Non-surgical endodontic treatment is routinely practiced in modern dentistry. Revolution of material science and techniques in root canal treatment has resulted in the retention of millions of teeth that would have otherwise been lost. Even as recent advances in surgical, prosthetic and restorative care have made tooth replacement less onerous than in the past, it is universally accepted that a natural tooth with a good prognosis is a superior choice to loss and replacement [1].
Retreatment is a procedure to remove root canal filling material from the tooth, followed by cleaning, shaping and obturation of the canals [2].
Complete removal of gutta-percha from root canal walls, re-establishing working length, promoting disinfection and re-obturating the root canal are the main goals of non-surgical retreatment to re-establish healthy periapical tissues and obtain predictable success [3].
Several techniques have been proposed to remove filling materials from root canal system, including the use of endodontic hand files, Nickel Titanium rotary instruments, Gates Glidden burs, heated instrument, ultrasonic instruments, laser, and use of adjunctive solvents. Conventionally, the removal of gutta percha using hand files with or without solvent can be a tedious, time consuming process especially when the root filling material is well compacted [4].
When endodontic retreatment is performed, irritants in the form of filling materials, necrotic pulp, bacteria or irrigant might be introduced into the apical region. Apical extrusion of debris produced in endodontic treatment and retreatment might lead to post-operative pain and discomfort. These apically extruded materials have been held clinically responsible for post-operative inflammation and flare ups eventually leading to failure of apical healing [5].
Retreatment is a tedious and time consuming process leading to many procedural errors. Selecting the case for retreatment is a meticulous process where the pros and cons of tooth prognosis have to be weighed. So duration of time plays an important role in selecting the case.
The aim of the study was to evaluate and compare the effective removal of gutta percha and sealer from the root canals, amount of apical debris extrusion and the time required for gutta-percha removal using various endodontic files.
Materials and Methods
The present study was carried out in the Department of Conservative Dentistry and Endodontics at JSS Dental College, Mysore from April 2015 to September 2015 after the approval by the ethical committee of the institute.
Specimen Preparation: Based on previous studies conducted in a similar manner, a sample size of 48 human mandibular premolar teeth showed statistically significant results. The premolars which were extracted for orthodontic purpose were used. External surface of teeth were cleaned to remove debris and soft tissue remnants and were stored in normal saline solution. Teeth with single root canal with type 1 canal configuration, root curvature of 0° - 10° were taken and were evaluated by using RVG. Samples with multiple canals, cracks, internal resorption, external resorption, root caries, calcification and open apices were excluded.
Intial Endodontic Treatment: After access cavity preparation, apical patency was confirmed and working length was established 1mm shorter than the length at which a size 15 K-file was visualized at the apical foramen. Root canals were prepared using step back technique and enlarged upto a size 40 K file. After each instrumentation, the canals were irrigated with 2ml 1% sodium hypochlorite using 27 gauge needle then with normal saline, later 17% EDTA was applied for 3min and the canals were finally flushed with normal saline.
All samples were dried with paper points and obturated with gutta-percha and zinc oxide eugenol as sealer using lateral condensation technique and coronal access cavity were sealed with zinc oxide eugenol cement. Teeth were stored under 100% humidity at 37oC for 30 days to allow the sealer to set.
Endodontic Retreatment: The teeth were decoronated at the cementoenamel junction with a diamond disk to leave a root of 15mm in length and specimens were randomly divided into three experimental groups and a control group with 12 teeth each. The first 2-3mm of gutta percha was removed with Gates Glidden drill. A reservoir was created and deposited with a drop of xylene for 2min.
The tooth specimens are removed from the acrylic blocks and mounted in screw capped plastic vials.
Specimens in each group were retreated as follows:
Group 1 :- H-FILES (control group) 12 samples: Hand instrumentation was carried out with H files sizes 15-40 in crown down technique. H files are the most commonly used files for removing gutta-percha from the root canals.
Group 2:-Safe Sided H Files: Flutes on one side of H-file were blunted using a diamond disk and hand instrumentation was carried out with safe sided H files sizes 15-40 by circumferential filing. In order to prevent strip perforations, which is one of the many endodontic mishaps that may occur during the course of a retreatment procedure; safe sided H files were used as a part of the study.
