‘Ubiquitous’ Tumour Elsewhere, But Uncommon in the Colon! Can We Ignore this Lesion?
Gabriel Rodrigues1
1 Professor, Department of General Surgery, Kasturba Medical College, Manipal University, Manipal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gabriel Rodrigues, Professor, Department of General Surgery, Kasturba Medical College, Manipal University, Manipal-576104, India.
E-mail: gabyrodricks@gmail.com
Lipoma, a benign tumour of mature fat cells, can occur anywhere in the body and hence termed ’ubiquitous tumour’. But it rarely occurs in the colon and can present with complications and mimic malignancy. We present a case of descending colonic lipoma which led to a diagnostic dilemma.
Lipoma, Obstruction, Surgery
Case Report
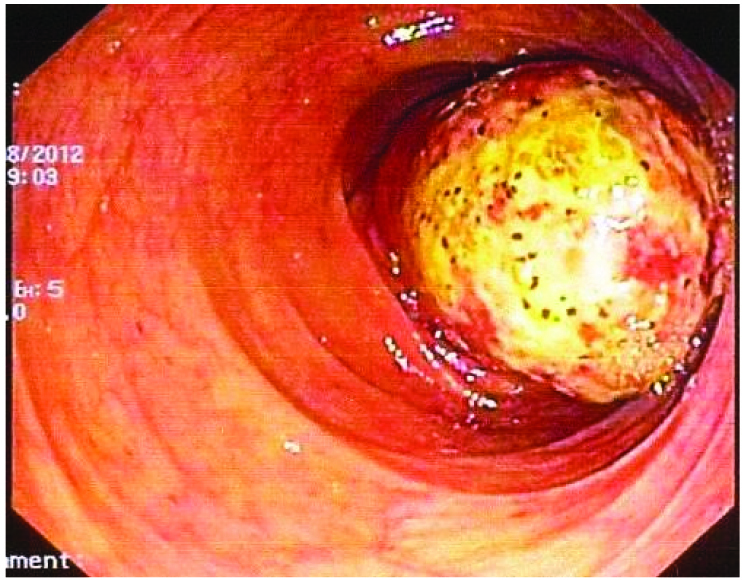
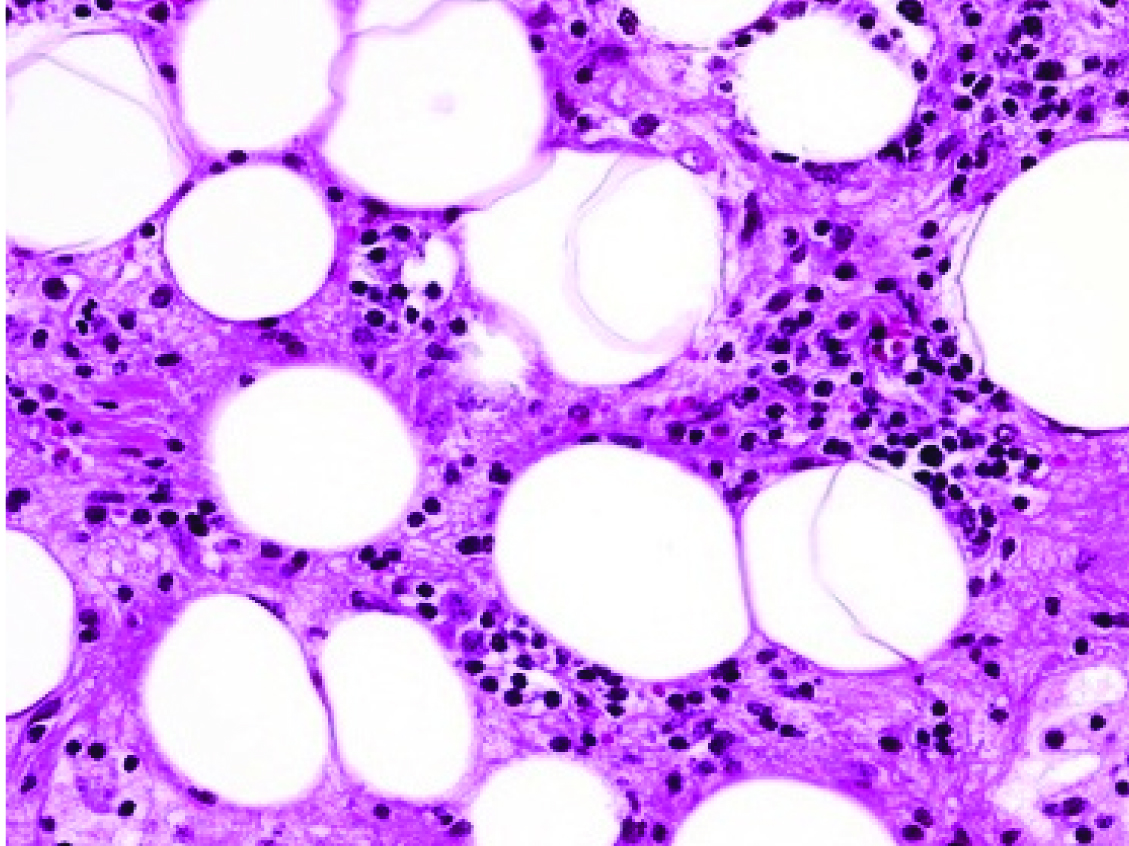
A 72-year-old male with no co-morbidities was admitted with the history of obstipation, generalized abdominal distension and vomiting of three days duration. There was no similar history in the past. General examination was not contributory except for mild dehydration. Per abdomen evaluation revealed generalized gaseous distension with absent bowel sounds. There was no tenderness, guarding, mass or free fluid. All blood investigations were normal and an erect abdominal X-ray revealed multiple air fluid levels up to the terminal ileum indicating a distal bowel obstruction. Due to financial constraints, an abdominal CT scan could not be done. Colonoscopy revealed a smooth, rounded, lesion totally obstructing the lumen of the descending colon [Table/Fig-1]. A biopsy was performed but as the patient was in total obstruction, he was taken up for an emergency exploratory laparotomy. Intraoperatively, the entire bowel was dilated up mid jejunum. A hard impacted mass was felt in the mid-descending colon with no serosal involvement; hence a right radical hemicolectomy was performed considering his age and a provisional clinical diagnosis of carcinoma. The histopathological diagnosis was suggestive of a pedunculated lipoma [Table/Fig-2].
Colonoscopic view of the descending colon mass.
Photomicrograph showing mature adipose tissue cells, H&E X40.
Discussion
