(8):1188-95. [Google Scholar]
[20]. Ong EB, Ignatius J, Anthony AA, Aziah I, Ismail A, Lim TS, Multi-isotype antibody responses against the multimeric Salmonella typhi recombinant haemolysin E antigenMicrobiol Immunol 2015 59(1):43-47. [Google Scholar]
[21]. Nurkka A, Ahman H, Korkeila M, Jantti V, Kayhty H, Eskola J, Serum and salivary anti-capsular antibodies in infants and children immunized with the heptavalent pneumococcal conjugate vaccinePaediatr Infect Dis J 2001 20(1):25-33. [Google Scholar]
[22]. Ong EB, Anthony AA, Ismail A, Lim TS, Cloning, expression, and purification of the haemolysin/cytolysin (HlyE antigen) from Salmonella enterica serovar Typhi: potential application for immunoassay developmentDiagn Microbiol Infect Dis 2013 77(1):87-89. [Google Scholar]
[23]. Zaka-ur-Rab Z, Abqari S, Shahab T, Islam N, Shukla I, Evaluation of salivary anti-Salmonella typhi lipopolysaccharide IgA ELISA for serodiagnosis of typhoid fever in childrenArch Dis Child 2012 97(3):236-38. [Google Scholar]
[24]. Agarwal PK, Gogia A, Gupta RK, Typhoid FeverJ Indian Acad Clin Med 2004 5(1):60-64. [Google Scholar]
[25]. Sharma Y, Arya V, Jain S, Kumar M, Deka L, Mathur A, Dengue and Typhoid Co-infection- Study from a Government Hospital in North DelhiJ Clin Diagn Res 2014 8(12):DC09-11. [Google Scholar]
[26]. Begum Z, Ahsan MM, Begum A, Baten MA, M.M. A, Ahmed KGS, Value of the single Widal test in the diagnosis of typhoid feverComm Based Med J 2013 2(1):34-38. [Google Scholar]