Group 3:-Protaper Rotary Files: All the three Protaper Universal system retreatment files were used in crown down technique sequentially, until working length is reached. D1 Protaper file (0.09 taper, 300 rpm) was used to remove the filling material from the coronal third of the root canal. D2 Protaper file (0.08 taper, 300 rpm) was used in the coronal two thirds of the root canal. The D3 Protaper file (0.07 taper, 300rpm) was used with light apical pressure until the working length is reached and no further filling material was removed. Protaper retreatment rotary files have been proven to be one of the most popular and commonly used systems currently available in the market which was the reason behind its selection.
Group 4:-Ultrasonic Endodontic Retreatment Tip: Use of ultrasonics in retreatment is a fairly unexplored territory in Endodontics which is why ultrasonic endodontic retreatment tip E-7, E 3~ Max (0.6mm diameter at tip and 16mm length) was used for the removal of root canal filling material.
During retreatment root canals were irrigated with 1ml of 1% NaOCl for 10 secs then saline after each file use. Files were discarded after three uses. After instrumentation 1ml of 17% EDTA was applied for 1min and finally flushed with 1ml of 1% NaOCl for 10 secs.
Evaluation
1. The amount of remaining gutta-percha and sealer were evaluated. The roots were grooved and split longitudinally using a chisel after which the coronal, middle and apical thirds of the specimens were examined under stereo microscope 20 X magnification (Lieca MS 5, Germany). The specimens were photographed with a camera which was attached to stereomicroscope after which the images were evaluated using AUTOCAD software using a formula [Table/Fig-1].
Showing stereomicroscopic images of coronal, middle, apical thirds of the canal and AUTOCAD processing.
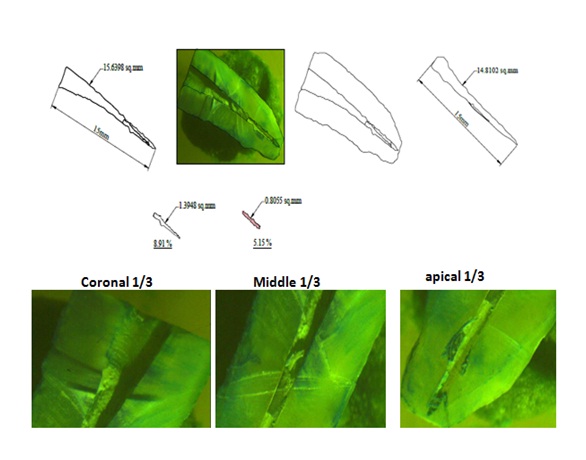
The percentage of volume of remaining filling material on canal walls was calculated with the following equation:

2. Using a stop watch the time duration from entering the root canal with file or engine driven instrument to the completion of re instrumentation was measured in seconds.
3. Immediately after instrumentation, the vials with collected debris were kept in hot air oven at 8000C for three days in order to evaporate the moisture to get dry debris. The weight of the debris was calculated in grams by subtracting weight of screw capped plastic vials before instrumentation from weight of screw capped plastic vials after instrumentation which was left after autoclaving.
Statistical Analysis
The data obtained was analyzed by using descriptive statistics, ANOVA (Analysis of Variance)-one way, ANOVA (Analysis of Variance)-two way and Scheffe’s post hoc test through SPSS for windows (v 16.0).
Results
1. Comparison of the mean % of gutta-percha remaining in the coronal 1/3rd region in the all groups: The mean scores of % of GP remaining in the coronal 1/3rd region using H files, safe H files, protaper retreatment rotary files, ultrasonic retreatment tips were 7.38, 9.31, 7.71,6.16% respectively [Table/Fig-2]. ANOVA showed significant differences between the groups i.e., 0.000 (p=0.05 or less). Ultrasonic retreatment tip has shown least % of GP remaining in the coronal 1/3rd region, followed by H files, protaper retreatment rotary files and safe sided H files [Table/Fig-3].