Lipoma is the most common benign tumour of the human body which occurs in most of the organs and hence termed as a ’ubiquitous’ tumour. But lipomas of the gastrointestinal tract are rare conditions first described by Baurer in 1757. It is the second most common benign tumour of the colon after adenomas [1–3]. Females are affected more commonly and become symptomatic between 50 and 65 years. Right colon is commonly affected (61%), followed by left colon (20.1%), transverse colon (15.4%) and rectum (3.4%) [4]. They are usually submucosal and asymptomatic but may cause bleeding, obstruction, intussusception, or abdominal pain [1]. Accurate preoperative diagnosis is difficult and is often mistaken for adenomatous polyps or carcinoma. Though an abdominal CT scan usually indicates the diagnosis, it can only be confirmed by a colonoscopy and biopsy [5]. While small asymptomatic submucosal lipomas can be managed conservatively, large or pedunculated ones can be dealt either endoscopically or by surgery [6]. Though a colotomy and lipectomy has been described previously, many surgeons’ prefer to do either a segmental resection or a hemicolectomy [3]. In an emergency setting, especially when patient is in total obstruction and not responding to conservative management, emergency surgery has to be performed to relieve the obstruction. The decision of extent of bowel resection can be made only ’on table’, especially when a preoperative CT scan has not been performed. In patients with subacute intestinal obstruction, it is worthwhile to obtain a histopathological report to decide on the extent of surgery.
Conclusion
Colonic lipomas are rare and can present as acute intestinal obstruction. Abdominal CT scan usually indicates the diagnosis, but can only be confirmed by a colonoscopy and biopsy. In an acute setting, laparotomy and bowel resection has to be performed. Prognosis is good in these patients.
[1]. Lee CS, Lee MJ, Kim KL, Kim YS, Baik GH, Kim JB, A case of giant lipoma causing chronic recurrent intussusception of the colonClin Endosc 2012 45:165-68. [Google Scholar]
[2]. Presti ME, Flynn MF, Schuval DM, Vollmar TM, Zotos VD, Colonic lipoma with gastrointestinal bleeding and intussusceptionACG Case Rep J 2015 2:135-36. [Google Scholar]
[3]. Grasso E, Guastella T, Giant submucosal lipoma cause colo-colonic intussusception. A case report and review of literatureAnn Ital Chir 2012 83:559-62. [Google Scholar]
[4]. Huh KC, Lee TH, Kim SM, Im EH, Choi YW, Kim BK, Intussuscepted sigmoid colonic lipoma mimicking carcinomaDig Dis Sci 2006 51:791-95. [Google Scholar]
[5]. Ghanem OM, Slater J, Singh P, Heitmiller RF, DiRocco JD, Pedunculated colonic lipoma prolapsing through the anusWorld J Clin Cases 2015 3:457-61. [Google Scholar]
[6]. Toumi O, Hellara O, Hammami M, Mahmoudi A, Nasr M, Kallel W, Colo-colonic intussusception secondary to a colonic lipoma: report of two casesTunis Med 2014 92:700-01. [Google Scholar]