Comparison of the mean % of total root canal filling material remaining in the coronal, middle, apical and entire tooth among the four groups.
| GROUPS | CoronalMean ± SD | MiddleMean ± SD | ApicalMean ± SD | TotalMean ± SD |
|---|
| H files | 7.3808 ± 0.413 | 13.8175±0.565 | 15.7133±0.334 | 13.1942±0.201 |
| Safe sided H files | 9.3108 ± 0.302 | 15.6083±0.572 | 18.3067±0.597 | 15.5575±0.263 |
| Protaper retreatment files | 7.7125 ± 0.366 | 11.2858±0.493 | 13.8175±0.565 | 11.4200±0.343 |
| Ultrasonic retreatment tip | 6.1683 ± 0.334 | 7.3808± 0.413 | 14.2725±0.701 | 9.3108±0.302 |
| Statistical inference | F- Value=158.235 | 575.194 | 153.077 | 1055.018 |
| p- Value= 0.00 | 0.00 | 0.00 | 0.00 |
Test of significance *ANOVA test
Percentage of filling material debris found on the root canal walls after retreatment in coronal, middle and apical thirds.
Group 1-H files, Group 2- safe sided H files, Group3 – Protaper universal retreatment files and Group 4 – Ultrasonic retreatment tip
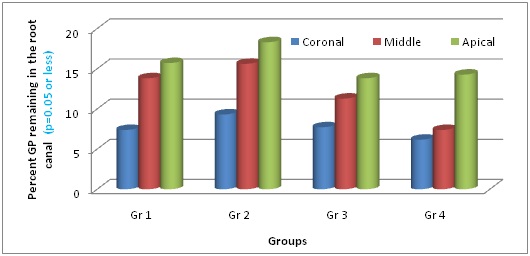
2. Comparison of the mean % of gutta-percha remaining in the middle 1/3rd region in the all groups: The mean scores of % of GP remaining in the middle 1/3rd region using H files, safe H files, protaper retreatment rotary files, ultrasonic retreatment tips were 13.8, 15.6, 11.2, 7.3% respectively [Table/Fig-2]. ANOVA showed significant differences between the groups i.e., (p=0.05 or less). Ultrasonic retreatment tip has shown least % of GP remaining in the middle 1/3rd region, followed by protaper retreatment rotary files, H files and safe sided H files [Table/Fig-3].
3. Comparison of the mean % of gutta-percha remaining in the apical 1/3rd region in the all groups: The mean scores of % of GP remaining in the apical 1/3rd region using H files, safe H files, protaper retreatment rotary files, ultrasonic retreatment tips were 15.7, 18.3, 13.8, 14.2% respectively [Table/Fig-2]. ANOVA showed significant differences between the groups i.e., (p=0.05 or less). protaper retreatment rotary files has shown least % of GP remaining in the apical 1/3rd region followed by Ultrasonic retreatment tip, H files and safe sided H files [Table/Fig-3].
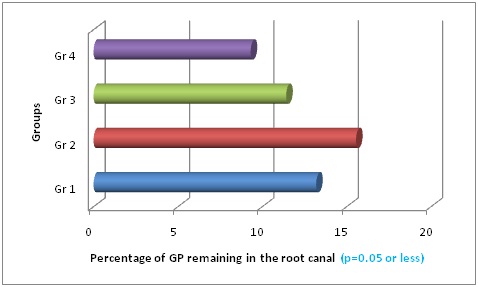
4. Comparison of the mean % of total gutta-percha remaining in the entire tooth in the all groups: The mean scores of % of GP remaining in the root canal using H files, safe H files, protaper retreatment rotary files, ultrasonic retreatment tips were 13.1, 15.5, 11.4, 9.3% respectively [Table/Fig-2]. ANOVA showed significant differences between the groups i.e., (p=0.05 or less). Ultrasonic retreatment tip has shown least % of GP remaining in total root canal, followed by protaper retreatment rotary files, H files and safe sided H files [Table/Fig-4].
Total percentage of filling material debris found on the root canal walls after retreatment.
Group 1-H files, Group 2- safe sided H files, Group3 – Protaper universal retreatment files and Group 4 – Ultrasonic retreatment tip
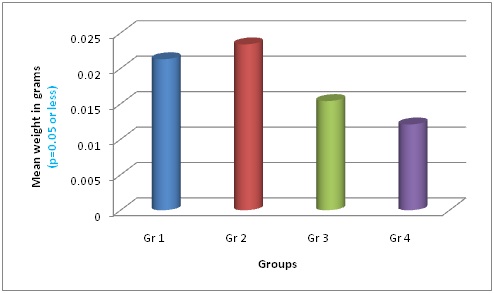
5. Comparison of the weight of apically extruded debris among all groups: The mean weight of apically extruded debris collected during retreatment using H files, safe H files, protaper retreatment rotary files, ultrasonic retreatment tips were 0.0215, 0.0234, 0.0154, 0.0121g respectively [Table/Fig-5]. ANOVA showed significant differences between the groups i.e., (p=0.05 or less). Ultrasonic retreatment tip has shown least apical debris extrusion, followed by protaper retreatment rotary files, H files and safe sided H files [Table/Fig-6].
Comparison of apically extruded debris in grams among the four groups.
| Groups | Mean weight of apical debris in gramsMean ± SD |
|---|
| H files | 0.0215±0.002 |
| Safe sided h files | 0.0234±0.00271 |
| Protaper retreatment files | 0.0154±0.00477 |
| Ultrasonic retreatment tip | 0.0121±0.00261 |
| Statistical inference | F- Value=78.975 |
| p-Value= 0.00 |
Test of significance *ANOVA test
Weight of apically extruded debris during retreatment.
Group 1-H files, Group 2- Safe sided H files, Group3 – Protaper universal retreatment files and Group 4 – Ultrasonic retreatment tip
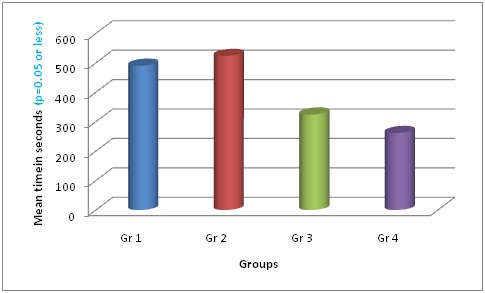
6. Comparison of the retreatment time among all groups: The mean retreatment time using H files, safe H files, protaper retreatment rotary files, ultrasonic retreatment tips were 490, 523, 324, 261sec respectively [Table/Fig-7]. ANOVA showed significant differences between the groups i.e., (p=0.05 or less). Ultrasonic retreatment tip has shown less time to remove root canal filling material, followed by protaper retreatment rotary files, H files and safe sided H files [Table/Fig-8].
Comparison of retreatment time in seconds among the four groups.
| Groups | Mean weight of apical debris in gramsMean ± SD |
|---|
| H files | 490.33 ±18.583 |
| Safe sided h files | 523.67 ±21.559 |
| Protaper retreatment files | 324.42 ±17.604 |
| Ultrasonic retreatment tip | 261.75 ±12.707 |
| Statistical inference | F- Value=602.787 |
| p-Value= 0.00 |
Test of significance *ANOVA test
Mean time for retreatment.
Group 1-H files, Group 2- Safe sided H files, Group3 – Protaper universal retreatment files and Group 4 – Ultrasonic retreatment tip
Discussion
The major goal of root canal treatment is to clean and shape the root canal system and seal it in three dimensions to prevent reinfection and retain the tooth with durable outcome. Although initial endodontic therapy has been shown with a high degree of predictable success, failures can also occur often due to various procedural and non procedural errors [5].
Compared to primary root canal therapy non-surgical retreatment procedure leads to more extrusion apically. When endodontic retreatment is performed, irritants in the form of filling materials, necrotic pulp tissues, bacteria or irrigants are introduced into the apical region. This leads to post operative pain and discomfort due to post operative inflammation and flare ups leading to failure of periapical healing [5].
An epidemiological study was done by Kvist T et al., to know the success of non surgical retreatment and surgical retreatment. There was no statistically significant difference between the success rate of surgical and for non surgical retreatment; the preferred treatment for failed endodontic cases is non surgical retreatment as surgical retreatment resulted in more postoperative discomfort, trauma to the normal oral tissues, post surgical complications [6].
In the present study samples were decoronated with a diamond disk to standardize the length 16mm to minimize variations by eliminating some variables, such as crown anatomy and root length, thus proving a reliable comparison of the proposed retreatment system [7, 8]. The teeth were mounted in an acrylic tube to simulate the periodontal ligament space and stability [9].
Gates Glidden drill (1-3size) was used in the present study to remove coronal 2mm of the canals. This step facilitates access to the more apical portions of canals and it provides a receptacle for the placement of the chemical solvent. The deep penetration with Gates Glidden drill would have removed the entire root filling material and even an extensive amount of surrounding root dentin which weaken the tooth and make it susceptible for future root fracture. Xylene was used as a solvent to remove gutta-percha filling from the root canal. According to Filho TM et al., xylene has better capacity of dissolution of gutta-percha [10, 11].
In the present study safe sided H files left the maximum amount of gutta-percha in the canals, produced more apical debris extrusion and took more time to remove filling material from the canals. This could be because of the cutting surface; cutting blades and the contact cutting surface were less. Hand instruments are stiffer than NiTi rotary instruments, cannot be directed effectively towards the root canal walls and don’t produce frictional heat leaving more amount in the root canals. The non cutting side on one side of the H file will lead to more debris accumulation. The push pull filing action of the safe sided H files acts as a piston, posing a risk of pumping the debris through the apical foramen [12].
Protaper showed good results in the apical thirds could be explained by the fact that the obturation is done with 40.02 master cone and D3 has 0.07 taper which is greater than the master apical file size. Therefore along the gutta-percha root filling material, the adjacent dentin wall also has been removed. This leads to the complete removal of root filling material. Rotary NiTi retreatment instrument used in the present study produced less apical debris extrusion than hand files; this could be because of triangular cross section of protaper retreatment files that reduces the area of contact between the instrument and the dentin walls. During the retreatment procedure, debris positioned between the apical blades and conveyed apically in the rotating instrument in auger like fashion, which helps to decrease the amount of the debris [12].
Ultrasonic instrument removed more material from the root canals within short period and produced very little extrusion. The ultrasonic vibration from the ultrasonic tip promoted the displacement of filling material from the root canal walls facilitating sealer removal and frictional heat produced by ultrasonic instrument causes synergistic effect on gutta-percha leading to softening and displacement of gutta-percha from the root canal [13].
Ultrasonics showed best results in coronal and middle thirds of the canal compared to apical thirds. This is because tip diameter of ultrasonic tip 0.6mm is more than the master apical file size and it has no cutting action on dentin.
Ultrasonic retreatment tip used in the present study produced little extrusion. When files are activated the filling material debris is displaced coronally resulting in less debris and the other reason could be the tip diameter of ultrasonic tip is more than the master apical file size [14]. So the tip is not reaching the apical area completely producing less apical debris extrusion. So the tip length and diameter could be a limitation of the study.
In the present study, in terms of retreatment time ultrasonics and protaper rotary retreatment files were faster than hand files. This is probably caused by the gutta-percha plasticization resulting from rotation of the rotary instrument and vibrations of the ultrasonic tip.
Softened guttapercha is less resistant to penetration of the instruments. This facilitates faster and easier removal of gutta-percha [15].
Limitation
1. The availability of the NSK ultrasonic tip length (16 mm) and diameter (0.6 mm) of the ultrasonic tip which corresponds to ISO size 60 K file are limitations as the apical preparation is usually finished at a much smaller size, especially for posterior teeth and generally the working length will be greater than 16mm.
2. Dentin removal and micro cracks formation in dentin during retreatment procedure will weaken the tooth structure non surgical retreatment is a less traumatic procedure to treat endodontic failures and ultrasonics proved to be an efficient method for the removal of gutta-percha.
Conclusion
Within the limitations of this in vitro study, it can be concluded that retreatment done using ultrasonic retreatment tip proved to be most effective, least time consuming and produced quantitatively lesser amount of apical debris extrusion followed by protaper rotary retreatment files, H files and safe sided H files. Under the experimental conditions, all four instruments proved to be helpful and safe devices for gutta percha removal in nonsurgical endodontic retreatment. All the systems left gutta percha or sealer remnants and fatigue effect on root canal walls.
Test of significance *ANOVA test
Test of significance *ANOVA test
Test of significance *ANOVA test